(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a kidney and bladder cancers poster session. Dr. Joshua Meeks presented the ongoing TroFuse-027 study, a phase I/II trial of intravesical sacituzumab tirumotecan in participants with intermediate-risk non–muscle-invasive bladder cancer (NMIBC).
The standard treatment for patients with intermediate-risk (IR) NMIBC is transurethral resection of bladder tumor (TURBT) with either adjuvant intravesical (I-VESIC) chemotherapy or bacillus Calmette-Guérin.1 Despite treatment, the rates of disease recurrence are high,2,3 and novel therapies with favorable efficacy and safety profiles are urgently needed.
Trophoblast cell-surface antigen 2 (TROP2) is a transmembrane glycoprotein expressed broadly in several tumor types, including bladder,4,5 making it a viable therapeutic target. Systemic TROP2 inhibitors have demonstrated efficacy and a manageable safety profile in participants with metastatic urothelial carcinoma previously treated with platinum-, immune-, or checkpoint inhibitor-based therapies when administered alone6,7 or in combination with pembrolizumab8 or enfortumab.9
Sacituzumab tirumotecan (sac-TMT; MK-2870/SKB264) is an antibody-drug conjugate (ADC) consisting of 3 major components: 1) a TROP2-targeting monoclonal antibody, sacituzumab; 2) a cytotoxic payload from the topoisomerase 1 inhibitor class; and 3) a novel, irreversible but hydrolysable linker, which joins the monoclonal antibody and the cytotoxic payload, leveraging proprietary linker conjugation technology.10 In in vivo NMIBC mouse models, intravesical sac TMT was shown to have antitumor activity, tolerability, and minimal systemic exposure.
TroFuse-027 (NCT06637423) is a nonrandomized, open-label, phase 1/2 study designed to evaluate the safety and efficacy of I-VESIC sac-TMT monotherapy as ablative therapy in participants with intermediate-risk NMIBC.
The study design is illustrated below:
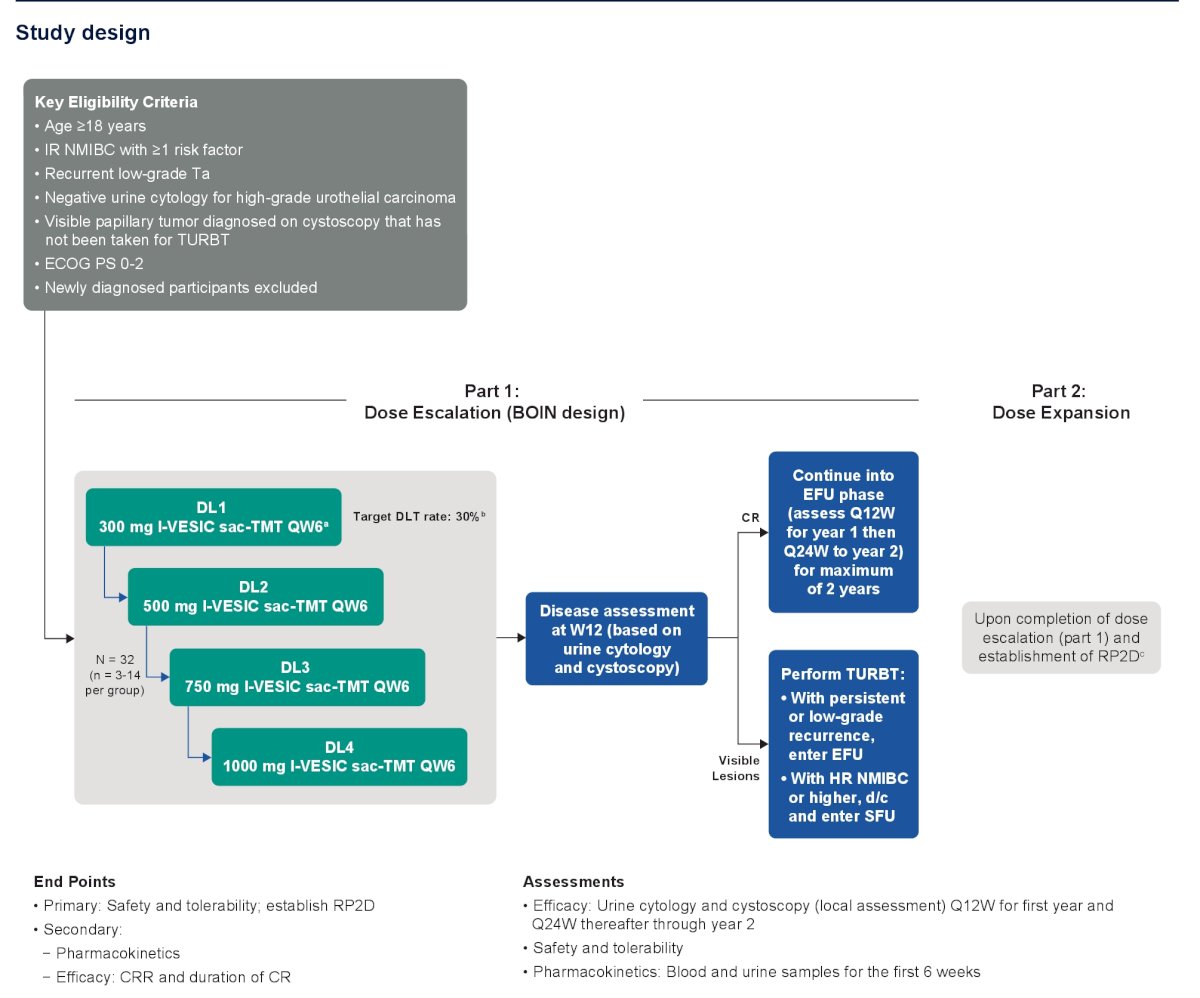
This trial will include adult patients with IR, recurrent, low-grade Ta with visible papillary tumor visible on cystoscopy, but not resected on TURBT. In the Part 1 dose escalation portion, increasing I-VESIC sac-TMT doses from 300 to 1,000 mg will be evaluated. The target dose-limiting toxicity (DLT) rate is 30%.
