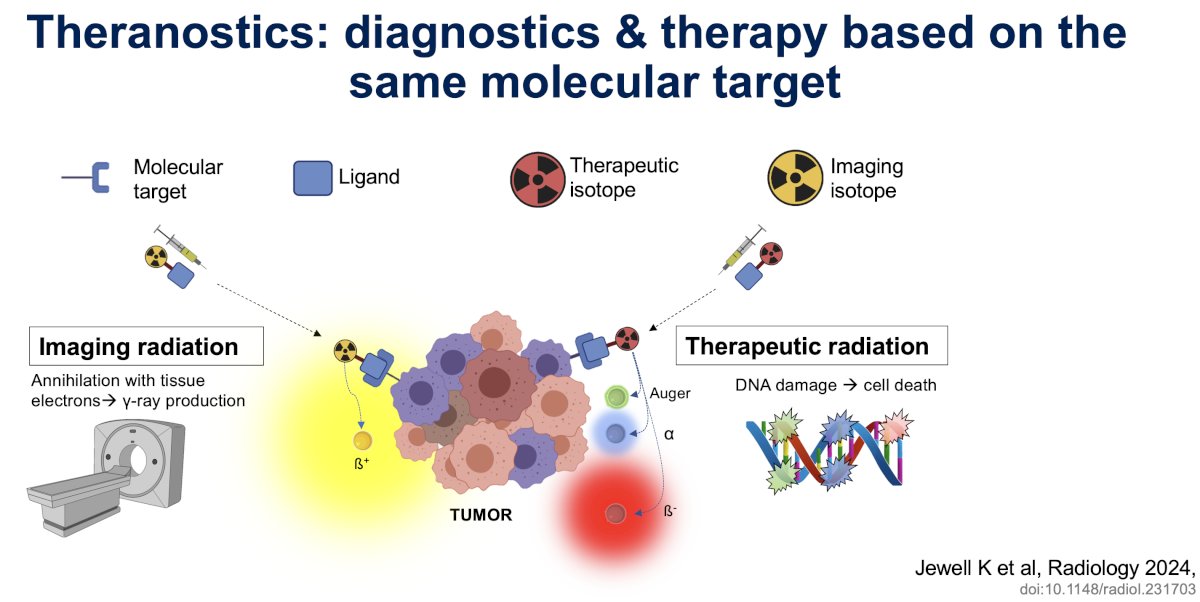
(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to a State of the Science session on novel diagnostics and therapeutics in renal cell and urothelial carcinomas. Dr. Michael Hofman presented an in-depth overview of the emerging diagnostic and therapeutic applications of functional imaging strategies in renal cell carcinoma (RCC).
Dr. Hofman began by noting that ‘theranostics have revolutionized prostate cancer care with PSMA…the next target (RCC) is now clear’. In the RCC space, the Carbonic Anhydrase 9 (CA-IX) receptor has emerged as a key theranostic target. Carbonic anhydrases are a superfamily of metalloenzymes present in all kingdoms of life that catalyze the conversion of CO2 to bicarbonate and proton. CA-IX is over-expressed in clear cell RCC and is a target ‘analogous’ to PSMA for prostate cancer.

The history of CA-IX ‘development’ is summarized below.
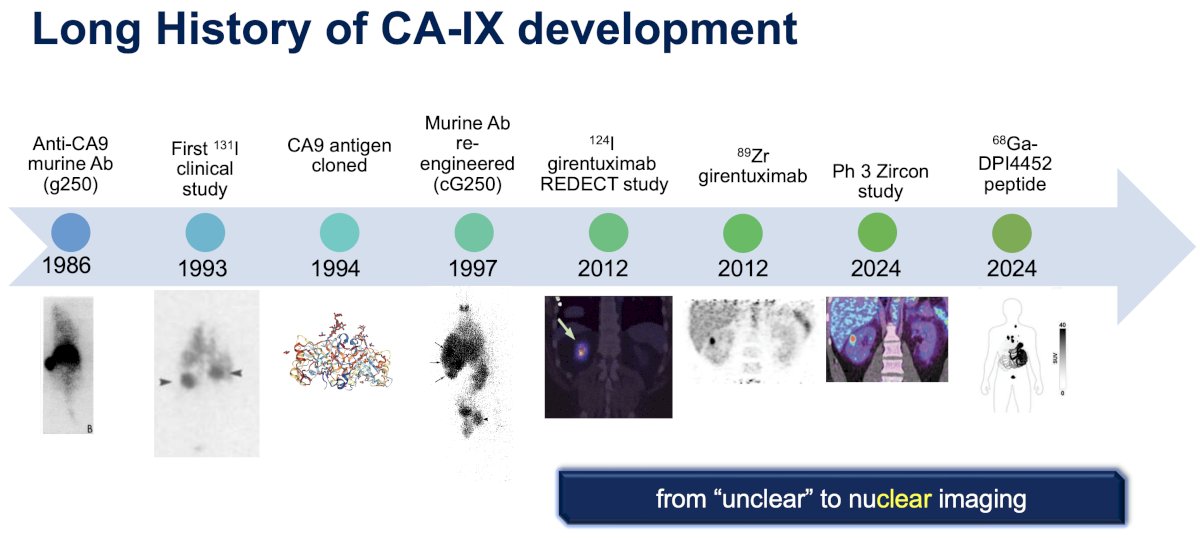
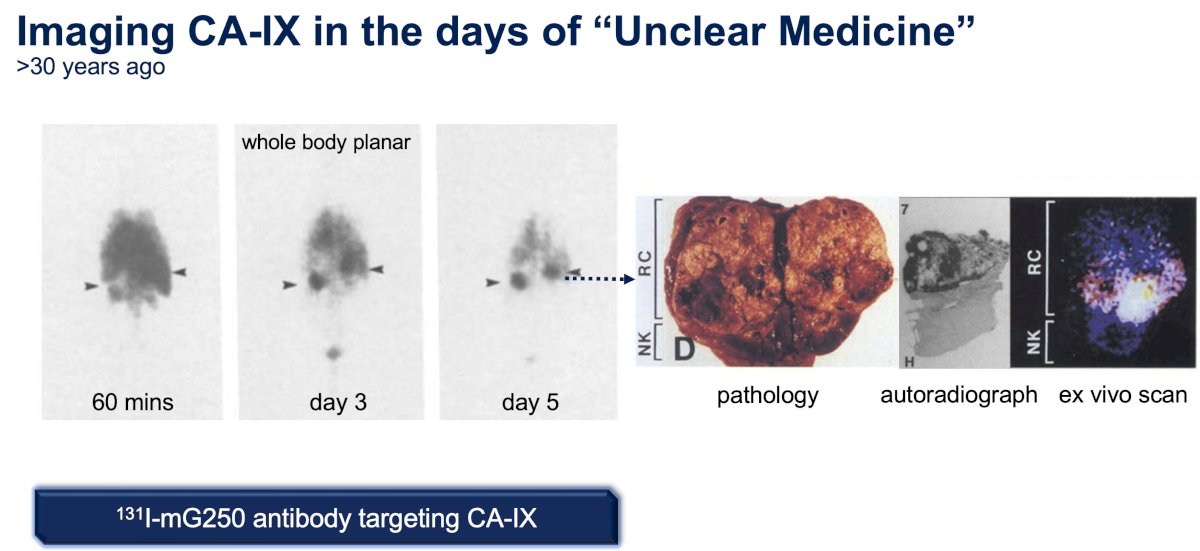
