(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30 and June 3 was host to the session Advancing Perioperative Treatment Options for Localized Muscle-Invasive Bladder Cancer: A Step Forward. Dr. Anne Schuckman delivered a presentation titled: Navigating the Crossroads: Evolving Paradigms in Perioperative Management of Muscle-Invasive Bladder Cancer.
Dr. Schuckman opened her presentation by emphasizing the complexity of treatment decision-making in muscle-invasive bladder cancer (MIBC), particularly within the evolving landscape of perioperative management. Patients today stand at a therapeutic crossroads between three main options: trimodal therapy (TMT), radical cystectomy (RC) alone, and the more established approach of neoadjuvant chemotherapy followed by RC (RC + NACT).
Our roadmap requires a multifaceted evaluation that accounts for physician and patient-specific factors, potential physical and financial toxicities, and the specificity of treatment based on tumor biology. She also highlighted the growing importance of biomarkers to better guide therapy selection and the role of ongoing clinical trials in refining treatment strategies.
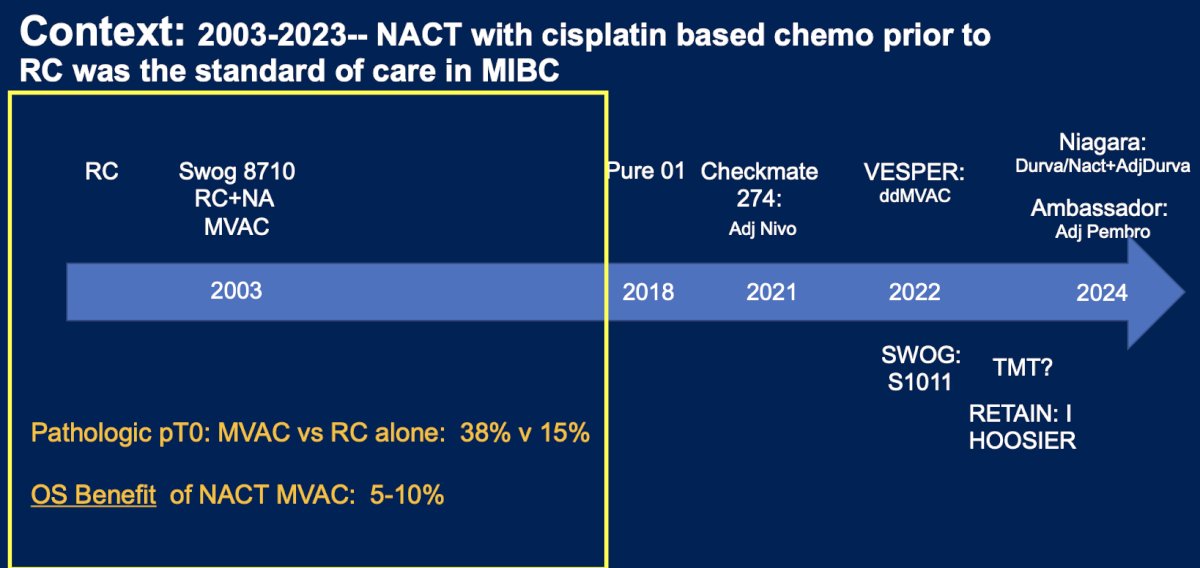
Historically, between 2003 and 2023, neoadjuvant cisplatin-based chemotherapy followed by RC was the standard of care for MIBC, supported by the SWOG 8710 trial. This study showed a significant improvement in pT0 rates with MVAC (38%) versus RC alone (15%), and a 5–10% overall survival benefit.1 However, the treatment landscape has evolved. Adjuvant immunotherapy is now a standard option for select patients, and perioperative combination strategies such as those evaluated in the NIAGARA trial using neoadjuvant chemotherapy plus durvalumab followed by adjuvant durvalumab are redefining the management of MIBC.2
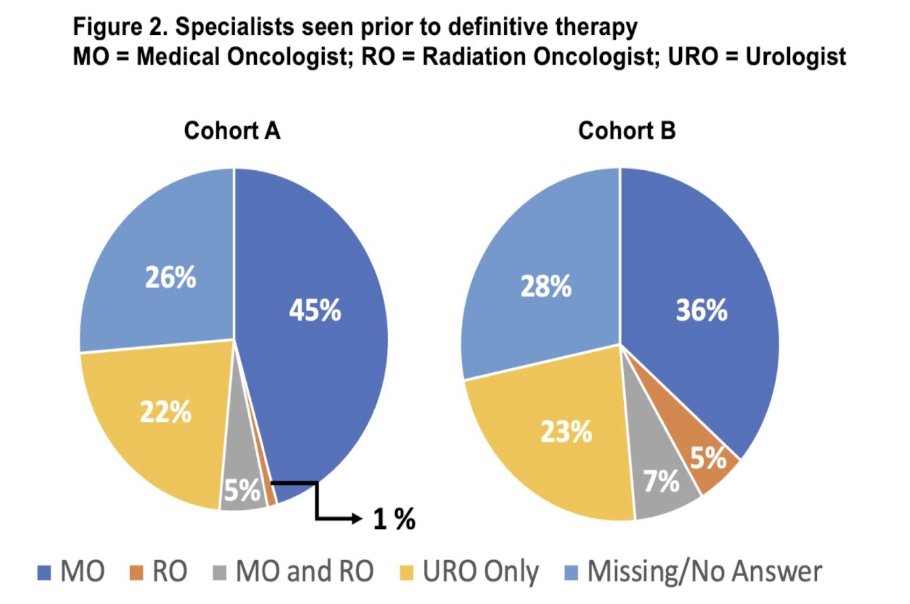
Notably, treatment usage trends from a Bladder Cancer Advocacy Network (BCAN) survey presented at GU ASCO 2025 revealed that only 1–5% of patients reported having seen a radiation oncologist and only half were referred to a medical oncologist to discussed neoadjuvant chemotherapy.
