(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30 and June 3 was host to the Poster Session: Genitourinary Cancer - Kidney and Bladder. Dr. Brendan Raizenne presented Poster 4578: Prognostic utility of ctDNA before and after trimodality therapy (TMT) for muscle invasive bladder cancer
Dr. Raizenne opened the presentation by highlighting that trimodality therapy (TMT) has emerged as a curative option for select patients with muscle-invasive bladder cancer (MIBC).1 However, there remains a critical lack of predictive clinical factors or biomarkers to identify patients at higher risk of progression and to guide the need for adjuvant or neoadjuvant treatment intensification in this setting.
The investigators evaluated the clinical utility of a circulating tumor DNA (ctDNA) assay in predicting treatment outcomes following TMT. Using a retrospective approach, they leveraged the institutional database at the University of California, San Francisco (UCSF) to identify patients with MIBC (cT2–T4, cN0–N2, cM0–M1a) who underwent definitive TMT between 2022 and 2024 and had at least one ctDNA measurement obtained during the course of treatment. The Signatera ctDNA assay with whole exome sequencing (WES) was used to measure ctDNA.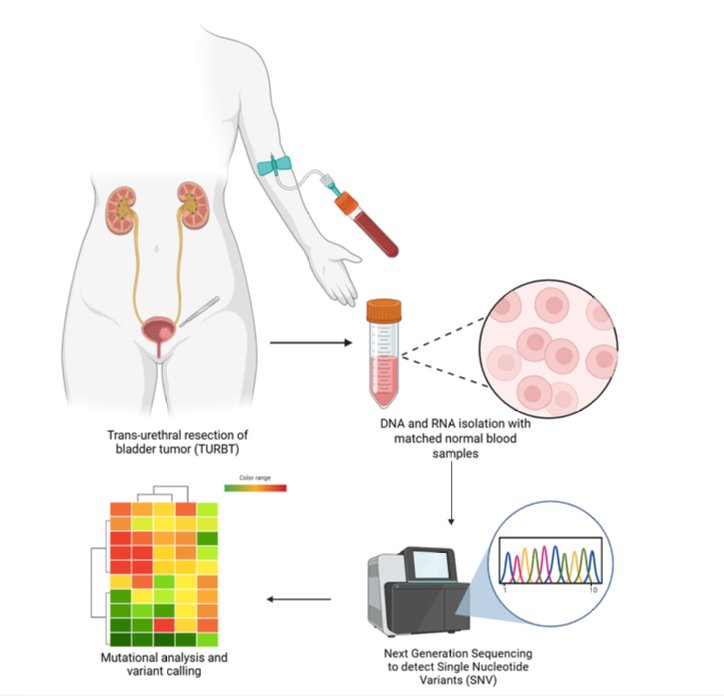
The primary endpoint was disease-free survival (DFS), measured beginning three months after the final dose of radiation and analyzed using the Kaplan-Meier method. Predictors of disease recurrence were assessed using Cox proportional hazards models.