In 1986, the 1st anti-CA-IX murine antibody (g25) was developed.1
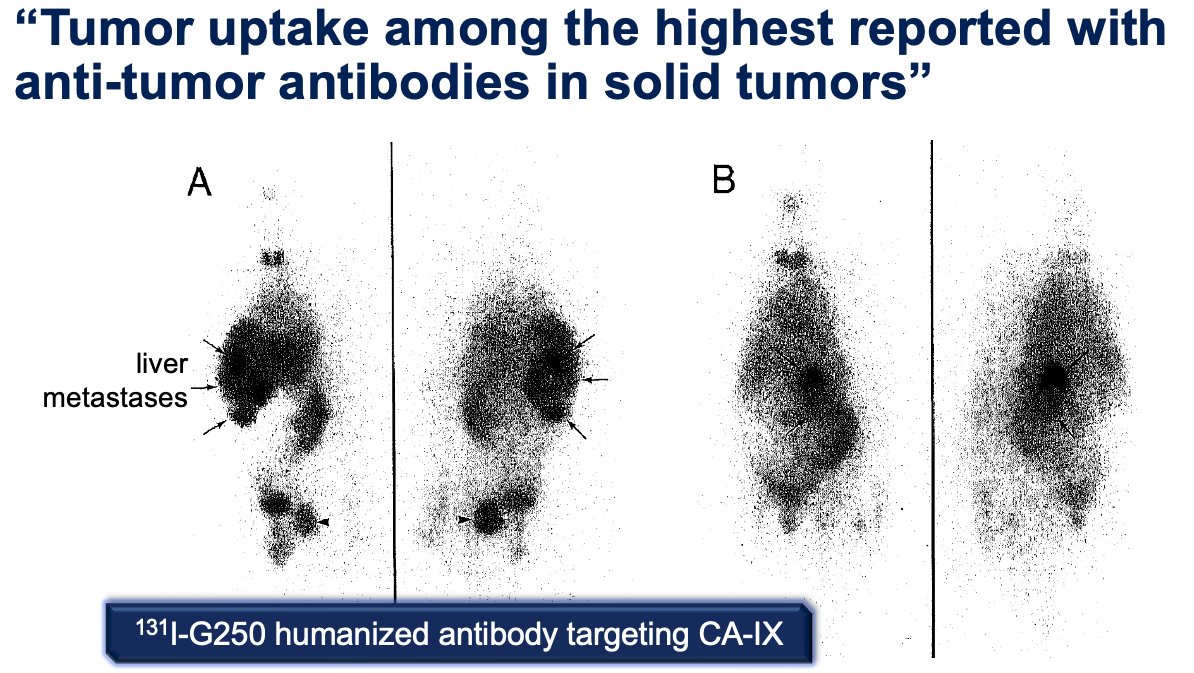
In 1994, the CA-IX antigen was cloned, and, in 1997, the 1st humanized antibody targeting CA-IX was developed.2
In 2012, 124I-girentuximab was evaluated in the REDECT trial, which was an open-label multicenter study of 124I-girentuximab PET/CT in patients with renal masses who were scheduled for resection. PET/CT and contrast-enhanced CT (CECT) of the abdomen were performed 2 to 6 days after intravenous 124I-girentuximab administration and before resection of the renal mass(es). The average sensitivity of PET/CT was 86% (versus 76% for CECT), and the specificity was 86% (versus 47% for CECT). This study represented the first clinical validation of a CAIX-targeting radiotracer for PET/CT imaging for the accurate and non-invasive identification of clear cell RCC.3

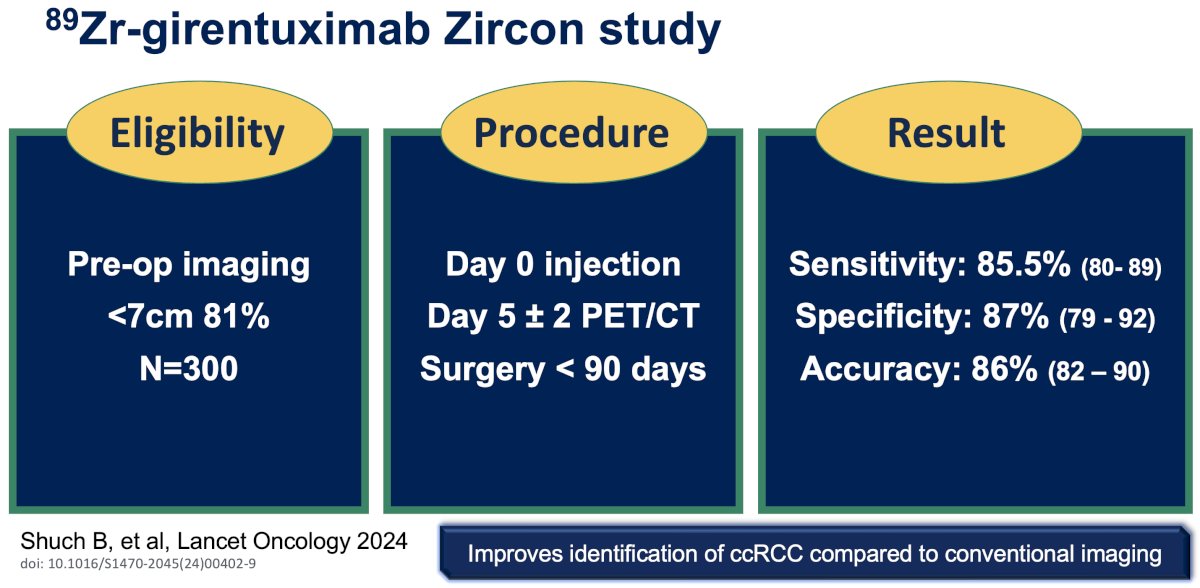