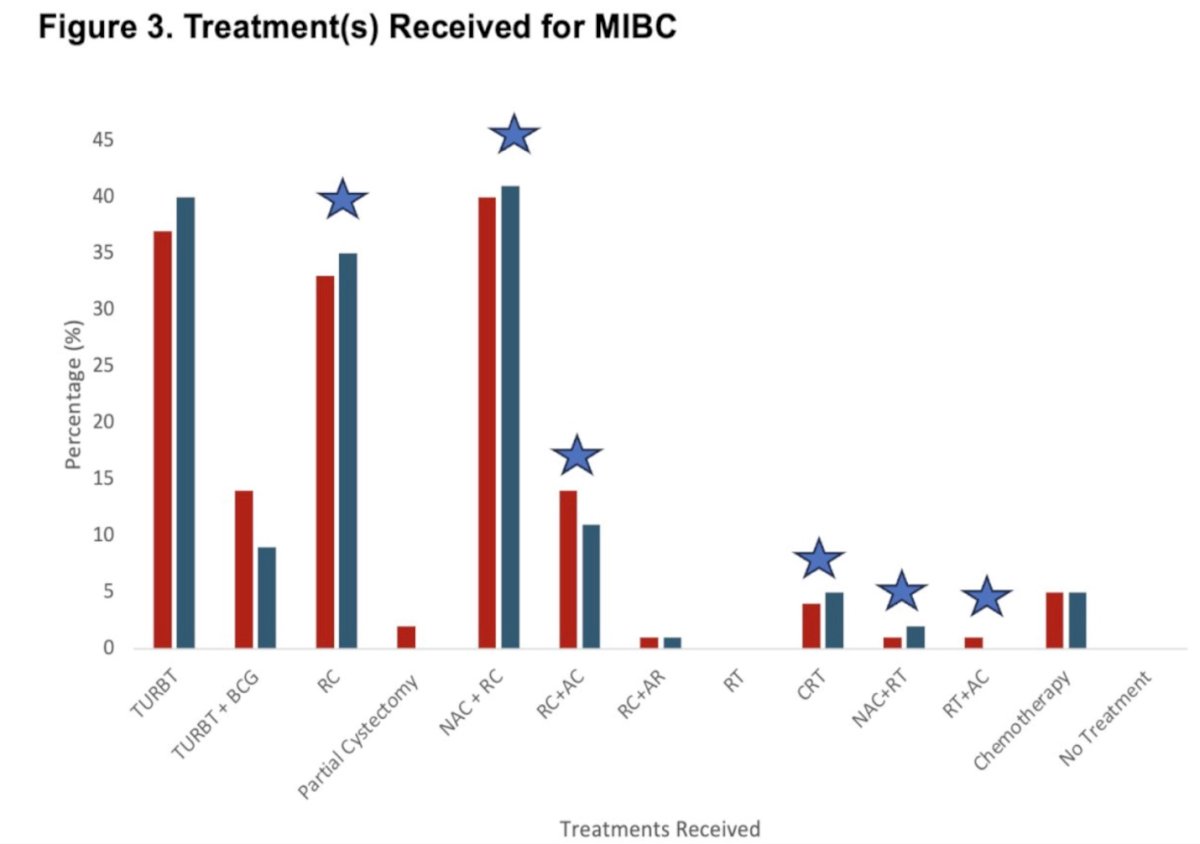
Moreover, when evaluating the treatments received by patients in this survey study, the majority underwent RC with or without NAC or AC. Only a small fraction received chemoradiotherapy (CRT), NAC followed by radiation therapy, or radiation therapy combined with AC, underscoring limited uptake of bladder-preserving strategies in real-world practice.3
The most common reasons for patients not receiving NAC before RC include perceived limited benefit of systemic therapy for individual patients, concerns about ineligibility or toxicity, patients declining systemic treatment, and the risk of overtreatment in many who may not ultimately require it.
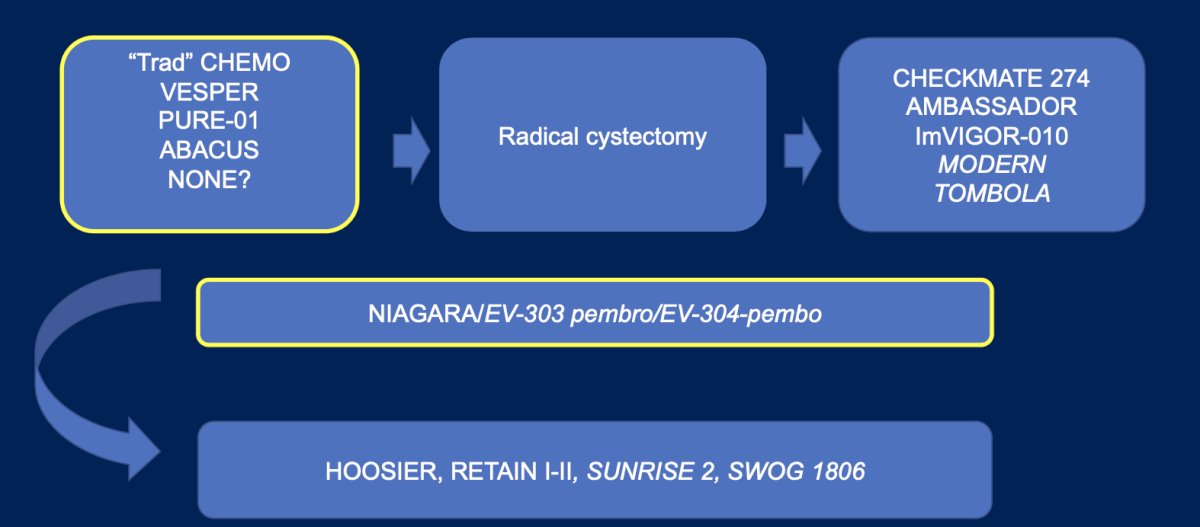
The current treatment landscape for MIBC includes several evolving strategies. Standard options involve NAC commonly with six cycles of dose-dense MVAC, followed by RC. For patients with high-risk features post-surgery, adjuvant immunotherapy with nivolumab or pembrolizumab is now incorporated into care. Additionally, the NIAGARA trial has introduced a perioperative approach combining cisplatin-based NAC with durvalumab, followed by adjuvant durvalumab. Bladder-sparing options like TMT remain relevant, alongside ongoing trials evaluating novel bladder-preserving strategies. These are the choices we are increasingly asked to make in clinic, as illustrated in the figure below.
