(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30 and June 3 was host to the Poster Session: Genitourinary Cancer - Kidney and Bladder. Dr. Hal Difede Rives presented Poster 4576: Assessing treatment outcomes of enfortumab vedotin dose reduction in metastatic bladder cancer.
Enfortumab vedotin (EV), an antibody-drug conjugate targeting Nectin-4, has become a first-line treatment option for advanced urothelial carcinoma (UC) when administered in combination with pembrolizumab, an anti–PD-1 immune checkpoint inhibitor. While the combination demonstrates strong clinical efficacy, EV is associated with both acute and cumulative toxicities that can adversely impact patients' quality of life.1 Treatment-related adverse events (TRAEs) are frequently managed through dose reductions and schedule modifications. Currently, treatment is continued until disease progression or the development of unacceptable toxicity. This single-center retrospective study assessed the impact of EV dose reductions on treatment duration, the incidence of adverse events, and survival outcomes in patients with advanced UC.
Patients were stratified into three groups based on EV dosing:
- Group A: Received 1.25 mg/kg with no dose reductions
- Group B: Started at 1.25 mg/kg with subsequent dose reductions
- Group C: Received <1.25 mg/kg from the outset
Clinical data were extracted from the electronic medical record (EMR). Outcomes evaluated included overall survival (OS), progression-free survival (PFS), treatment-related adverse events (TRAEs), and the number of EV doses received.
Kaplan-Meier and Cox proportional hazards regression models were used to compare PFS and OS across the three dosing groups. Additionally, EV dose (1.25 mg/kg vs. <1.25 mg/kg) was modeled as a time-varying covariate. TRAEs (yes/no) and the total number of doses received were analyzed using logistic regression and negative binomial regression, respectively. All regression models were adjusted for age, ECOG performance status, and concurrent use of pembrolizumab.
A total of 153 patients with urothelial carcinoma treated with EV were included in this analysis and categorized into three dosing groups: Group A (n=47), Group B (n=73), and Group C (n=33). The overall cohort was predominantly male (78.4%) and white (79.1%), with no significant demographic differences across groups.
Patients in Group C were older and had higher baseline ECOG performance status, with median age and ECOG score both significantly elevated compared to Groups A and B (p<0.001 and p=0.033, respectively). Prior immunotherapy had been received by 52.9% of patients, and 35.9% were treated with concurrent pembrolizumab, similar across all groups.
Patients in Group B, who began treatment at full dose and later required reduction, experienced a higher incidence of treatment-related adverse events (TRAEs), particularly neuropathy and cutaneous toxicity. Neuropathy rates were 15.2%, 34.2%, and 12.1% in Groups A, B, and C, respectively (p<0.001); cutaneous AEs occurred in 4.3%, 27.4%, and 2.1,% respectively (p=0.004).
In unadjusted Kaplan-Meier analyses, there was a trend toward improved outcomes in Groups B and C, but no statistically significant differences in progression-free survival (PFS: A 6.4 mo, B 10.1 mo, C 13.1 mo; p=0.10) or overall survival (OS: A 10.5 mo, B 15.6 mo, C 22.9 mo; p=0.22). After adjusting for confounders in patients who received a minimum of five EV doses, there was no significant difference in the total number of doses administered across groups (p=0.6867).
Adjusted Cox proportional hazards regression demonstrated significantly improved PFS and OS for patients receiving <1.25 mg/kg dosing, both in landmark and time-varying analyses. Specifically, in time-varying covariate models, lower-dose EV was associated with a hazard ratio of 0.48 for PFS (p=0.019) and 0.53 for OS (p=0.038) as shown in the Table below.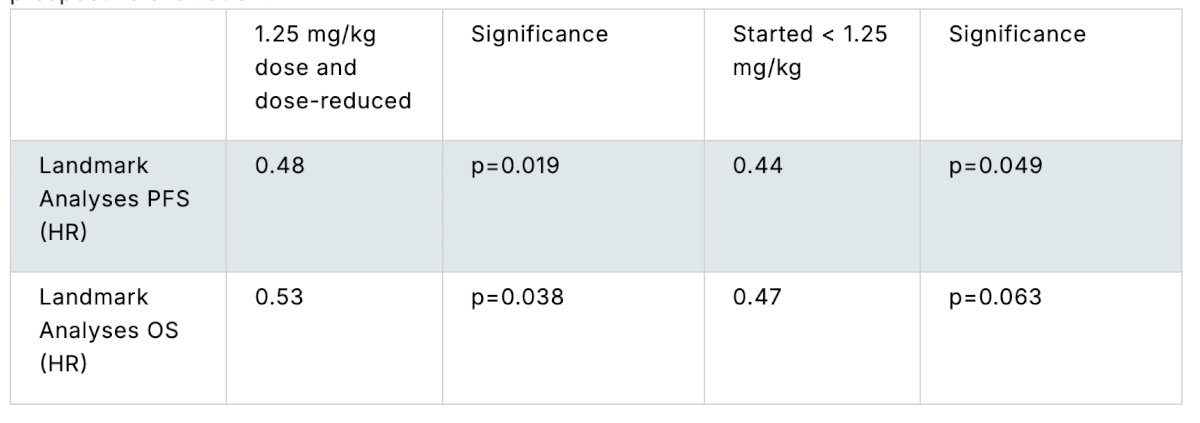
Dr. Difede Rives concluded with the following key messages:
- Adjusted analyses demonstrated significantly improved progression-free survival and overall survival in the dose-reduced groups.
- These findings suggest that EV dose reductions may reduce overall treatment-related adverse events without compromising clinical efficacy.
- The results support the need for prospective studies to further evaluate the impact of dose modification strategies in patients receiving EV-based therapy.
Presented by: Hal Difede Rives, BS, The Fox Chase Cancer Center Foundation. Philadelphia, PA.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Reference:
- Powles T, Valderrama BP, Gupta S, Bedke J, Kikuchi E, Hoffman-Censits J, Iyer G, Vulsteke C, Park SH, Shin SJ, Castellano D, Fornarini G, Li JR, Gümüş M, Mar N, Loriot Y, Fléchon A, Duran I, Drakaki A, Narayanan S, Yu X, Gorla S, Homet Moreno B, van der Heijden MS; EV-302 Trial Investigators. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N Engl J Med. 2024 Mar 7;390(10):875-888. doi: 10.1056/NEJMoa2312117. PMID: 38446675.