In 2024, the results of the phase III ZIRCON trial, which evaluated the diagnostic performance of 89Zr-DFO-girentuximab (TLX250-CDx) PET/CT, were published.4 ZIRCON was an open-label, multicenter clinical trial. Patients with indeterminate renal masses (≤ 7 cm; tumor stage cT1) who were scheduled for a partial or radical nephrectomy within 90 days of planned 89Zr-DFO-girentuximab administration were eligible. Enrolled patients received a single dose of 89Zr-DFO-girentuximab (37 MBq ± 10%; 10 mg girentuximab) on Day 0 and underwent PET/CT imaging on Day 5 (± 2 days) prior to surgery:
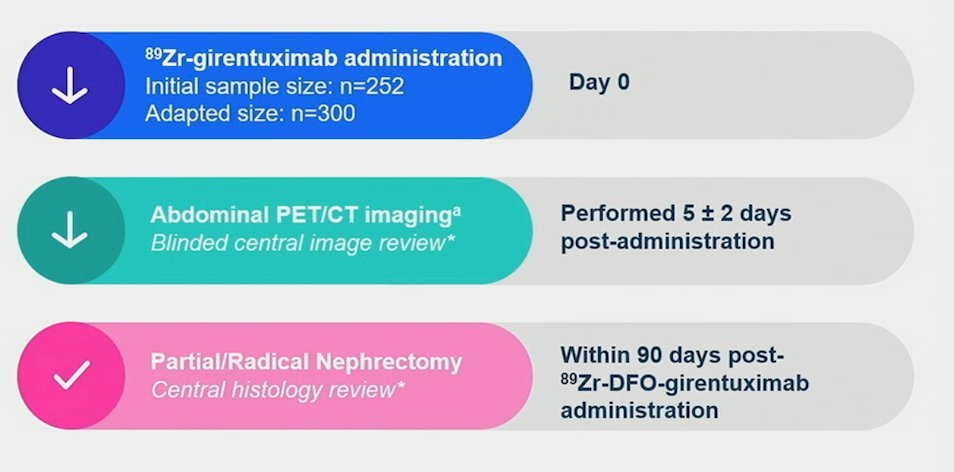
This imaging modality demonstrated:
- Sensitivity: 86%
- Specificity: 87%
- Positive predictive value: 91%
- Negative predictive value: 74%
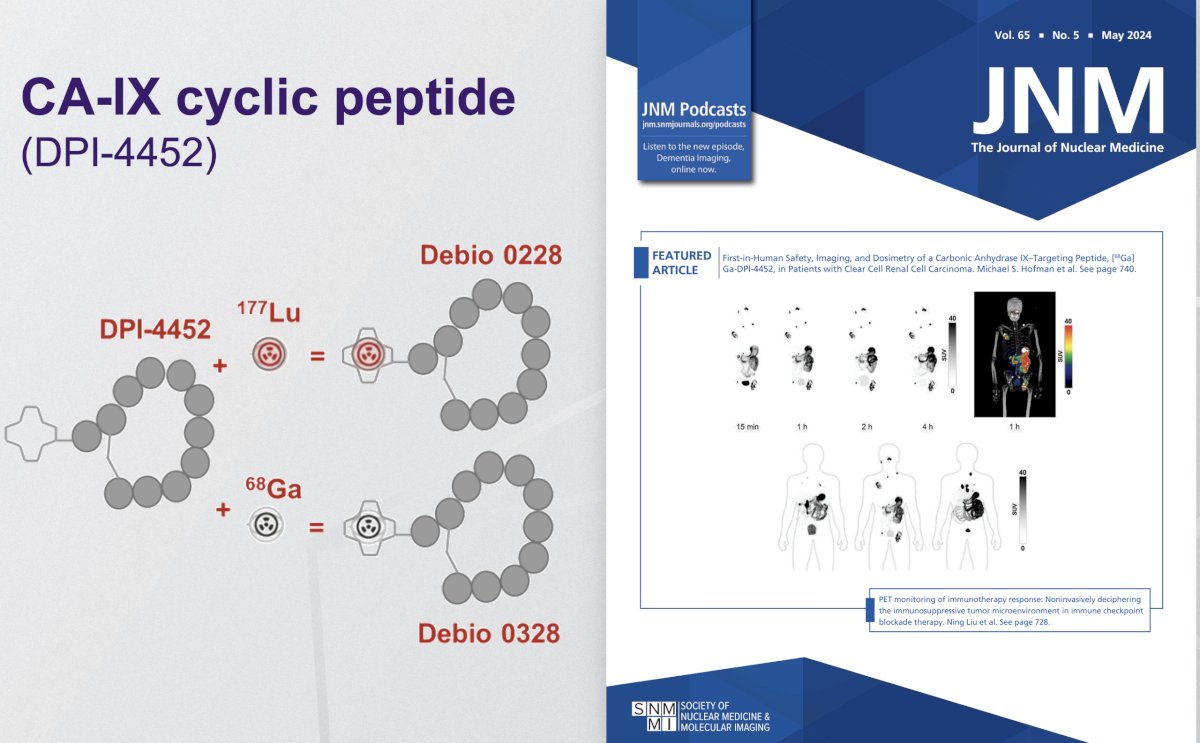
What about the CA-IX cyclic peptide, DPI-4452? [68Ga]Ga-DPI-4452, a first-in-class CA-IX-binding radiolabeled peptide, is the imaging agent of a theranostic pair with [177Lu]Lu-DPI-4452, developed for selecting and treating patients with carbonic anhydrase IX-expressing