All patients will undergo disease assessment at 12 weeks (cystoscopy + urine cytology). Those with a complete response will proceed into the efficacy follow-up (EFU) phase. Conversely, those with visible lesions will be recommended for a TURBT. If this represents disease persistence of low-grade recurrence, then patients enter EFU. Conversely, those with HR NMIBC or worse disease enter the survival follow-up (SFU) phase.
The Part 2 dose expansion portion begins upon completion of the dose escalation (Part 1) portion and establishment of a recommended phase 2 dose (RP2D).
The primary endpoints are:
- Safety and tolerability
- Establish RP2D
The secondary endpoints are:
- Pharmacokinetics
- Efficacy: Complete response rate; duration of complete response
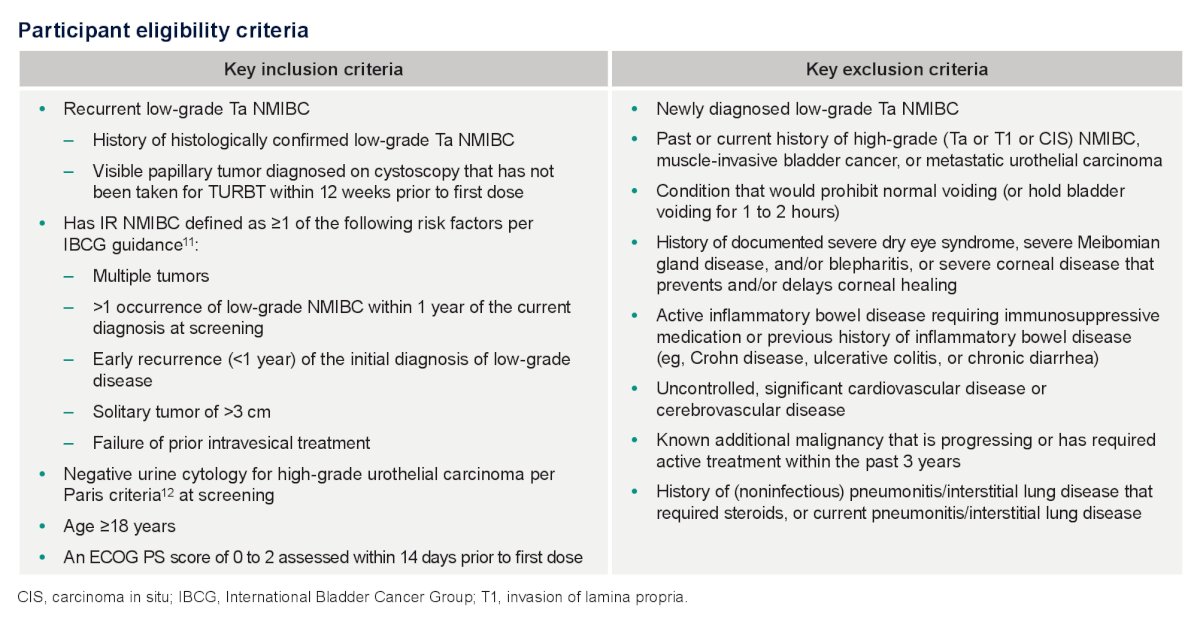
The full participant eligibility criteria are summarized below:
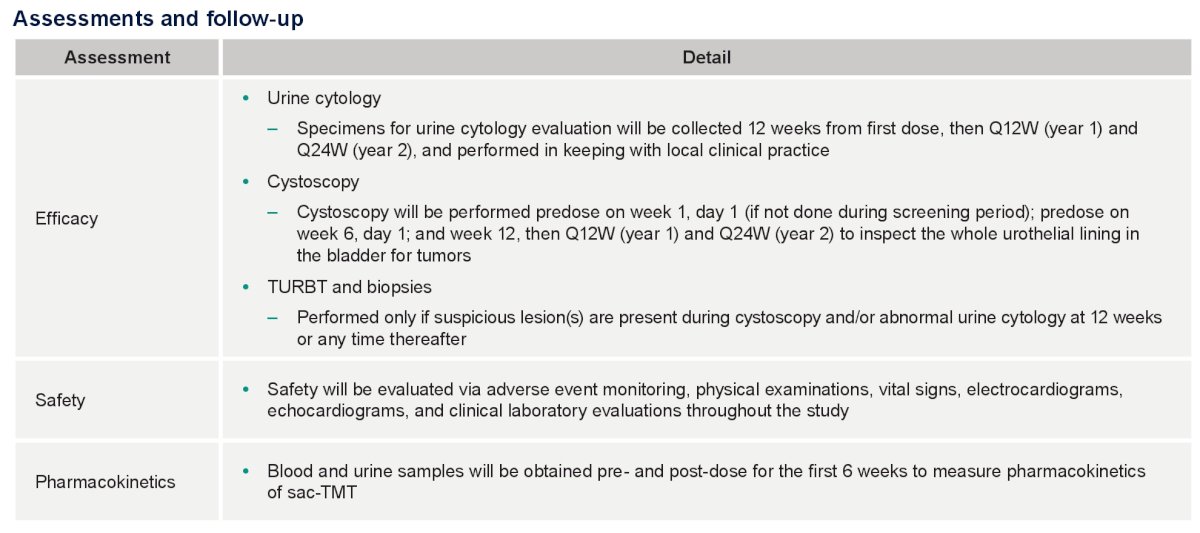
The assessments and follow-up are summarized below:
The statistical analytic plan is as follows:
TroFuse-027 will be conducted across Canada, France, Netherlands, Spain, United Kingdom, and the United States and is currently recruiting participants. Future studies (phase 2) will be initiated upon completion of dose escalation and based on the totality of data.
Presented by: Joshua Meeks, MD, PhD, Associate Professor of Urology, Department of Urology, Northwestern University Feinberg School of Medicine, Chicago, IL
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:- Powles T, Csőszi T, Özgüroğlu M, et al. Clinical efficacy and safety of enfortumab vedotin in patients with previously treated locally advanced or metastatic urothelial carcinoma: a multicentre, open-label, single-arm, phase 2 study. Ann Oncol. 2022;33(3):244-258.
