(UroToday.com) The 2025 ASCO annual meeting featured a urothelial carcinoma oral abstract session and a discussant presentation by Dr. Jacqueline Brown discussing three abstracts, including “Nivolumab + ipilimumab versus gemcitabine + carboplatin chemotherapy for previously untreated unresectable or metastatic urothelial carcinoma: Final results for cisplatin-ineligible patients from the CheckMate 901 trial” by Dr. Michiel van der Heijden, “Avelumab + sacituzumab govitecan versus avelumab monotherapy as first-line maintenance treatment in patients with advanced urothelial carcinoma: Interim analysis from the JAVELIN Bladder Medley phase 2 trial” by Dr. Jeannie Hoffman-Censits, and “Exploratory analysis of responders from the phase 3 EV-302 trial of enfortumab vedotin + pembrolizumab versus chemotherapy in previously untreated locally advanced or metastatic urothelial carcinoma” by Dr. Shilpa Gupta.
Dr. Brown started her presented by highlighting the last quarter century of first line therapy for metastatic urothelial carcinoma:

To put these treatment advances and the data presented today into context, Dr. Brown notes that she has a patient who has metastatic urothelial carcinoma with retroperitoneal lymphadenopathy who is worried about his prognosis and anxious to start treatment. In this context, the first trial she discussed was the JAVELIN Medley trial, an interim analysis of avelumab + sacituzumab govitecan versus avelumab as first line maintenance therapy:

We know from the phase 2 TROPHY-U-01 trial that sacituzumab govitecan is an active drug, with an objective response rate of 27%,1 in addition to a response rate of 23% in the phase 3 TROPiCS-04 trial,2 which both compare similarly to the objective response rate of 24.3% reported in JAVELIN Medley:

Sacituzumab govitecan also requires careful handling given the adverse events reported in JAVELIN Medley and previously in TROPiCS-04, where 4% of treatment adverse events led to death. Of note, primary G-CSF use was not mandated (21% received) in TROPiCS-04. As such, Dr. Brown cautions that sacituzumab govitecan may not be the right drug for maintenance therapy. So, where does sacituzumab govitecan go from here?
- Patients with bladder cancer require special consideration of their comorbidities
- Is the cost of sacituzumab govitecan over single agent chemotherapy justified based on a better objective response rate alone?
- Is 3rd line the best setting to test promising drugs in metastatic urothelial carcinoma?
- G-CSF prophylaxis and dose reduction will be needed in future trials
- Trop-2 is highly expressed in variant histologies
- Sacituzumab govitecan is now being tested in the non-metastatic setting
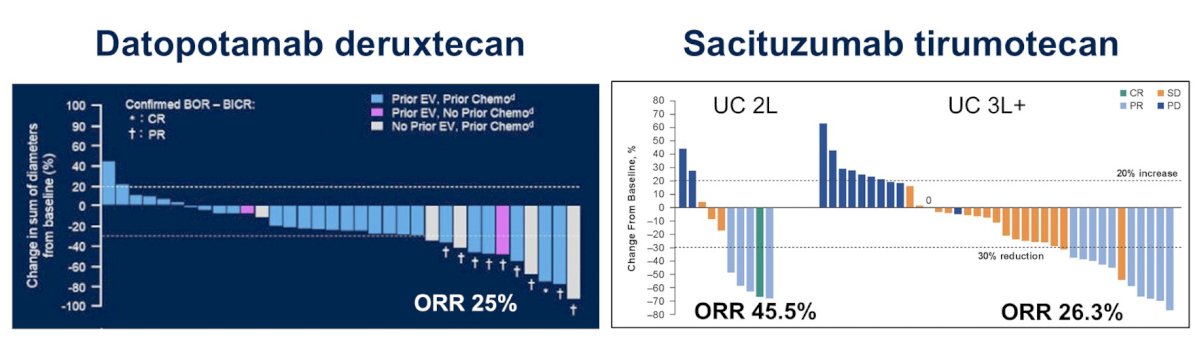
Dr. Brown highlighted that other Trop-2 targets have also been recently evaluated, including datopotamab deruxtecan (objective response rate 25%) and sacituzumab tirumotecan (objective response rate of 45.5% in second line; 26.3% in 3+ line):
Ultimately, the disease landscape is changing, and we have entered the wild west of post-enfortumab vedotin sequencing, with the likely following landscape:

Moreover, the investigation of sacituzumab govitecan + immunotherapy continues as a first line triple therapy. The phase 1 DAD trial assessed enfortumab vedotin + sacituzumab govitecan in the post immunotherapy and platinum setting, noting an objective response rate of 70% (n = 23).3 Currently, the phase 3 DAD-IO trial is recruiting, assessing enfortumab vedotin + pembrolizumab + sacituzumab govitecan in the first line setting.
Dr. Brown then discussed the CheckMate 901 trial assessing nivolumab + ipilimumab versus gemcitabine + carboplatin in first line metastatic urothelial carcinoma. As noted by Dr. van der Heijden, both co-primary endpoints for this study were negative:
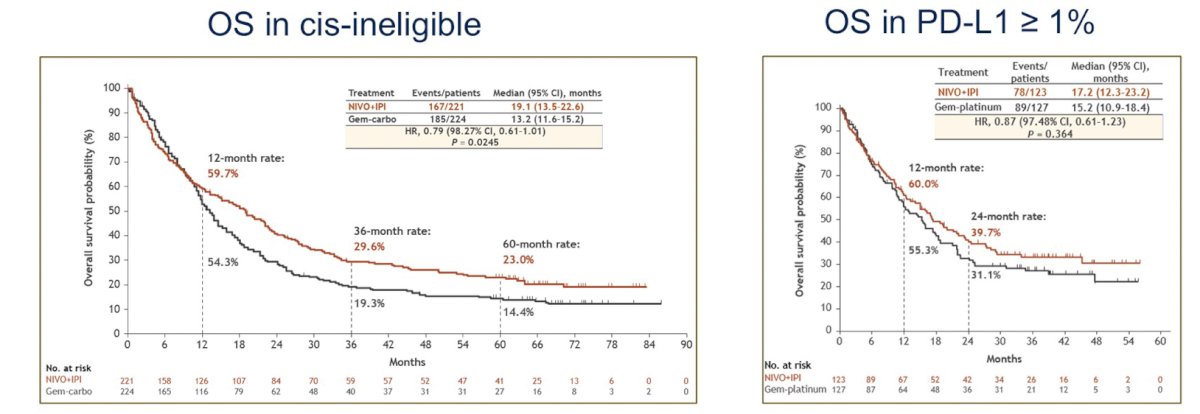
Dr. Brown notes that biomarkers are needed to select for exceptional responders. Looking closer at the overall survival Kaplan Meier curves, the curves are similar in year 1, have later separation, and if we consider a 5 year landmark overall survival assessment, the tail of the curve for these patients receiving immunotherapy is life changing:

As such, is there an intensified immunotherapy + antibody drug conjugate triplet in the first for first line cisplatin ineligible metastatic urothelial carcinoma? Previously reported at ESMO 2024, nivolumab + ipilimumab + sacituzumab govitecan demonstrated an overall response rate of 88.2%, a median progression free survival of 12.7 months, and median overall survival that was not reached, but the trial was terminated early after two deaths (8%) from immune mediate myocarditis. Dr. Brown notes that immunotherapy doublets have risks, as do triplets, thus, we should pursue these options cautiously.
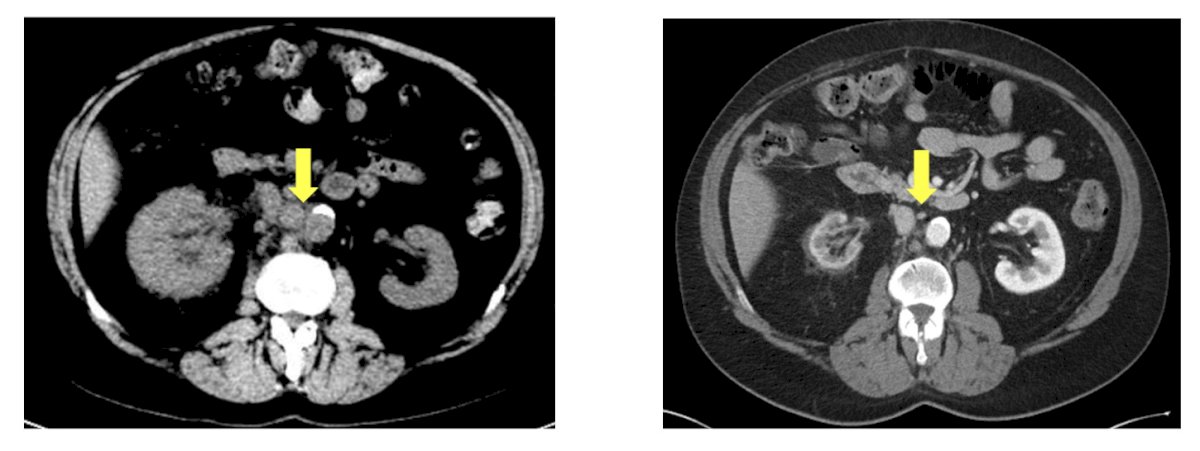
Can we apply these data from JAVELIN Medley and CheckMate 901 to the patient’s next week? No, but we can learn from them. Dr. Brown’s patient started on enfortumab vedotin + pembrolizumab, and after six months his scans showed a complete response:
But, how long will this last? How long does he continue when scans do not show active cancer? He has some numbness in his fingers that he says he can tolerate, and after all, his scans do not show cancer.
Dr. Brown then discussed the exploratory analysis of responders from EV-302, which she calls a victory lap for enfortumab vedotin + pembrolizumab, but she discussed it with special attention paid to the work we still have to do. Dr. Brown states that she can now tell her patient that 3 in 4 patients with scans like his maintain these scans 2 years later. He asks if he can be cured, and she tells him that it may be possible based on the duration of complete response in patients achieving an initial complete response is 74.3% at 2 years:

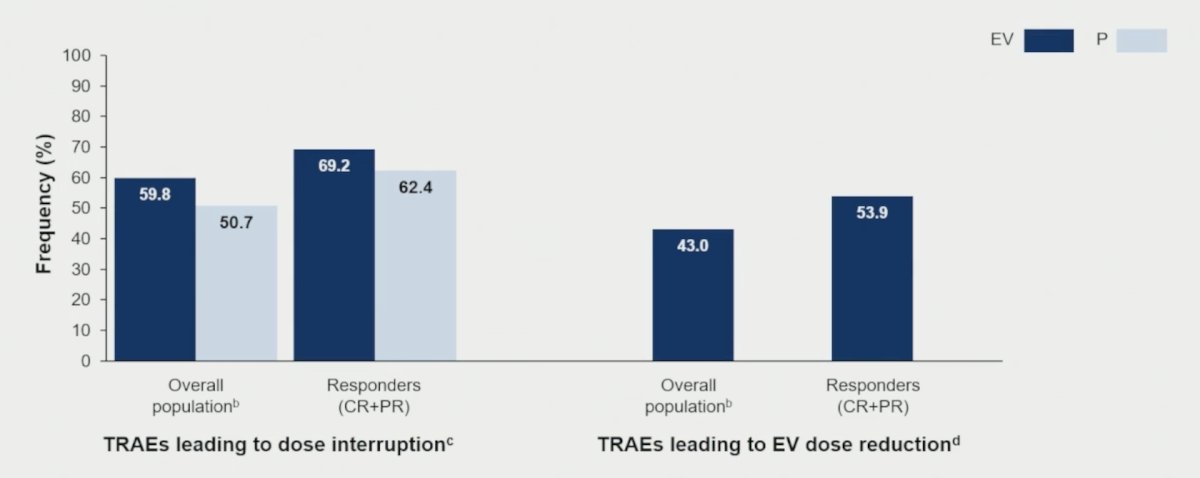
However, not surprisingly, responders received more treatment than the overall population in EV-302, with similar toxicities to the overall population, but we have to do better:

Grade 2 neuropathy impacts quality of life, specifically managing money, meal prep, driving, taking pills, and using a cell phone. The onset of grade 2 neuropathy from enfortumab vedotin + pembrolizumab typically is a median of 6 months after starting treatment, with improvement to grade 1+ toxicity taking a median 6.6 months after discontinuing therapy. But, at that point, do we restart enfortumab vedotin + pembrolizumab? Dr. Brown held her patient’s enfortumab vedotin + pembrolizumab for several cycles, and his next scans showed a continued complete response. But questions remain as to when to restart therapy and how we can avoid morbidity while not compromising his chance of cure?
Enfortumab vedotin + pembrolizumab is the right treatment, but it’s time to learn how to really use it:
- Enfortumab vedotin + pembrolizumab is chemotherapy, but unbound by the 4-6 cycles that platinum was. How much is enough?
- In the current state, optimization is guided by toxicity, and we are being reactive not proactive
- Grade 2 neuropathy is intolerable, and enfortumab vedotin + pembrolizumab dose interruption/reduction should happen before this
- The future state should include personalization of treatment dose and duration, incorporating radiographic and molecular response (ctDNA)
Right-sizing treatment is happening now, based on Dr. Gupta’s EV-302 update:
Additionally, a pilot trial at Fox Chase Cancer Center is assessing de-escalating enfortumab vedotin + pembrolizumab in metastatic urothelial carcinoma. The pilot trial has enrolled 40 out of 61 patients as of May 2025, and phase 2 trial is planned for Fall 2025:

For other patients, there is still an unmet need. In EV-302, the duration of partial response in partial responders is only 23.4% at 24 months, and 2 of 3 patients do not receive second line treatment. Thus, we need to focus on:
- Triplet therapy in first line with enfortumab vedotin + pembrolizumab
- ctDNA guided strategies for escalation
- Novel combination therapies (antibody drug conjugates + immunotherapy paradigm)
Dr. Brown concluded her discussant by emphasizing that breaking the platinum ceiling is not enough:
- We now face the challenge of customizing the roofline with the information we have learned from these studies and our patients
- From CHECKMATE-901: perhaps not a chemotherapy-free approach is feasible, but biomarker selection to de-escalate to immunotherapy monotherapy
- From JAVELIN Medley: the concept here is treatment intensification, and Trop-2 targeting agents may help us do that
- From EV-302: cure is possible, but side effects are likely
- We need to work together to make enfortumab vedotin + pembrolizumab the control arm of future trials
Presented by: Jacqueline T. Brown, MD, Emory University School of Medicine, Atlanta, GA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: Advances in Urothelial Cancer Treatment: Efficacy, Toxicity, and Unanswered Questions - Jacqueline Brown
References:
- Tagawa ST, Balar AV, Petrylak DP, et al. Metastatic urothelial carcinoma progressing after platinum-based chemotherapy and checkpoint inhibitors. J Clin Oncol. 2021 Aug 1;39(22):2474-2485.
- Powles T, Tagawa S, Vulsteke C, et al. Sacituzumab govitecan in advanced urothelial carcinoma: TROPiCS-04, a phase III randomized trial. Ann Oncol. 2025 May;36(5):561-571.
- McGregor BA, Sonpavde GP, Kwak L, et al. The Double Antibody Drug Conjugate (DAD) phase I trial: Sacituzumab govitecan plus enfortumab vedotin for metastatic urothelial carcinoma. Ann Oncol. 2024 Jan;35(1):91-97.