tumors. In their study published on the cover of The Journal of Nuclear Medicine in 2024, Dr. Hofman and colleagues assessed the imaging characteristics, dosimetry, pharmacokinetics, and safety of [68Ga]Ga-DPI-4452 in 3 patients with clear cell RCC.5
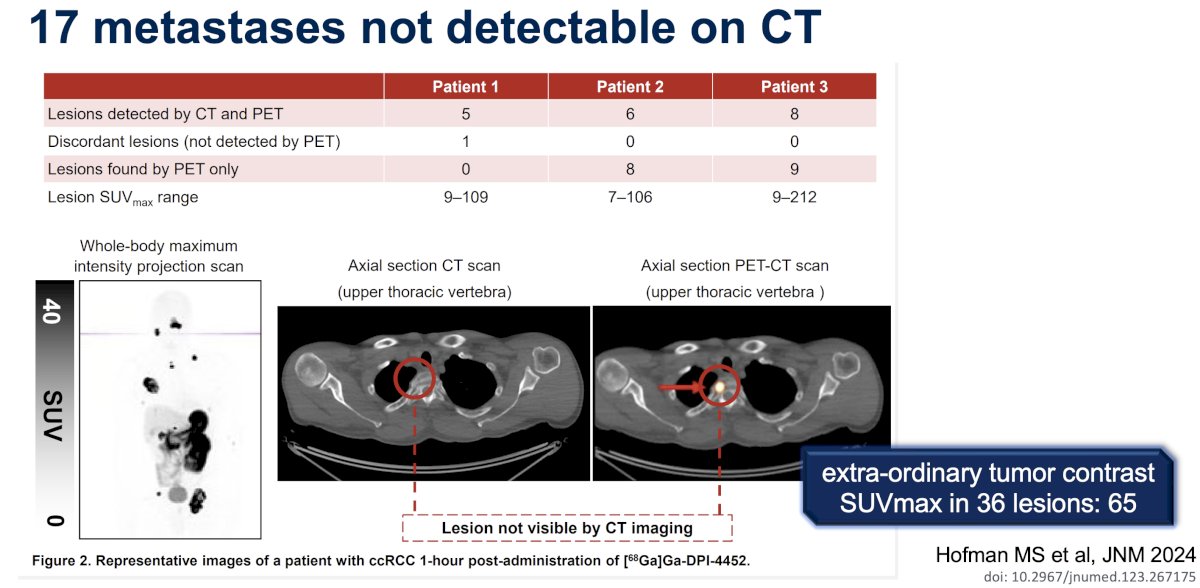
Tumor uptake was observed at all time points (15 min to 4 h). Across 36 lesions, the SUVmax one-hour post-administration ranged from 6.8 to 211.6 (mean: 64.6). The kidneys, liver, and bone marrow demonstrated low activity. [68Ga]Ga-DPI-4452 was rapidly eliminated from blood and urine. No clinically significant toxicity was observed. Dr. Hofman concluded that [68Ga]Ga-DPI-4452 showed exceptional tumor uptake in patients with clear cell RCC, with very high tumor-to-background ratios and no significant adverse events, suggesting potential diagnostic and patient selection applications. This target may also show promise for colorectal and pancreatic cancer, for which studies are currently underway.
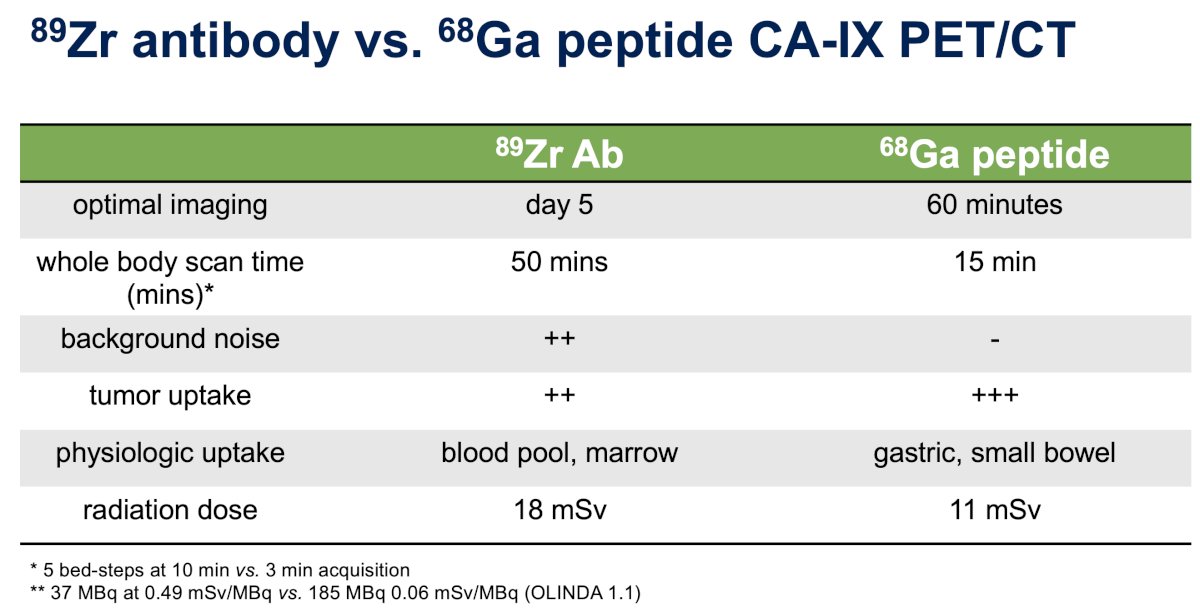
What are some notable differences between CA-IX-targeted 89Zr-antibody and 68Ga-peptide PET/CT imaging for clear cell RCC?

The optimal imaging window for 68Ga PET/CT imaging is much earlier (60 minutes versus 5 days) and requires much less time (15 versus 50 minutes). There is less background noise and improved tumor uptake. There is physiologic uptake of the 68Ga peptide in the gastric and small bowel cells. Significantly, the radiation dose is lower (11 mSv versus 18 mSv).
The ’natural’ next step is to leverage this into the theranostic space:
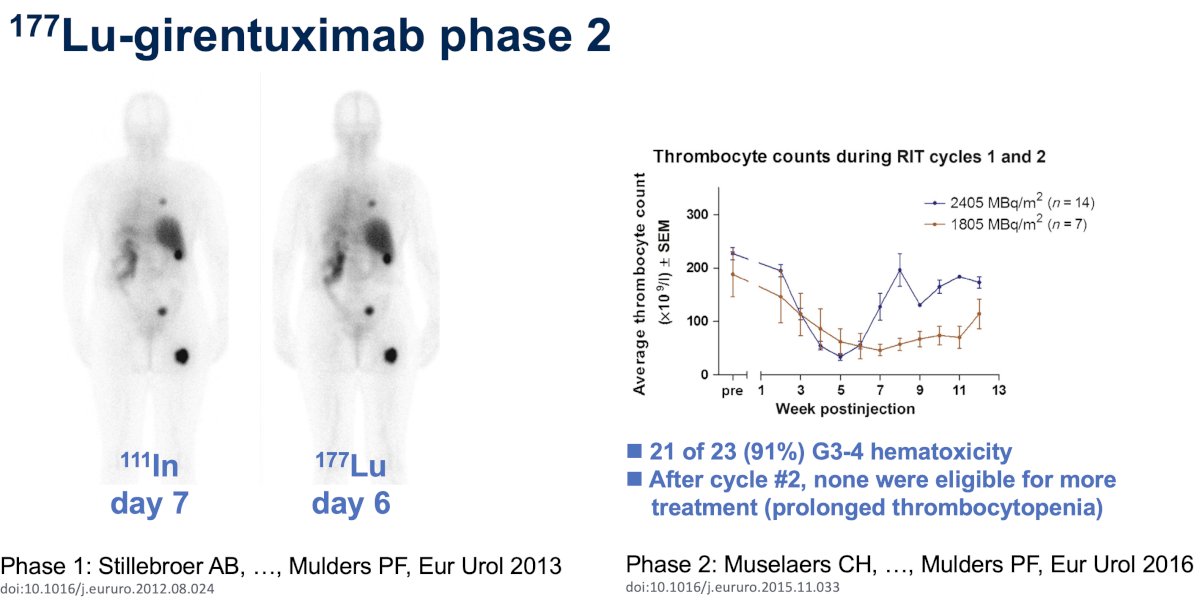
177Lu-girentuximab has been evaluated in a phase I study published by Stillebroer et al. in 2013.6 In a case series of 23 patients with progressive ccRCC metastases, they demonstrated that 177Lu-cG250 radioimmunotherapy is well-tolerated at an activity dose level as high as 2405 MBq/m2 and may stabilize previously progressive metastatic ccRCC.