Baseline characteristics of the cohort are summarized below. A total of 34 patients who underwent TMT were included in the analysis. The median age was 69 years, and the majority were male (91%). Most patients (65%) had pure urothelial carcinoma histology. Notably, 38% of patients received elective pelvic nodal radiation as part of their treatment regimen.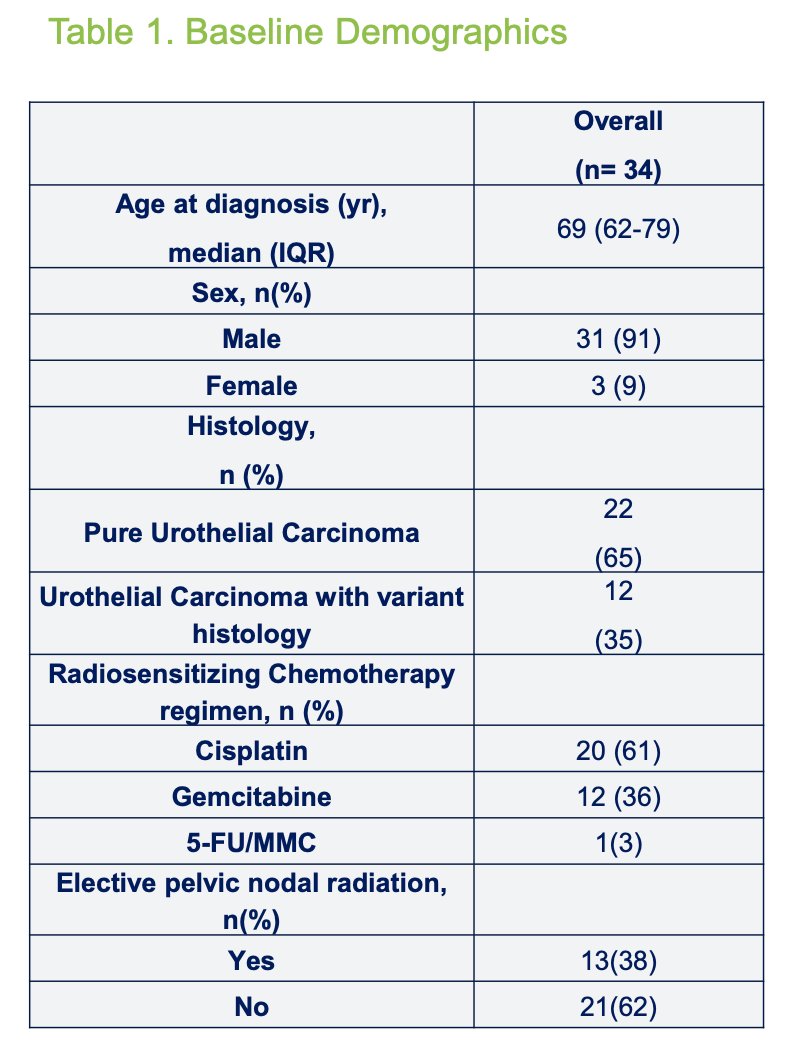
Among patients who experienced disease recurrence, 62% presented with distant metastases and/or nodal recurrence and subsequently received systemic therapy. Notably, all patients with distant recurrence had detectable ctDNA at the time of recurrence.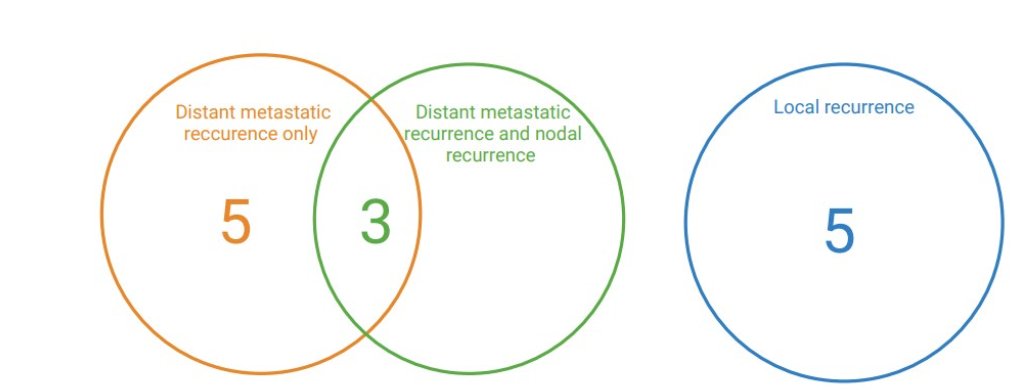
Of the 20 patients who underwent ctDNA testing prior to initiating TMT, 10 (50%) had detectable ctDNA, with a median concentration of 4.5 MTM/mL (IQR: 0.31–9.03 MTM/mL). Among these patients, those who converted to an undetectable ctDNA status following TMT (n=7) demonstrated the most favorable outcomes, with a median DFS of 20 months. In contrast, patients who remained ctDNA-positive after TMT had the poorest prognosis, with a median DFS of just 5 months (log-rank p=0.093). Notably, no patients converted from undetectable to detectable ctDNA following treatment.