The critical questions we must ask ourselves when managing patients with MIBC are: Should all patients receive the same amount and kind of therapy? and will they all derive the same benefit? The answer, increasingly, is no. To guide individualized treatment decisions, several tools and factors should be considered, including:
- Clinical stage and disease burden
- Performance status and frailty
- Renal and physiologic function, particularly cisplatin eligibility
- Presence of obstruction, pain, or other symptoms precluding chemotherapy
- Locally advanced disease or variant histology
Biomarkers
- PD-L1 status for potential immunotherapy benefit
- Circulating tumor DNA (ctDNA) for residual disease detection
- Genetic markers that may predict therapy response
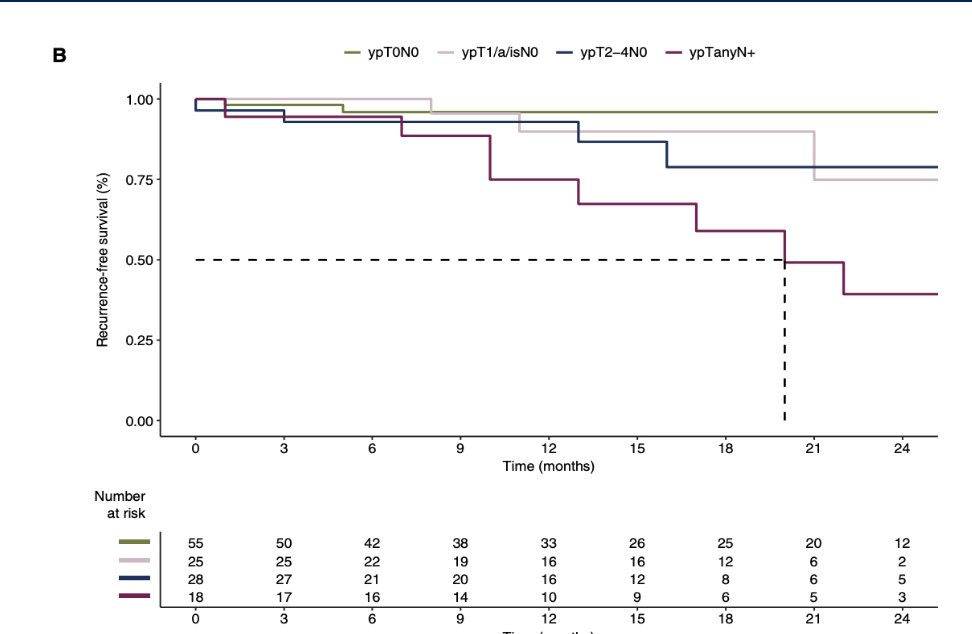
The PURE-01 trial demonstrated a complete pathological response ypT0 rate of 42% (95% CI, 28.2% to 56.8%). Notably, patients achieving ypT0N0 after cystectomy experienced the most favorable survival outcomes as illustrated below.4
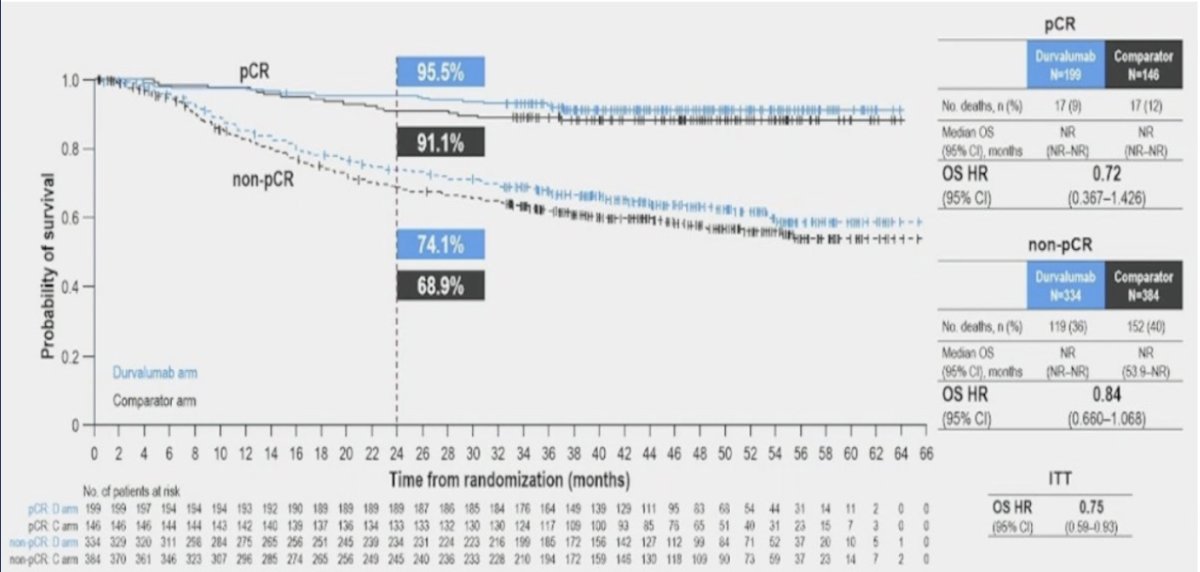
Similarly, pathological downstaging to ypT0 with NAC/ICI in the NIAGARA study was associated with significantly improved overall survival. Patients who achieved a pathological complete response (pCR) had better OS outcomes compared to those who did not, in both the treatment and comparator arms.3
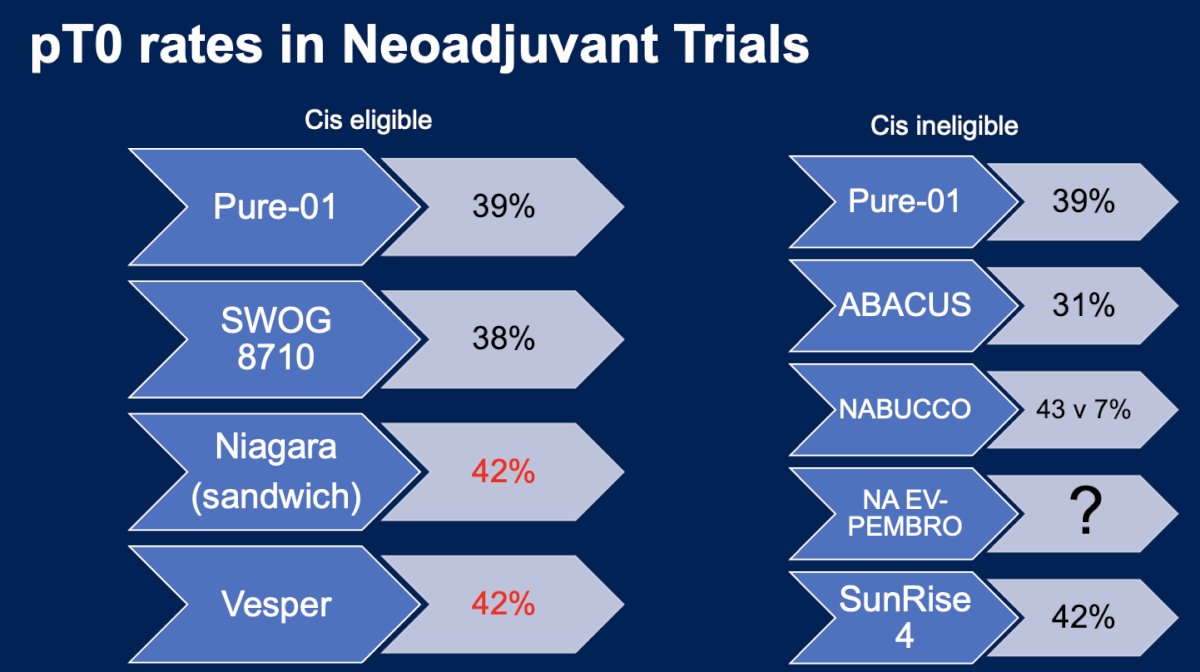
The ypT0 rates in neoadjuvant trials have steadily increased in both cisplatin-eligible and cisplatin-ineligible patients, with complete response rates reaching up to 42%.