In a subsequent phase II study published in 2016, Muselaers et al. evaluated 177Lu-girentuximab at a dose of 2405 MBq/m2 in a non-randomized single-arm trial of 14 patients with progressive metastatic ccRCC. In the absence of persistent toxicity and progressive disease, patients were eligible for retreatment after 3 months with 75% of the previous activity dose. After the first therapeutic infusion, eight patients (57%) had stable disease (SD) and one (7%) had a partial regression. The treatment was generally well tolerated but resulted in grade 3-4 myelotoxicity in most patients. After the second cycle, continued SD was observed in five of six patients, but none were eligible for retreatment due to prolonged thrombocytopenia.7
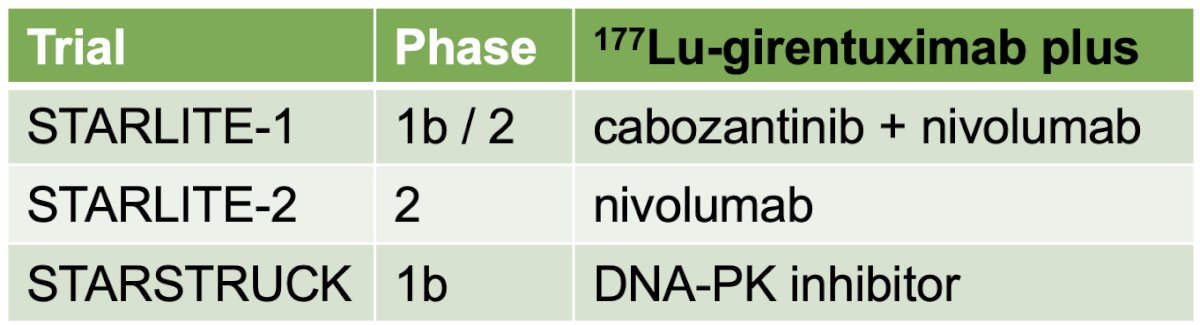
Despite these toxicity concerns, there are 3 ongoing trials evaluating 177Lu-girentuximab combination therapy in patients with metastatic ccRCC:
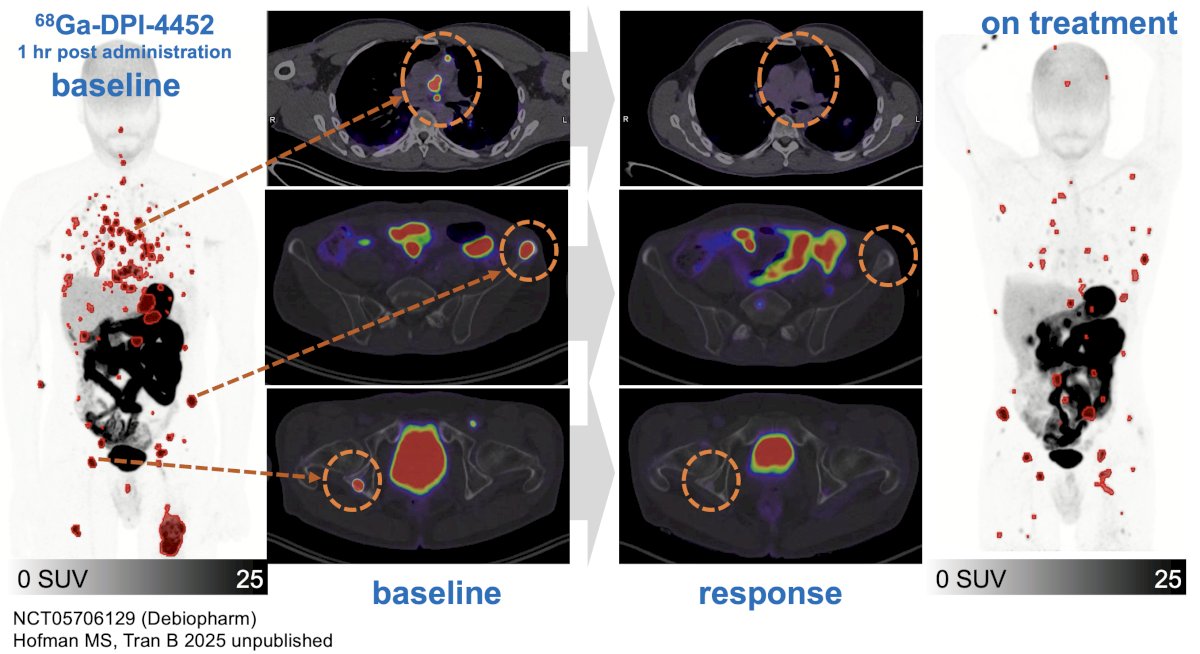
What about using DPI-4452 instead of girentuximab? In a yet unpublished phase I trial, Dr. Hofman and colleagues evaluated 3 cycles of 177Lu-DPI-4452 (10, 44, 66 mCi) in a metastatic RCC patient with positive findings on 68Ga-DPI-4452. An excellent treatment response was observed as illustrated below:
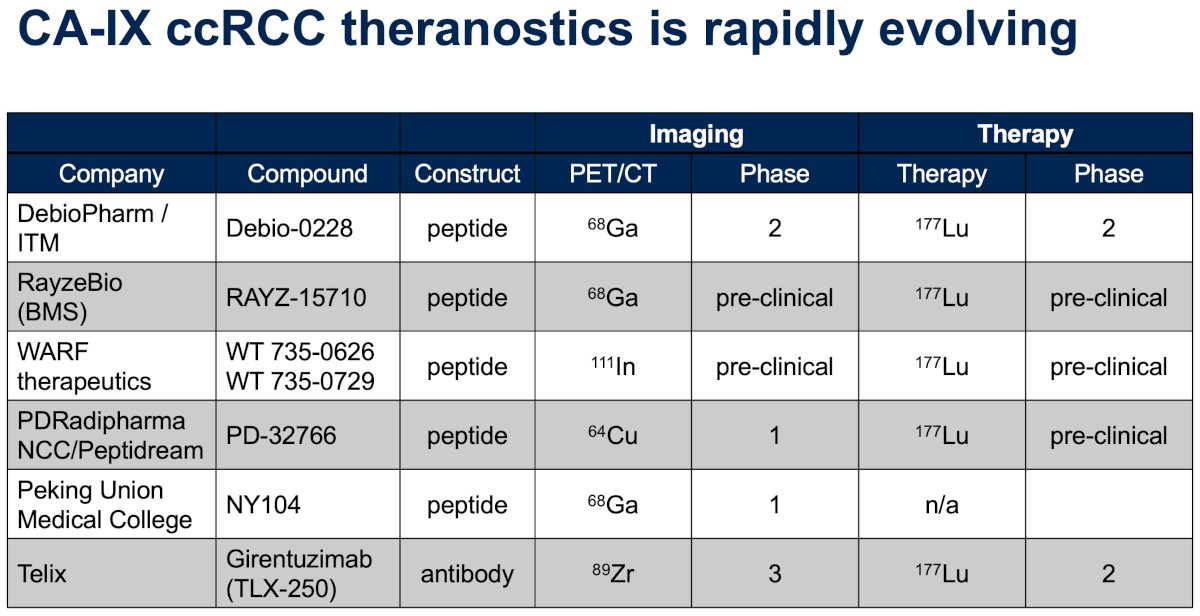
The CA-IX ccRCC theranostics space is rapidly evolving as summarized in the table below. However, to date, no radiolabeled C-IX theranostic agent has been approved yet.