Moreover, among patients who received elective pelvic nodal irradiation (ENI), the median DFS was not reached, compared to a median DFS of 7.6 months in patients with detectable ctDNA prior to TMT who did not receive ENI. However, this difference did not reach statistical significance (p=0.20).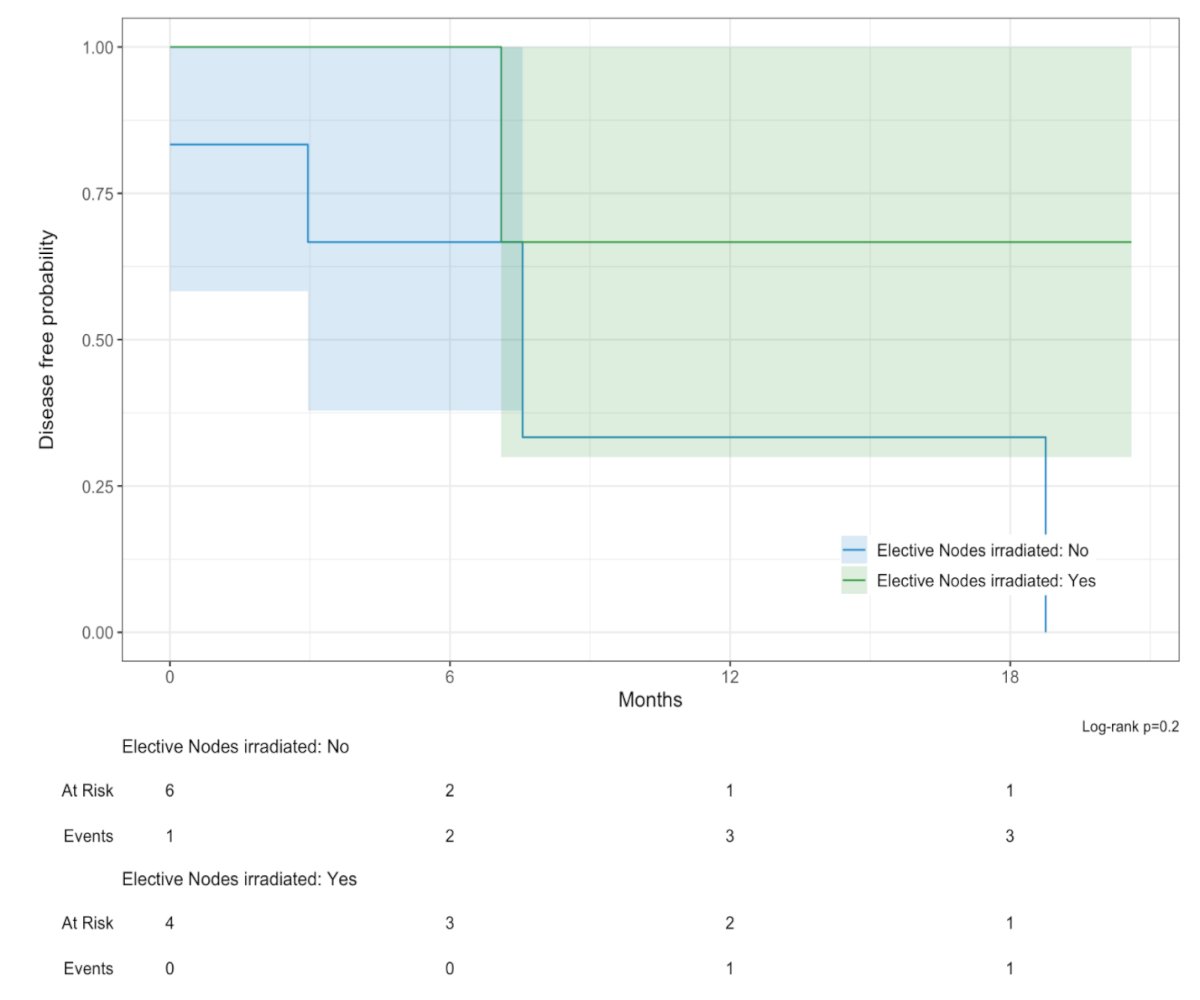
Dr. Raizenne noted that whole-exome sequencing analysis of 18 patients revealed TP53 (61%), ARID1A (39%), and RB1 (33%) as the most frequently mutated genes. Additionally, 11 patients (61%) had alterations in DNA damage repair genes, including BRCA1, BRCA2, ATM, and ERCC2 as illustrated below.