However, this increase in pCR rates is associated with a notable toxicity burden. In the VESPER trial, 43% of patients receiving ddMVAC experienced grade ≥3 serious adverse events. Similarly, in the NIAGARA trial, immune-related grade ≥3 SAEs occurred in 3% of patients, with total immune toxicity reaching 21% in the durvalumab arm compared to 3% in the placebo group.3,5
Moreover, the surgical toxicity of neoadjuvant immunotherapy (IO) remains largely unknown. In the PURE-01 trial, high-grade complications occurred in 35% of patients, though there was no control arm for comparison. A separate analysis from Mount Sinai Hospital evaluated 136 patients who underwent neoadjuvant IO therapy and reported Clavien-Dindo grade ≥3 complications in 27% at 30 days and 16% at 90 days. Importantly, there was no observed difference in complication rates between IO alone and chemo-IO combinations. However, these complication rates appeared higher than historical benchmarks for robotic-assisted radical cystectomy (RARC).
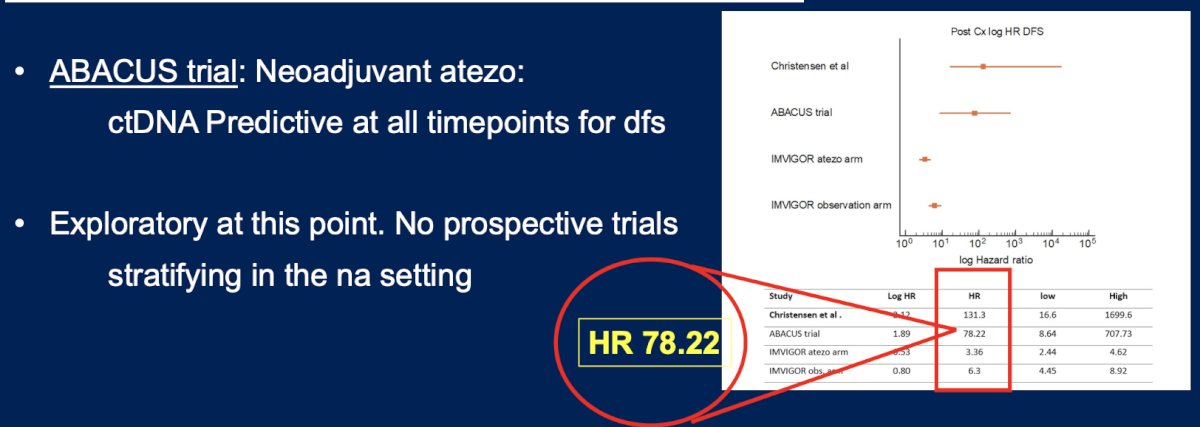
Dr. Schuckman moved on to discuss if biomarkers can predict pCR rates. In PURE-01, PD-L1 expression using CPS ≥10 was associated with higher rates of pT0, suggesting potential predictive value. In contrast, PD-L1 was not predictive in either the NIAGARA or ABACUS trials. Circulating tumor DNA (ctDNA) was not assessed in PURE-01 or NIAGARA, but in ABACUS, ctDNA positivity was predictive at all timepoints of disease-free survival (DFS).6 However, this analysis is only exploratory at this point and there are no prospective trials addressing this dilemma in the neoadjuvant setting.
