(UroToday.com) The 2025 ASCO annual meeting featured a urothelial carcinoma oral abstract session and a discussant presentation by Dr. John Sfakianos discussing two abstracts, including “Circulating tumor DNA in patients with muscle invasive bladder cancer who received perioperative durvalumab in NIAGARA” by Dr. Thomas Powles, and “Mitomycin + BCG as adjuvant intravesical therapy for high-risk, non muscle invasive bladder cancer: A randomized phase 3 trial (ANZUP 1301)” by Dr. Dickon Hayne.
Dr. Sfakianos started his presentation by discussing the NIAGARA trial and emphasizing his three takeaway points related to ctDNA:
- ctDNA is a novel biomarker with a strong clinical performance
- ctDNA clearance is a good prognostic indicator
- Attention is required for the ctDNA+ patients, which is approximately half of patients at presentation
ctDNA has good clinical performance and we have seen a robust contribution to the literature over the last several years. It is already established in guiding adjuvant therapy in stage II colon cancer, and a 2024 meta-analysis suggests it is a predictive and prognostic biomarker in the perioperative treatment of muscle invasive bladder cancer.1 Specifically, Dr. Sfakianos emphasized the conclusion of this meta-analysis stating “using ctDNA in clinical practice is a reality, with cumulative evidence of the prognostic and predictive impact on different tumor types.”
Nearly a quarter century ago, the old knowledge gap for muscle invasive bladder cancer was whether chemotherapy was important for patients undergoing radical cystectomy. Based on the Grossman et al.2 landmark neoadjuvant chemotherapy trial, the median survival among patients assigned to surgery alone was 46 months versus 77 months among patients assigned to neoadjuvant chemotherapy + radical cystectomy (p = 0.06). However, Dr. Sfakianos notes that there are patients who do not need neoadjuvant treatment (over-treated), those where ctDNA can assist in increasing the marginal benefit, and those that recur regardless of neoadjuvant treatment and who need earlier treatment intensification: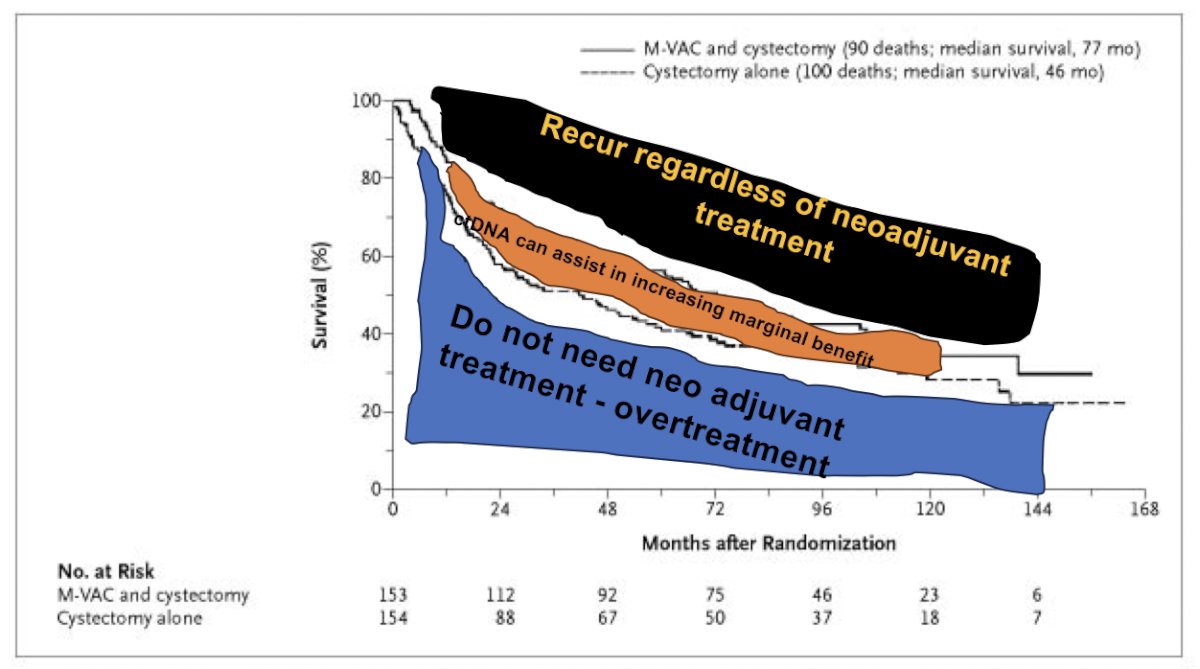
Christensen et al.3 were the first group to assess ctDNA in 2019 in the neoadjuvant setting, evaluating 68 patients with locally advanced muscle invasive bladder cancer. There were 658 plasma samples longitudinally collected before, during, and after therapy and analyzed using the Signatera assay:
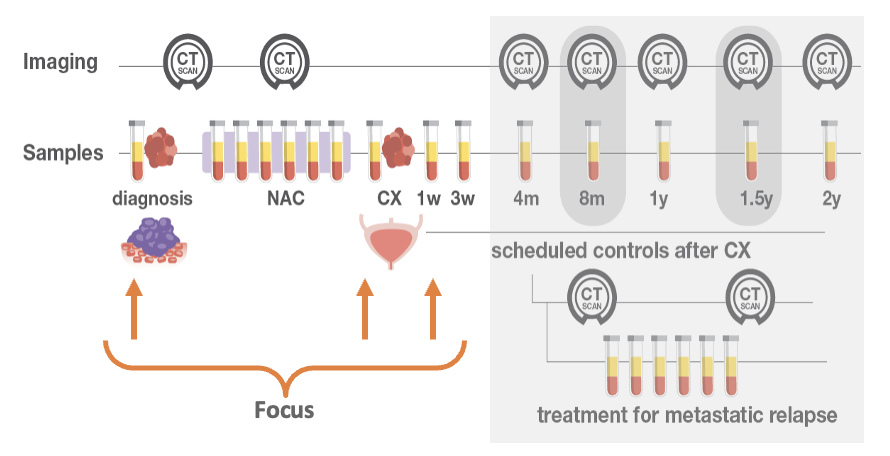
The key findings were that ctDNA is a prognostic marker after TURBT and before neoadjuvant chemotherapy, a lack of ctDNA clearance during neoadjuvant treatment is a better predictor of recurrence than pathologic response, lead time to clinical recurrence was a median of 96 days, and patients with serial negative ctDNA after radical cystectomy had an overall survival rate of 100%.
Recent work from Dr. Sfakianos’ group assessed whether ctDNA status before radical cystectomy is predictive of pathological and oncological outcomes, in addition to evaluating the dynamic changes in ctDNA status after radical cystectomy in relation to recurrence-free survival. Among 112 patients undergoing radical cystectomy from 2021-2023, ctDNA was detected before radical cystectomy in 53% of patients and was associated with poor recurrence free survival (log-rank p < 0.0001):

Additionally, multivariable analyses demonstrated that detectable ctDNA before radical cystectomy was associated with a higher risk of nodal disease (OR 5.4, 95% CI 1.9-18.2; p = 0.003) and locally advanced disease (OR 3.6, 95% CI 1.5-9; p = 0.005).
In NIAGARA, the event-free survival benefit in the durvalumab arm versus the comparator arm was observed in both the baseline ctDNA+ and ctDNA− groups:
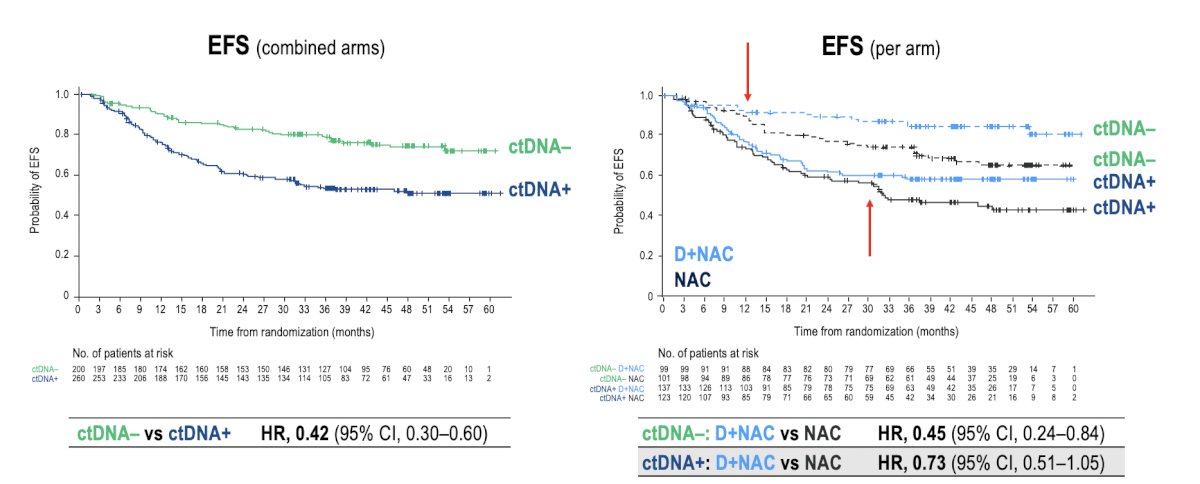
However, Dr. Sfakianos notes that this is not really a neoadjuvant therapy assessment, but rather a perioperative assessment and we do not really know whether the neoadjuvant and/or adjuvant treatment is contributing substantially to these results. Thus, the new knowledge gaps in the perioperative setting of muscle invasive bladder cancer are:
- Is ctDNA predictive?
- We will need novel clinical trial designs to better assess
- Can we de-escalate care for patients with negative ctDNA at presentation?
- Cystectomy alone?
- Cystectomy + adjuvant therapy?
- Bladder sparing?
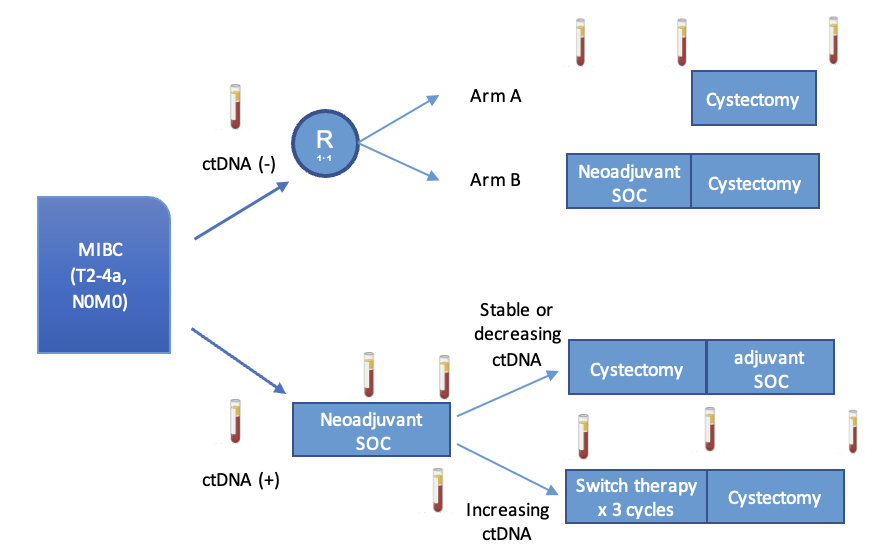
- How do we improve outcomes for ctDNA+ patients? Perhaps with the following trial design:
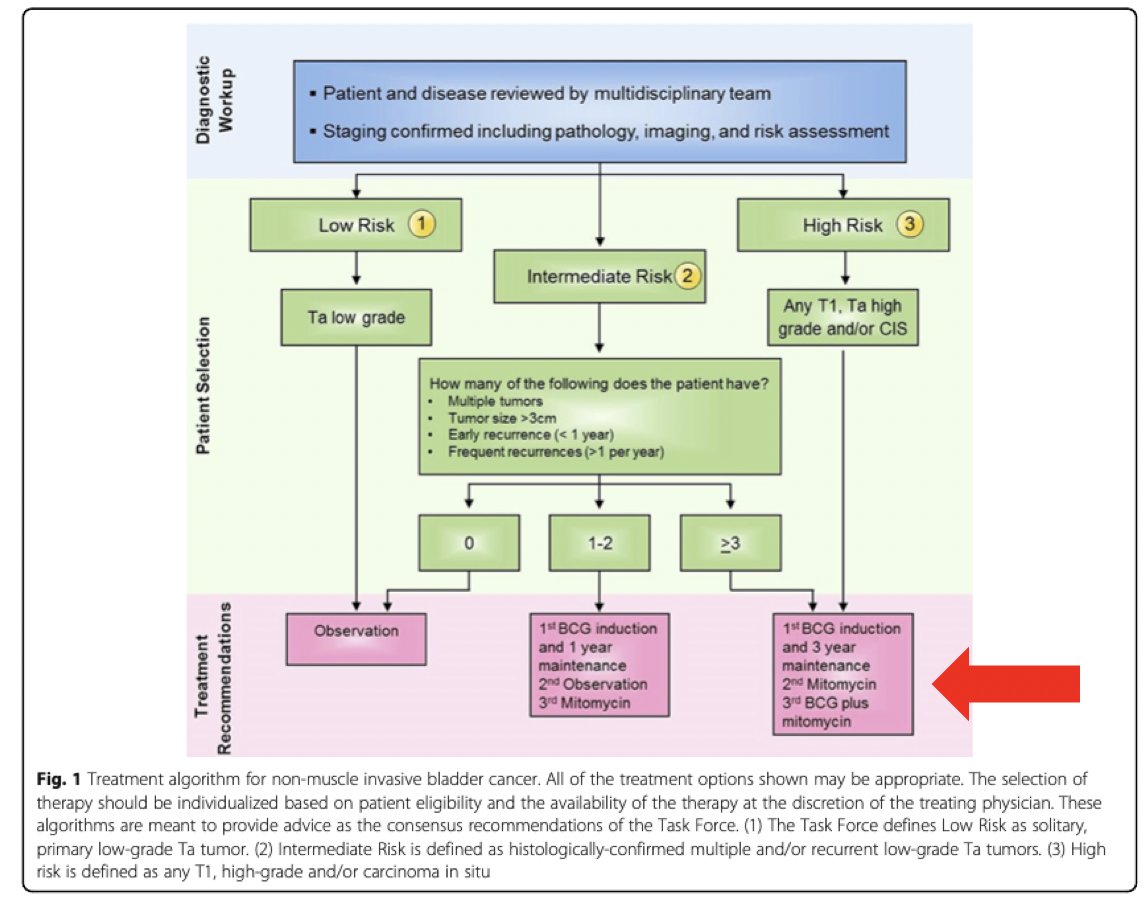
Dr. Sfakianos then discussed the ANZUP 1301 mitomycin + BCG phase 3 randomized trial. He notes that for high risk patients, mitomycin + BCG is already listed as a third option for treatment:
His key takeaways from this phase 3 trial are as follows:
- The BCG shortage is affecting patient care worldwide
- The BCG + mitomycin combination is well tolerated and has similar efficacy to BCG alone
- BCG-naïve non muscle invasive bladder cancer is the focus of many clinical trials
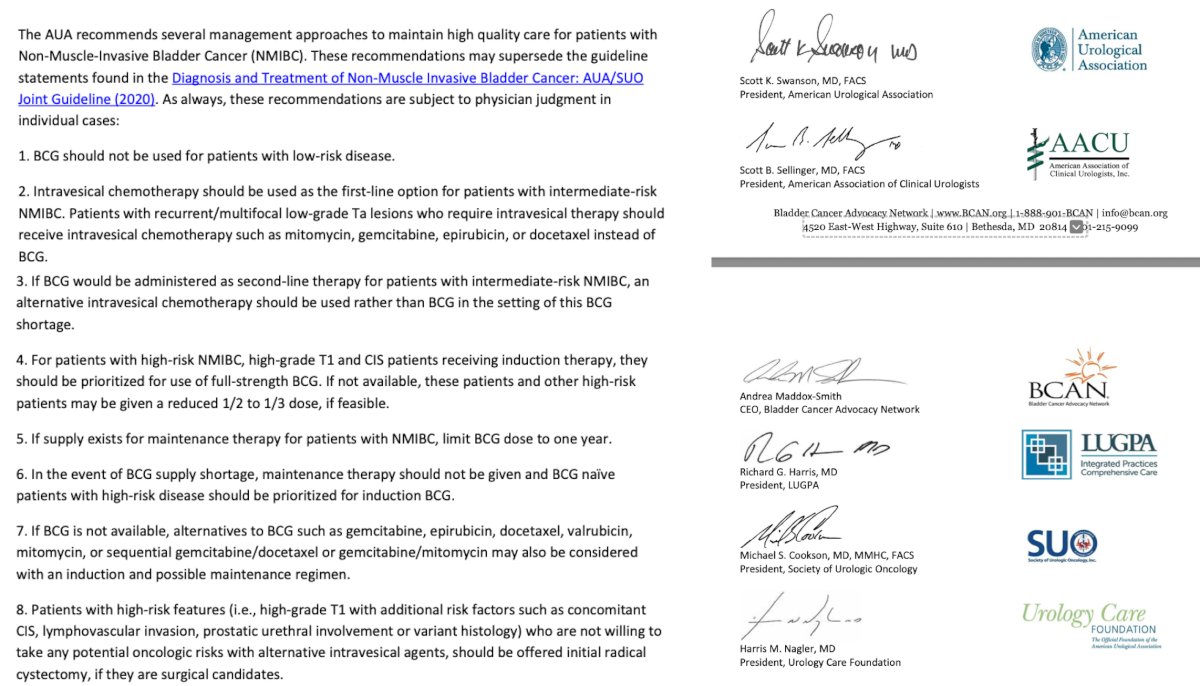
The BCG story as first line therapy in high risk non muscle invasive bladder cancer has been unchallenged since inception in 1976. However, the BCG shortage led key urologic organizations to quickly implement recommendations for alternative options for these patients:
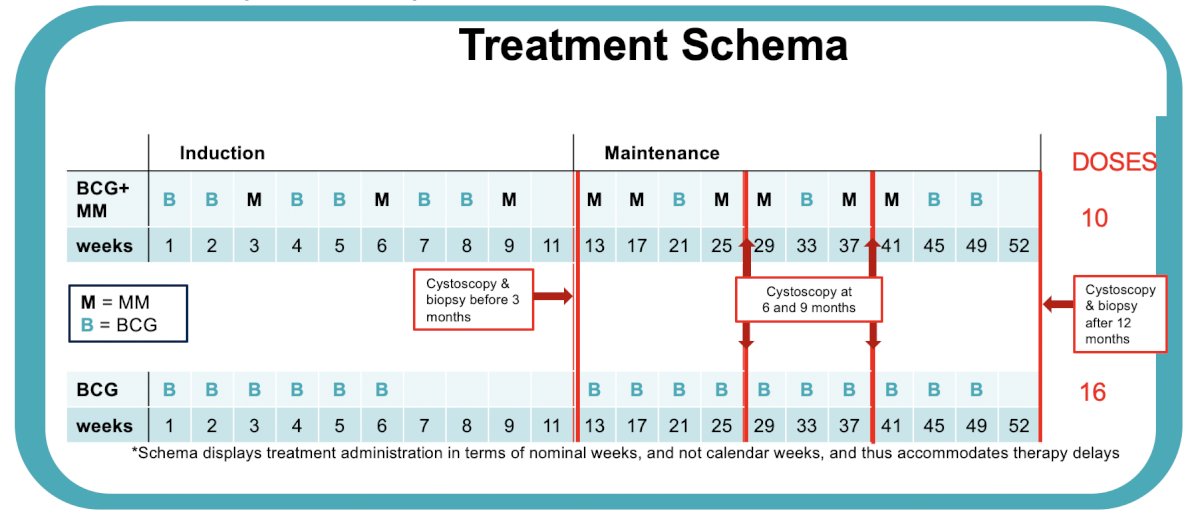
Unfortunately, the data to support these recommendation is generally retrospective, single center data, and expert opinion. As such, this has ignited a spark for more studies for BCG naïve non muscle invasive bladder cancer. This includes BCG unresponsive agents being moved to the front line (TAR-200, cretostimogene, chemotherapy options, novel agents, etc), as well as the EA8212 BRIDGE trial assessing BCG versus gemcitabine + docetaxel. In the ANZUP 1301 trial, Dr. Sfakianos notes that incorporating mitomycin + BCG would allow him to save 6 vials of BCG for every patient treated with this combination regimen:
Based on the efficacy endpoints of this trial, there were no statistically significant differences between the mitomycin + BCG versus BCG alone arms:

Dr. Sfakianos concluded his discussant presentation by emphasizing there is an exciting time to come in BCG naïve non muscle invasive bladder cancer:
- BCG naïve non muscle invasive bladder cancer is the new BCG unresponsive disease state
- There is a large phase III clinical trial
- Many new agents are competing against BCG
- Novel BCG and chemotherapy combinations are on the horizon
- We are learning about the biology and mechanisms of therapies
Presented by: John Sfakianos, MD, Icahn School of Medicine at Mount Sinai, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:
- Crupi E, de Padua TC, Marandino L, et al. Circulating tumor DNA as a Predictive and Prognostic Biomarker in the Perioperative Treatment of Muscle-invasive bladder cancer: A systematic review. Eur Urol Oncol. 2024 Feb;7(1):44-52.
- Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med 2003;349(9):859-866.
- Christensen E, Birkenkamp-Demtroder K, Sethi H, et al. Early detection of metastatic relapse and monitoring of therapeutic efficacy by ultra-deep sequencing of plasma cell-free DNA in patients with urothelial bladder carcinoma. J Clin Oncol. 2019 Jun 20;37(18):1547-1557.
- Ben-David R, Tillu N, Cumarasamy S, et al. Longitudinal tumor-informed circulating tumor DNA status predicts disease upstaging and poor prognosis for patients undergoing radical cystectomy. Eur Urol Oncol. 2024 Oct;7(5):1105-1112.