- Chevli KK, Narla S, Gelfand J, et al. Outcomes of patients with bladder cancer undergoing radical cystectomy: analysis of a large community-based population. Urology. 2020;96(1):61-69.
- Grabe-Heyne K, Seitz AK, Rink M, et al. Immune checkpoint inhibitors in advanced urothelial carcinoma: biomarkers, clinical activity, and perspectives. Front Oncol. 2023;13:1170124.
- Shvartsur A, Bonavida B. The role of nuclear factor-kappa B in tumor progression and the therapeutic potential of its inhibitors. Genes Cancer. 2015;6(3-4):84-105.
- Choi W, Ochoa A, McConkey DJ, et al. Genetic alterations in the molecular subtypes of bladder cancer: illustration in the Cancer Genome Atlas dataset. Eur Urol. 2022;81(2):138-142.
- Loriot Y, Tagawa ST, Galsky MD, et al. Phase 3 study of sacituzumab govitecan versus chemotherapy in patients with previously treated locally advanced or metastatic urothelial carcinoma. Ann Oncol. 2024;35(3):392-401.
- Ye D, Petrylak DP, Rosenberg JE, et al. A phase 3 trial of enfortumab vedotin plus pembrolizumab versus chemotherapy in previously untreated locally advanced or metastatic urothelial carcinoma (EV-302). J Clin Oncol. 2025;43(suppl 5):Abstract 796.
- Grivas P, Sternberg CN, Powles T, et al. Updated analysis from the phase 3 study of avelumab first-line maintenance therapy in patients with advanced urothelial carcinoma (JAVELIN Bladder 100). J Clin Oncol. 2024;42(12):1415-1425.
- McGregor BA, Zhang T, Xu H, et al. A phase II trial of combination checkpoint blockade in metastatic urothelial carcinoma: clinical activity and molecular correlates. Ann Oncol. 2024;35(1):91-99.
- Yin Y, Zhang L, Li J, et al. Spatially resolved single-cell analysis reveals immune microenvironment remodeling after immune checkpoint blockade in bladder cancer. Nat Med. 2025 Apr 11. doi:10.1038/541591-025-03630-W.