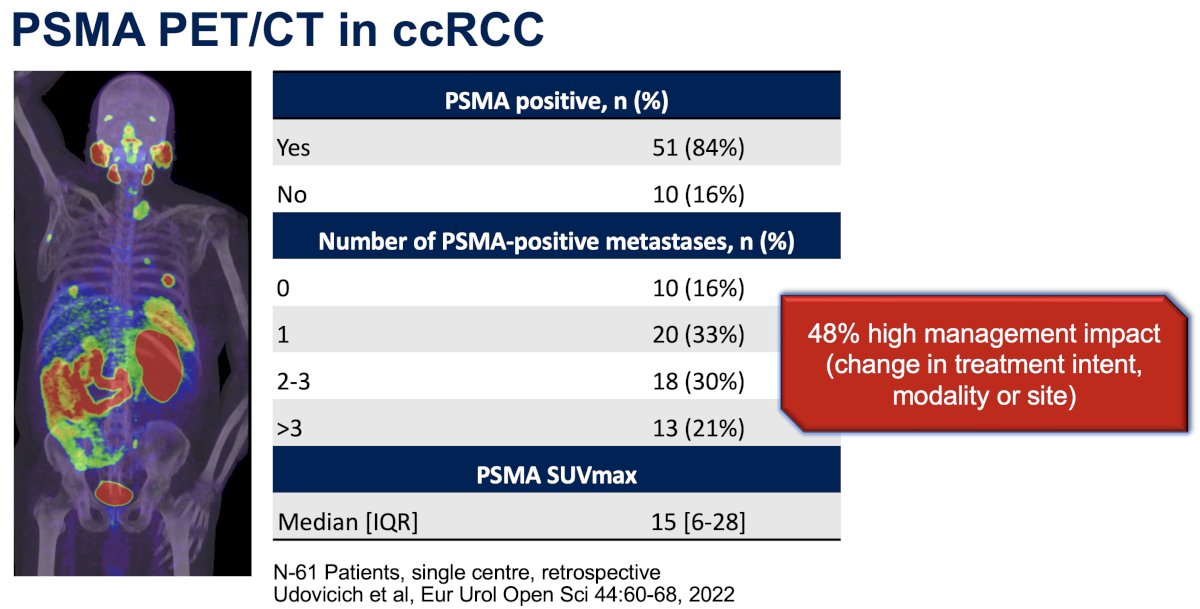
What about PSMA PET in ccRCC? In 2022, Dr. Hofman’s group published a retrospective review of 54 patients who underwent PSMA PET/CT from 2014 to 2020 for restaging or suspected metastatic ccRCC in a tertiary academic setting. Of the 54 patients, 51 (84%) had PSMA-positive disease. Notably, there was a ‘high impact’ change in management due to PSMA PET/CT findings in 48% of patients.8
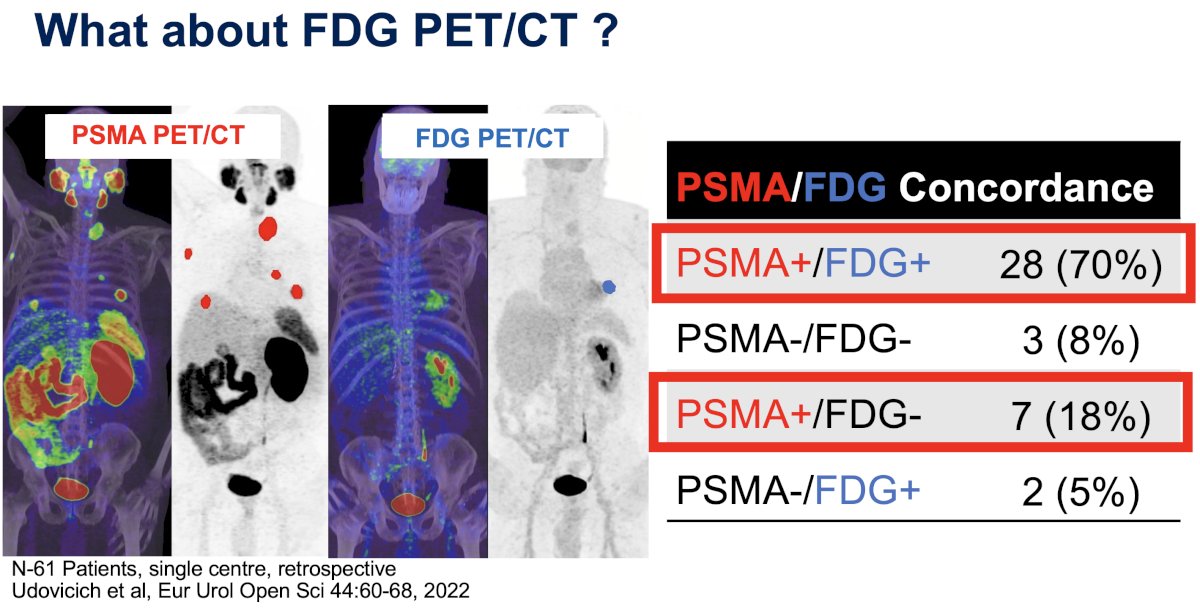
What about FDG PET/CT? Concordant PSMA and FDG PET/CT findings were observed in 705 of cases; however, PSMA+ and FDG- discordant findings were observed in 18%, highlighting the limitations of FDG PET/CT in this setting.8
Despite these limitations, numerous studies have demonstrated that FDG PET/CT in this setting is of prognostic value for survival outcomes, whereby patients who are FDG PET+ have worse survival outcomes.9
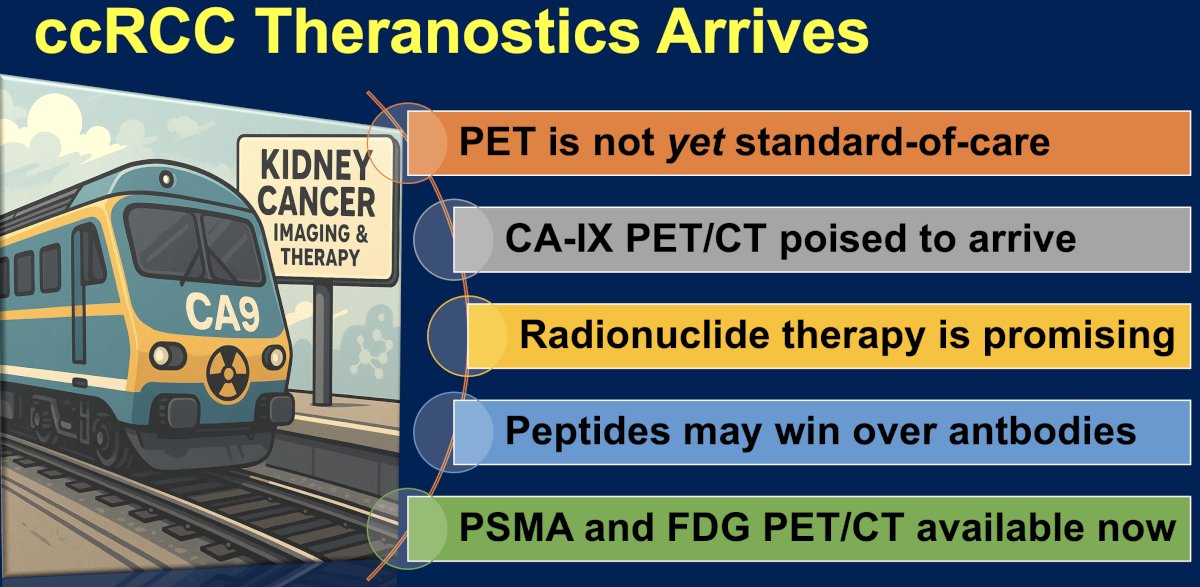
Dr. Hofman concluded his presentation of theranostics in the ccRCC space as follows:
Presented by: Michael Hofman, MBBS, FRACP, FAANMS, FICIS, GAICD, Prostate Cancer Theranostics and Imaging Centre of Excellence, Peter MacCallum Cancer Center, Melbourne, Australia
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:
- Oosterwijk E, Bander NH, Divgi CR, et al. Antibody localization in human renal cell carcinoma: clinicopathologic correlations. J Clin Oncol. 1993;11(4):738–50.
- Steffens MG, Boerman OC, Oosterwijk E, et al. Targeting of renal cell carcinoma with iodine-131-labeled chimeric monoclonal antibody G250. J Clin Oncol. 1997;15(4):1529–37.