Data from the University of Southern California (USC) evaluating management trends and outcomes in patients undergoing RC for MIBC show that despite advances in perioperative care and higher rates of pT0N0M0 following NAC and RC, RFS outcomes have remained stable. Interestingly, even patients who never received NAC either due to treatment era or ineligibility still achieved pT0N0M0 status.7 These findings prompt an important question: could treatment intensity be reduced or de-escalated in select patients without compromising outcomes?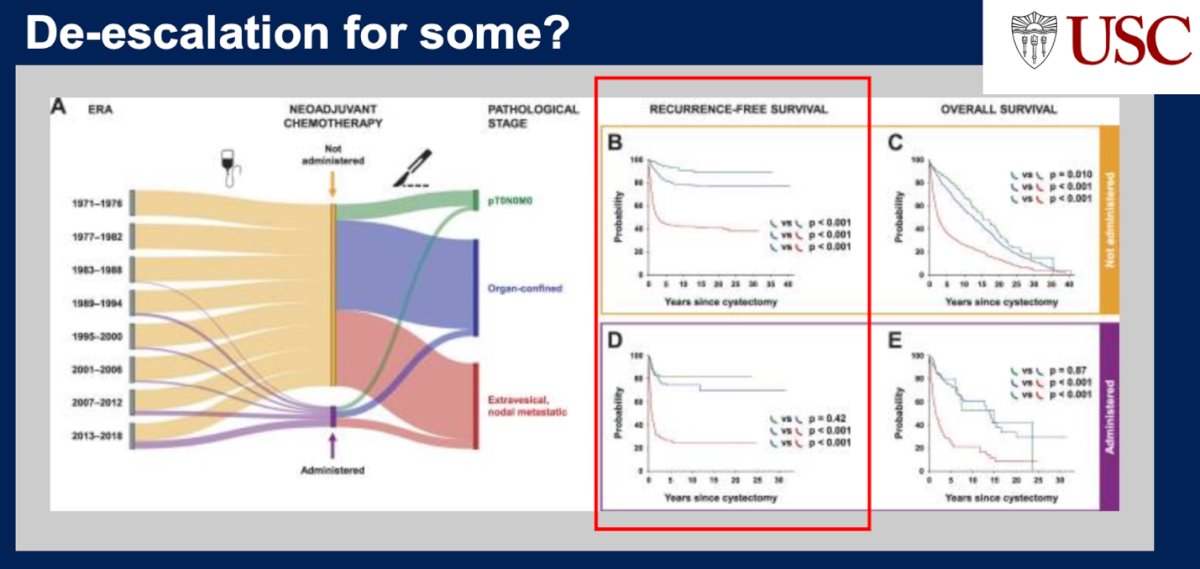
Dr. Schuckman briefly touched on current studies in the adjuvant setting following RC, including CheckMate 274, NIAGARA (perioperative), and AMBASSADOR. In patients with ≥ypT2 or ≥pT3N0 disease, there appears to be a clear EFS and possible OS benefit with adjuvant immunotherapy in both CheckMate 274 and AMBASSADOR. In contrast, ImVigor-010 did not demonstrate a survival benefit.3, 8-10
We need to understand the potential benefit and toxicity of adjuvant therapies. In CheckMate 274, nivolumab showed a 15% EFS and 11% OS benefit at 3 years, though it was associated with a ≥17.9% rate of serious adverse events compared to 7.2% with placebo, and 12.8% of patients discontinued due to adverse events. Moreover, in AMBASSADOR, pembrolizumab has yet to demonstrate an OS benefit possibly due to immune checkpoint inhibitor crossover but showed a DFS benefit (HR 0.69), though SAE rates were high at ≥48%.8-10
In NIAGARA, the combination of neoadjuvant chemotherapy with durvalumab followed by adjuvant durvalumab led to improved pathologic complete response, EFS, and OS, but with notable toxicity: 60% of patients in the adjuvant arm experienced treatment-related adverse events (compared to 6% in the observation group), with 3% experiencing grade ≥3 immune-related events.3
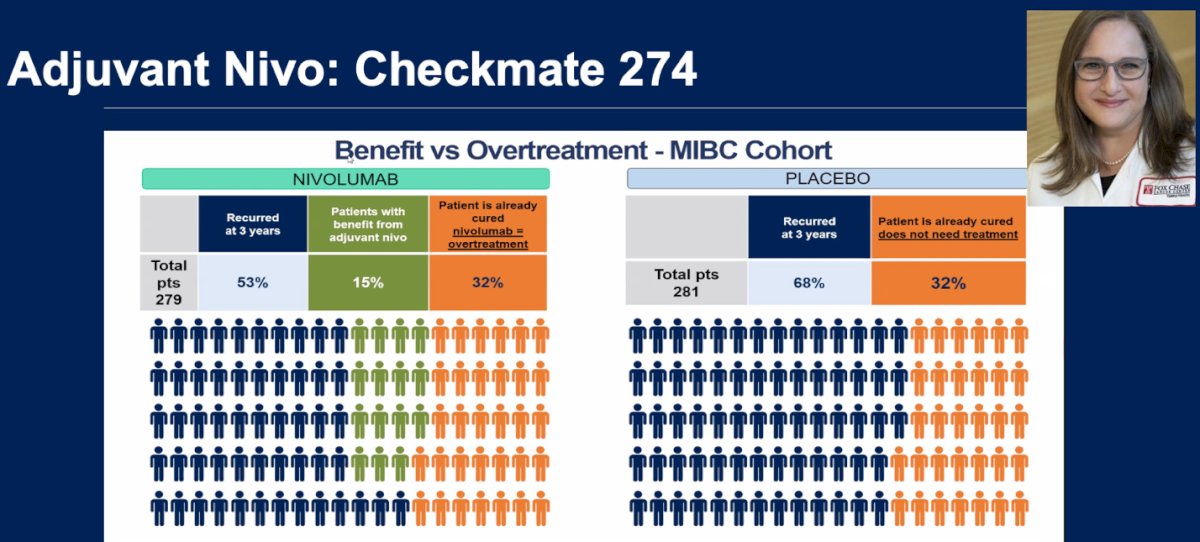
The question remains whether all patients should receive the same adjuvant treatment, and more importantly, how many may be overtreated. At GU ASCO 2025, Dr. Elizabeth Plimack presented an analysis from the CheckMate 274 trial highlighting that approximately 32% of patients in the nivolumab arm may have been overtreated, as they were likely already cured and never experienced recurrence. Similarly, in the placebo arm, about 32% of patients also remained disease-free, suggesting they did not require additional therapy either. These findings underscore the need for better biomarkers or risk-stratification tools to personalize treatment and avoid unnecessary toxicity in patients who may already be cured. Dr. Schuckman noted that while currently we offer this adjuvant IO to everybody, it may only provide benefit to 15% of patients.
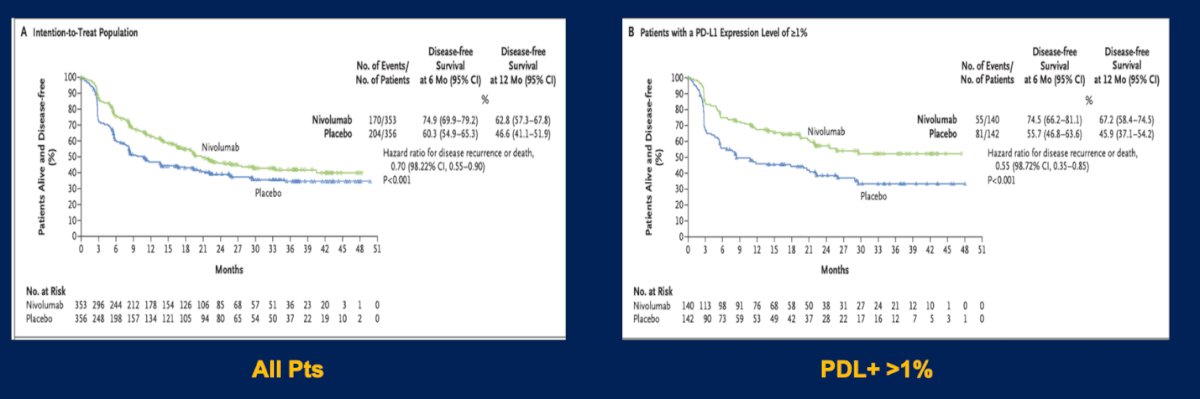
PD-L1 status, particularly expression levels ≥1%, demonstrated potential predictive value in the CheckMate 274 trial.8 Patients with PD-L1 ≥1% who received nivolumab experienced a 45% reduction in the risk of recurrence or death, suggesting a possible role for PD-L1 in guiding adjuvant immunotherapy. In contrast, the AMBASSADOR trial showed a 15-month increase in disease-free survival with adjuvant pembrolizumab, but no clear difference in outcomes was observed based on PD-L1 status across all patients.9 Similarly in NIAGARA there was no observed difference in OS by PDL Status.
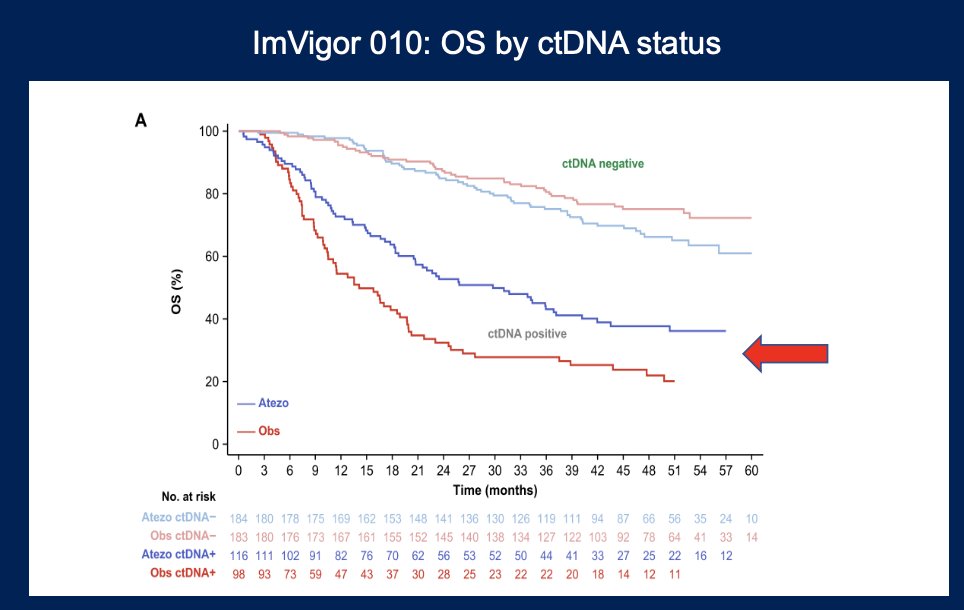
Dr. Schuckman highlighted ctDNA as a promising future biomarker in the perioperative setting. She presented findings from the IMvigor010 trial (adjuvant atezolizumab), where 36% of patients had detectable ctDNA after surgery. While there was no overall difference in DFS between treatment arms, patients with positive ctDNA who received atezolizumab had improved DFS (HR 0.58), suggesting potential benefit in this subgroup. Notably, ctDNA positivity was strongly predictive of recurrence, with a hazard ratio of 6.0 for recurrence compared to ctDNA-negative patients who did not receive treatment.10
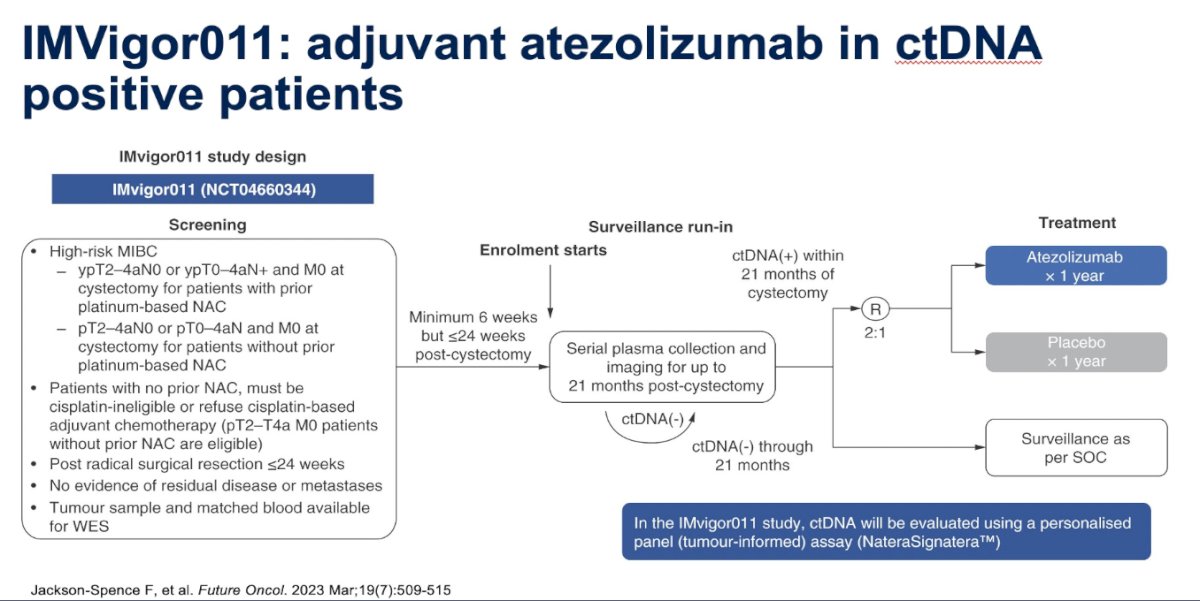