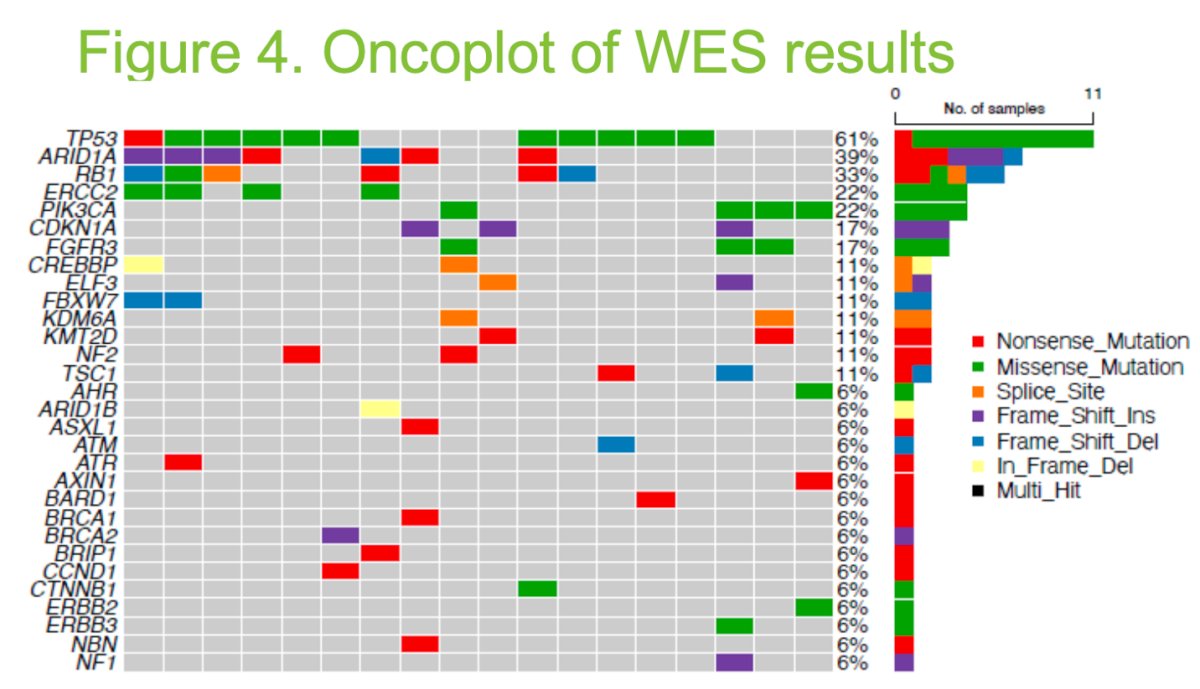
Dr. Raizenne concluded the presentation with the following key messages:
- Most patients with detectable ctDNA prior to trimodality therapy converted to undetectable ctDNA following treatment.
- Persistently positive ctDNA after TMT was associated with worse prognosis in patients with MIBC
- These findings support the potential role of ctDNA as a prognostic biomarker to guide post-TMT surveillance and treatment strategies.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Reference: