(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a kidney and bladder cancers poster session. Dr. Jens Bedke presented the patient-reported outcomes (PROs) from CREST, a phase II trial of sasinlimab in combination with bacillus Calmette-Guérin (BCG) in BCG-naive, high-risk, non–muscle-invasive bladder cancer (NMIBC).
Standard of care for high-risk NMIBC includes TURBT followed by BCG induction + maintenance therapy.1,2 Approximately 40% of patients experience disease recurrence or progression at 24 months, with unfavorable prognoses.3 There is a high unmet need for enhanced treatment options that provide durable disease control by delaying disease recurrence and progression while maintaining quality of life.
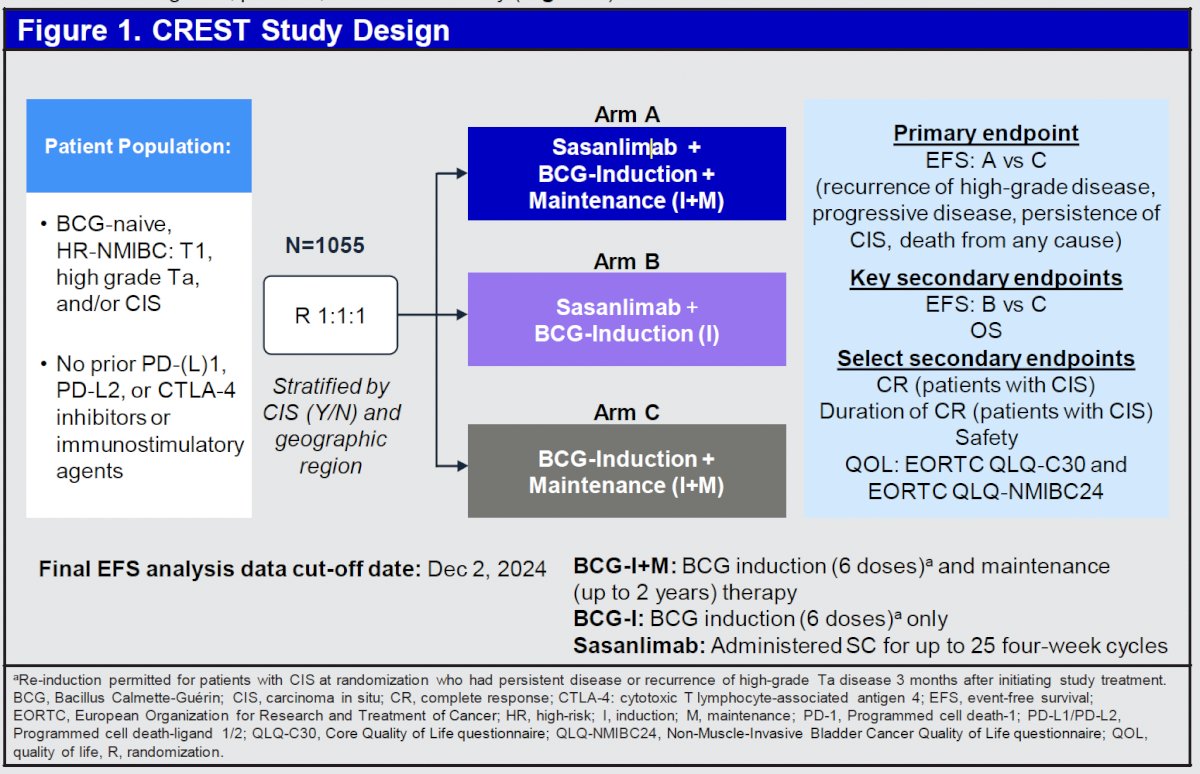
In the phase III CREST trial, sasanlimab in combination with BCG induction + maintenance (Arm A) demonstrated a statistically significant improvement in event-free survival (EFS), compared with the standard of care of BCG induction + maintenance (Arm C) in patients with high-risk NMIBC. No difference in EFS was observed between sasanlimab in combination with BCG induction (Arm B) and BCG induction + maintenance (Arm C).4
Oncology studies of patient preferences suggest that patients generally prefer the subcutaneous route of administration to other routes.5 In the CREST trial, subcutaneous sasanlimab (300 mg) was administered in a 2-mL prefilled syringe every 4 weeks, for up to 25 cycles. Herein, Dr. Bedke reported PROs for Arm A versus C of the CREST study to assess the impact of sasanlimab in combination with BCG induction + maintenance on quality of life in patients with high-risk NMIBC
The study design of the CREST trial is summarized below:
PROs were secondary endpoints and not included in the testing hierarchy. The EORTC QLQ-C30 and EORTC QLQ-NMIBC24 questionnaires were conducted at baseline, throughout treatment at select scheduled visits, and during the safety follow-up periods.

Completion rates were calculated as the number of patients who completed all questions divided by the number of patients who were expected to complete the questionnaire at each respective visit. Plots of mean change from baseline over time for the EORTC QLQ-C30 Global Health Status and NMIBC24 urinary symptoms scores are descriptive. Longitudinal mixed effect-model analyses were used to assess change from baseline in the EORTC QLQ-C30 and NMIBC24 items.
Model predictors were the corresponding baseline PRO score, treatment, time (continuous variable), and treatment-by-time interaction; intercept and time were considered as random effects particular to each participant. A ≥10-point within-group change from baseline has been validated as clinically meaningful for EORTC QLQ-C30.6 A between-group estimated mean difference in within-group change of 5 to 10 points is typically considered clinically meaningful. Data are presented for Arm A and Arm C.
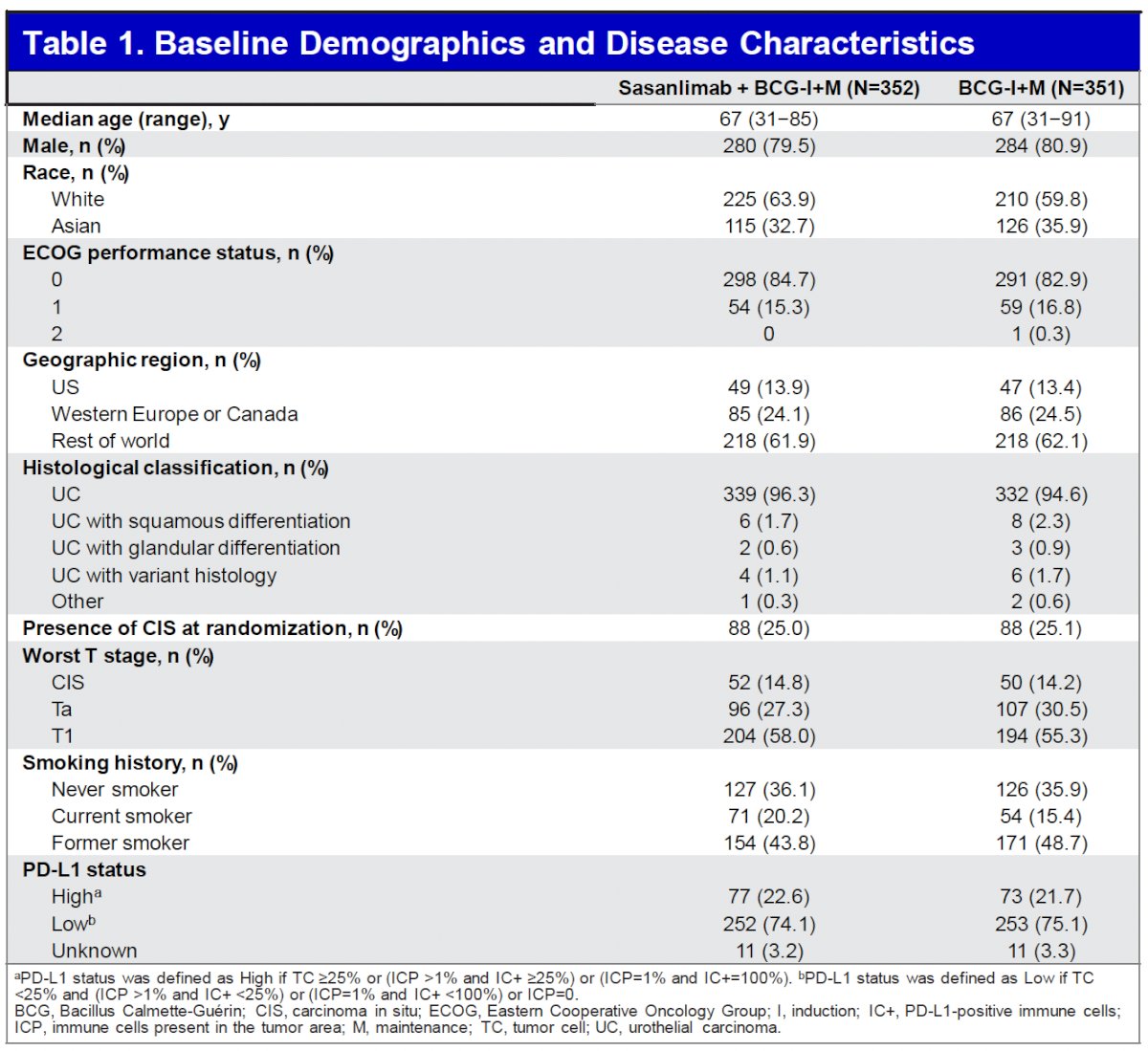
Baseline demographics and disease characteristics were generally balanced between arms. The study population for Arms A and C was predominantly male (80%) and had an ECOG performance status of 0 (84%). Pure urothelial carcinoma was reported in 95.4% of patients, 56.6% had T1 tumor as the highest grade, and 25% had CIS with or without papillary tumors.
The completion rates were >84% for all visits through the end-of-treatment visit (Cycle 25).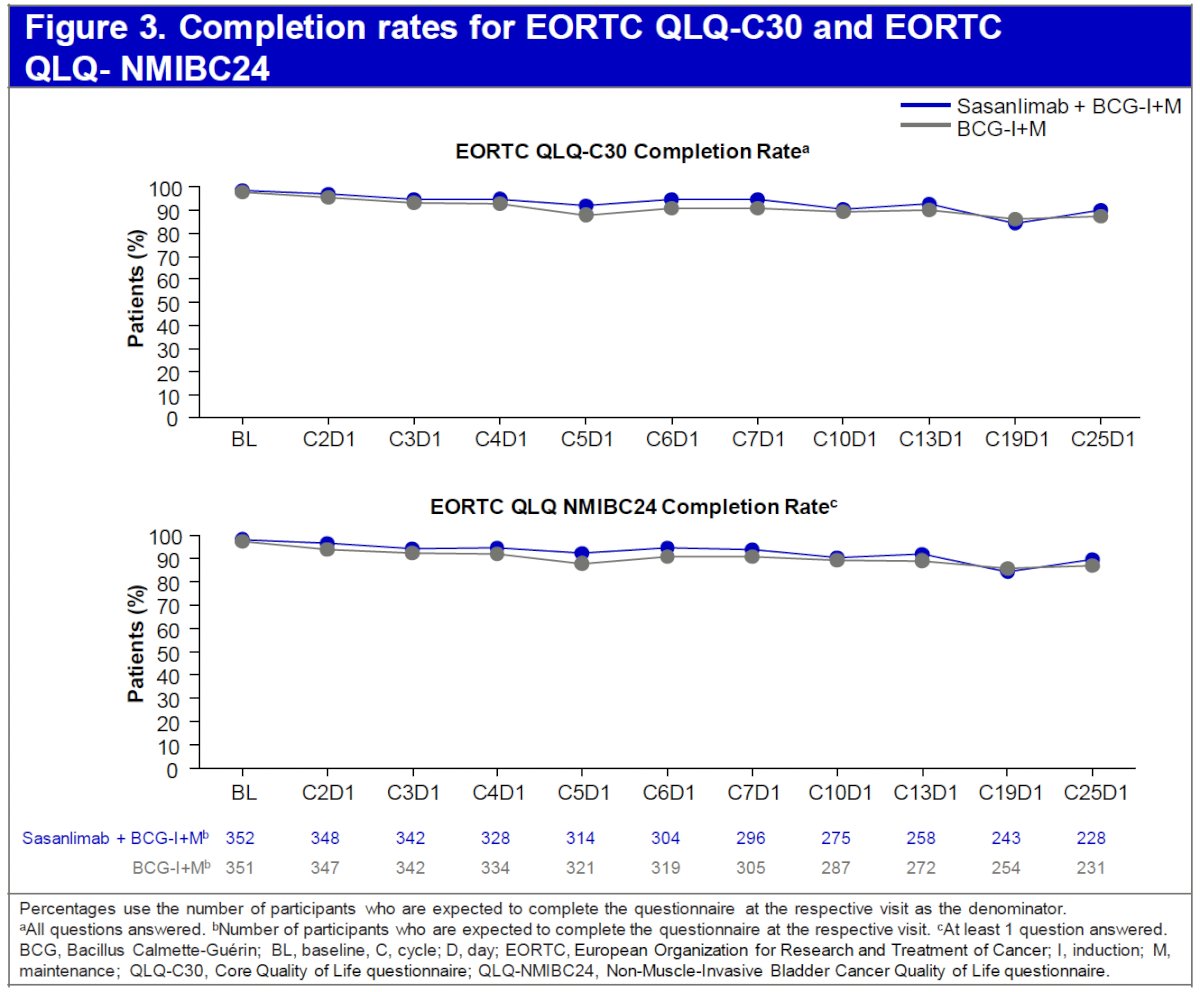
For EORTC QLQ-C30, the baseline Global Health Status scores were numerically similar between arms. A descriptive summary of mean change from baseline over time for the EORTC QLQ-C30 by visit for each treatment arm is shown for Global Health Status in the figure below.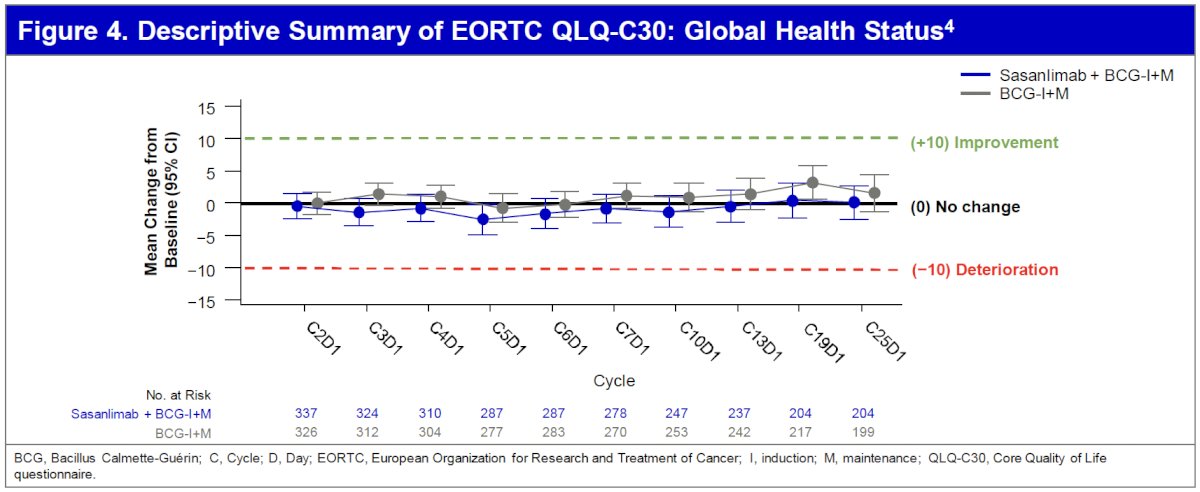
Longitudinal changes for the functioning scales had similar findings to the Global Health Status.
In the mixed model analysis, no functioning scale or symptom met the definition of a clinically meaningful change from baseline of ≥10 points for either treatment arm for within-arm comparisons. No differences met the 5 to 10-point threshold of a clinically meaningful difference between treatment arms.
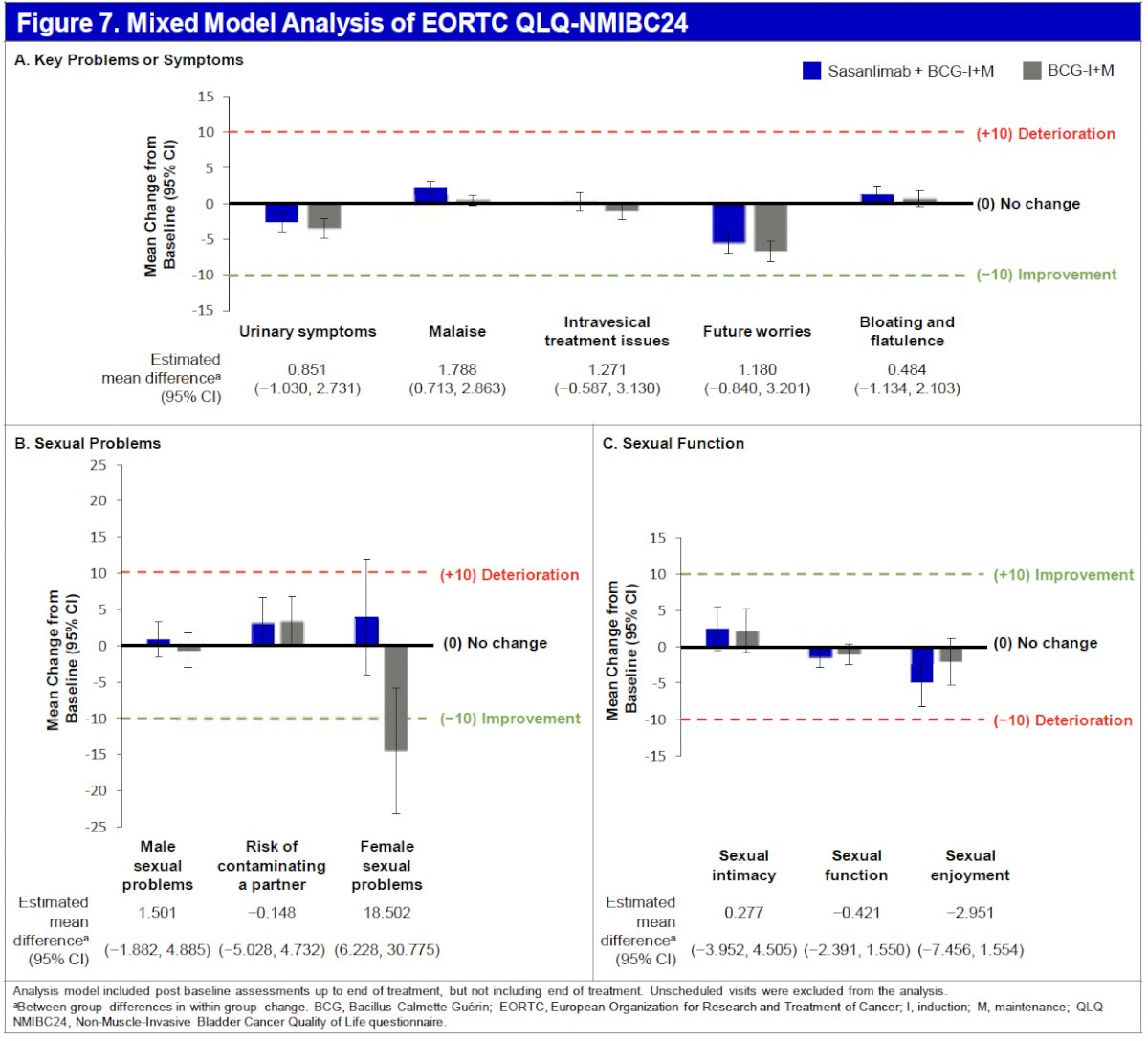
A descriptive summary of mean change from baseline over time for the EORTC QLQ-NMIBC24 urinary symptoms by visit for each treatment arm is shown below.
In the mixed model analysis for estimated mean differences between groups, no symptom met the threshold for a clinically meaningful difference between treatment arms, and no symptom met the definition of a clinically meaningful change from baseline in either treatment arm, except female sexual problems, which was assessed in a small subset of patients (Arm A, n=5; Arm C, n=4).
Dr. Bedke concluded as follows:
- In both the sasanlimab + BCG induction + maintenance (Arm A) and BCG induction + maintenance (Arm C) arms, PROs across functioning domains and key symptoms measured by the EORTC QLQ-C30 and NMIBC24 questionnaires had no clinically meaningful change from baseline, based on a 10-point threshold
- Between-group differences in within-group change did not meet the threshold of a 5- to 10-point difference to be clinically meaningful
- These PROs can help inform the benefit-risk assessment of sasanlimab in combination with BCG induction + maintenance
- The enhanced efficacy outcomes reported in the primary analysis and these results support that subcutaneous sasanlimab in combination with BCG induction + maintenance has the potential to redefine the treatment paradigm and clinical decision-making for patients with high-risk NMIBC without additional impacts on patient quality of life.
Presented by: Jens Bedke, MD, Department of Urology and Eva Mayr-Stihl Cancer Center, Klinikum Stuttgart, Stuttgart, Germany
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:- Holzbeierlein JM, Wright JL, Thrasher JB, et al. Contemporary management of BCG-unresponsive non–muscle-invasive bladder cancer. J Urol. 2024;211:533–8.
- Gontero P, Sylvester RJ, Rodríguez Otero J, et al. Systematic review and individual patient data meta-analysis of variant histology non–muscle-invasive bladder cancer. Eur Urol. 2024;86:531–49.
- Kamat AM, Li R, O’Donnell MA, et al. Predicting response to intravesical bacillus Calmette-Guérin in high-risk non–muscle-invasive bladder cancer: development and validation of a nomogram from an international cohort. J Clin Oncol. 2016;34(16):1935–44.
- Shore ND, Powles T, Bedke J, et al. Sasanlimab in combination with Bacillus Calmette-Guérin improves event-free survival versus Bacillus Calmette-Guérin as standard of care in high-risk non–muscle-invasive bladder cancer: Phase 3 CREST study results. J Urol. 2025;213(5S):e1001.
- Aguiar-Ibáñez R, Fotheringham I, Mittal L, et al. Differences between intravenous and subcutaneous modes of administration in oncology from the patient, healthcare provider, and healthcare system perspectives: a systematic review. Adv Ther. 2024;41(12):4396–4417.
- Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139–144.