IMvigor011 is a biomarker-selected, randomized phase III trial evaluating adjuvant atezolizumab in patients with MIBC who are ctDNA-positive following RC. Eligible patients must be ctDNA+ within 21 months of surgery and are randomized to receive either atezolizumab or placebo. The trial is specifically designed to assess the utility of ctDNA as a biomarker for guiding adjuvant immunotherapy. The study design is illustrated below.
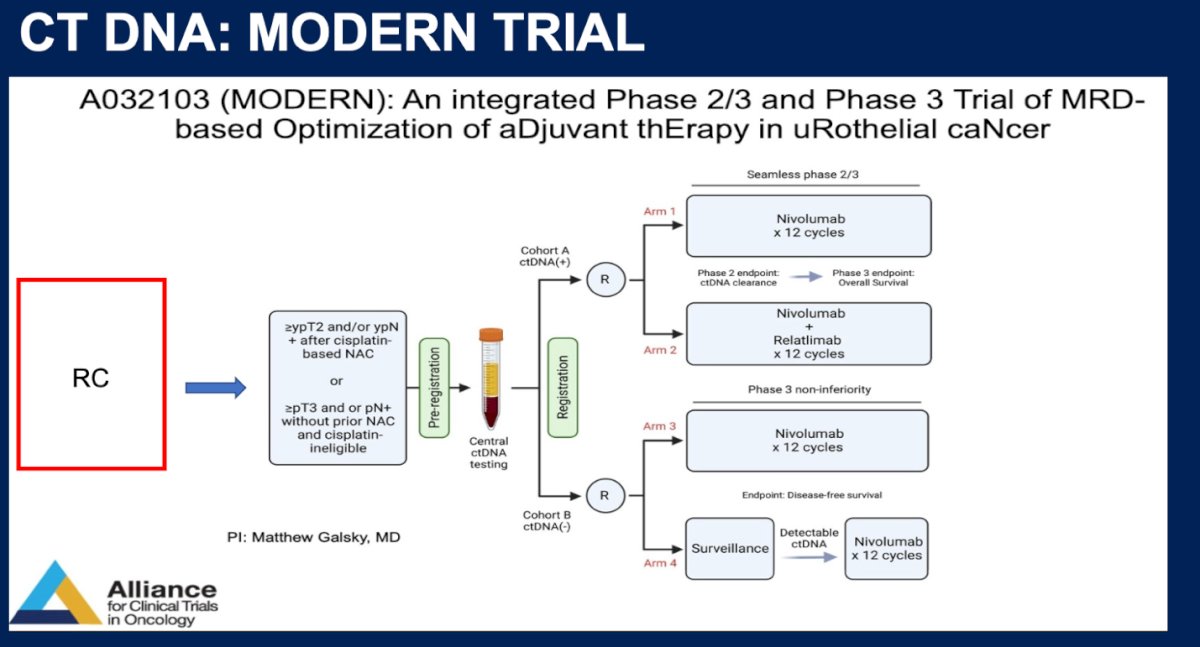
Similarly, the MODERN (A032103) trial is an integrated phase 2/3 study evaluating ctDNA-guided adjuvant immunotherapy in urothelial cancer following RC. Patients with high-risk pathological features either after neoadjuvant chemotherapy or who are cisplatin-ineligible undergo centralized ctDNA testing post-surgery. ctDNA-positive patients are randomized to receive nivolumab alone or in combination with relatlimab, while ctDNA-negative patients are randomized to either surveillance or nivolumab. This trial aims to personalize adjuvant therapy based on molecular residual disease status, with ctDNA clearance and survival outcomes as primary endpoints.
Dr. Schuckman emphasized that one of the most pressing and common questions from patients is: “Do I have to have my bladder out?” This underscores the growing interest in bladder preservation strategies. She highlighted several critical areas under investigation: the role of surgery or radiation therapy after achieving a pT0 response; whether perioperative immunotherapy alone might be sufficient in patients who achieve pT0 without requiring local therapy; and finally, the potential of combining immunotherapy with radiation following intended neoadjuvant chemotherapy.