- Divgi CR, Uzzo RG, Gatsonis C, et al. Positron emission tomography/computed tomography identification of clear cell renal cell carcinoma: results from the REDECT trial. J Clin Oncol. 2013;31(2):187-94.
- Shuch B, Pantuck AJ, Bernhard J-C, et al. [89Zr]Zr-girentuximab for PET–CT imaging of clear-cell renal cell carcinoma: a prospective, open-label, multicentre, phase 3 trial. Lancet Oncol. 2024;25(10):e1234–45.
- Hofman MS, Tran B, Feldman DR, et al. First-in-human safety, imaging, and dosimetry of a carbonic anhydrase IX–targeting peptide, [68Ga]Ga-DPI-4452, in patients with clear cell renal cell carcinoma. J Nucl Med. 2024;65(5):740–743.
- Stillebroer AB, Boerman OC, Desar IME, et al. Phase 1 radioimmunotherapy study with lutetium 177-labeled anti-carbonic anhydrase IX monoclonal antibody girentuximab in patients with advanced renal cell carcinoma. Eur Urol. 2013;64(3):478–485.
- Stillebroer AB, Boerman OC, Desar IME, et al. Phase 1 radioimmunotherapy study with lutetium 177-labeled anti-carbonic anhydrase IX monoclonal antibody girentuximab in patients with advanced renal cell carcinoma. Eur Urol. 2013;64(3):478–485.
- Udovicich C, Callahan J, Bressel M, Ong WL, Perera M, Tran B, et al. Impact of prostate-specific membrane antigen positron emission tomography/computed tomography in the management of oligometastatic renal cell carcinoma. Eur Urol Open Sci. 2022;44:60–68.
- Udovicich C, Callahan J, Bressel M, et al. FDG-PET positivity and overall survival in renal cell carcinoma. JAMA Netw Open. 2022;5(11):e2240577.