Retain I (NCT02710734) is a multi-institutional, phase II non-inferiority trial. Patients underwent tumor sequencing prior to NAC to identify mutations in ATM, ERCC2, FANCC, or RB1. Those received ddMVAC for 3 cycles, followed by restaging TURBT. Patients with a complete clinical response (cT0) and a favorable mutation profile were offered active surveillance. Those with residual tumor (cT>0) or without qualifying mutations were directed to intravesical therapy, chemoradiation or radiation therapy. The trial reported a 2-year MFS of 72% in the intention-to-treat population, 65% MFS in the active surveillance group at 41 months (post hoc), and 66% MFS at median 41 months in the ITT population and it was rendered as a negative trial.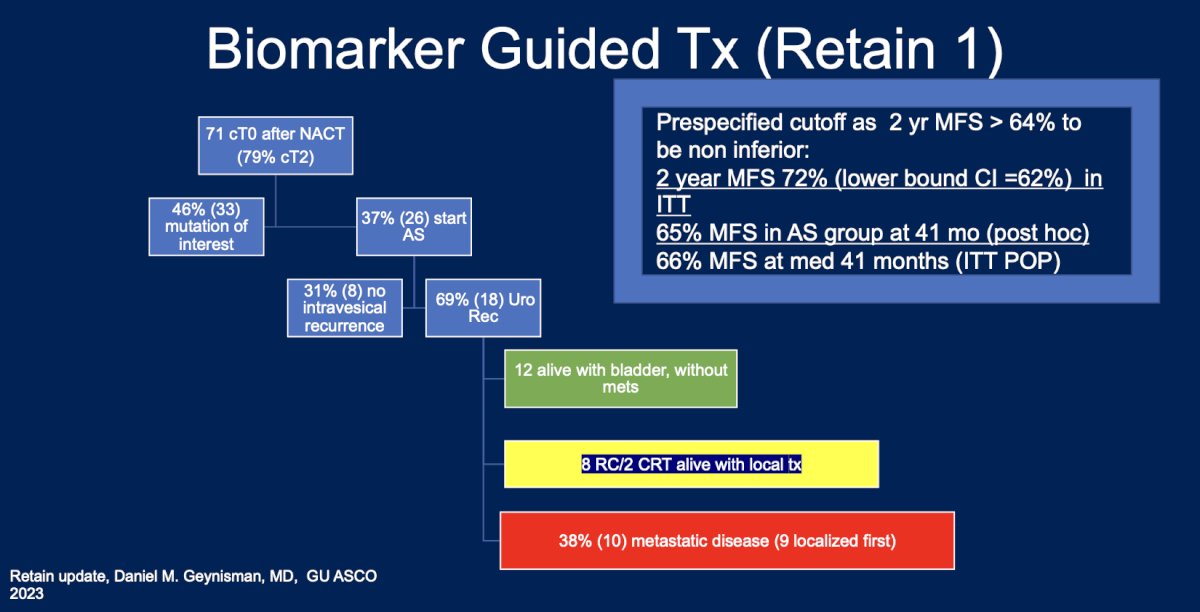
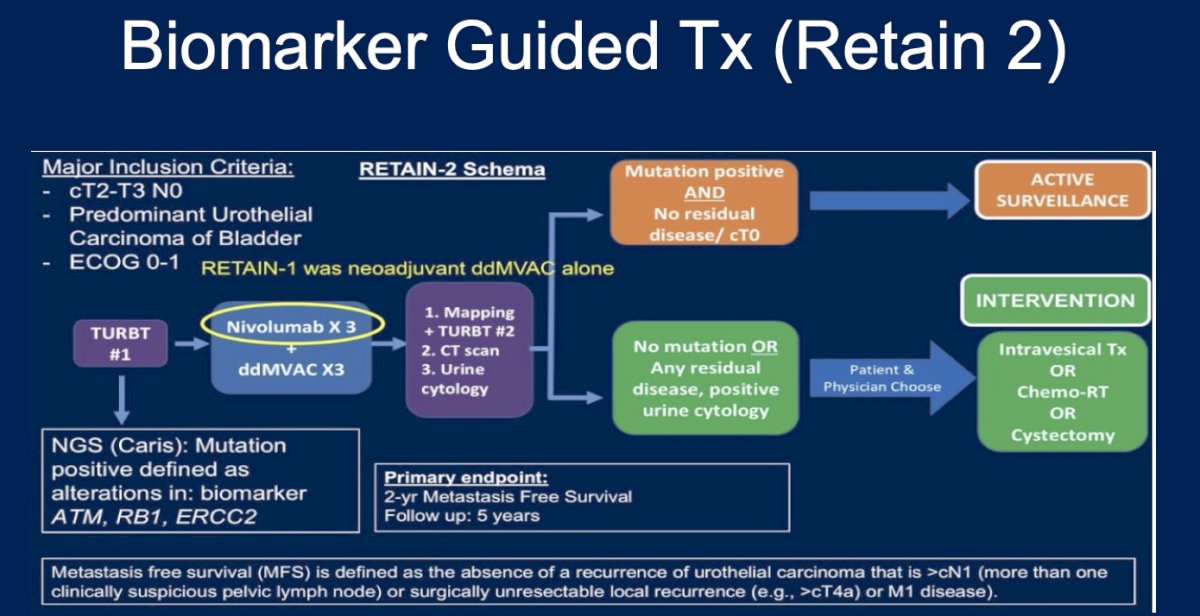
RETAIN-2 is a phase II biomarker-guided trial designed to evaluate a non-operative bladder-preserving strategy for patients with cT2–T3N0 urothelial carcinoma. Patients undergo tumor sequencing (ATM, RB1, ERCC2) and receive neoadjuvant nivolumab plus ddMVAC for three cycles. Restaging includes a repeat TURBT, CT scan, and urine cytology. Patients with both a positive biomarker profile and no residual disease (cT0) are offered active surveillance. Those with residual disease, positive cytology, or without the relevant mutations are directed to standard intervention, including intravesical therapy, chemo-radiation, or cystectomy. The primary endpoint is 2-year metastasis-free survival, with 5 years of follow-up.
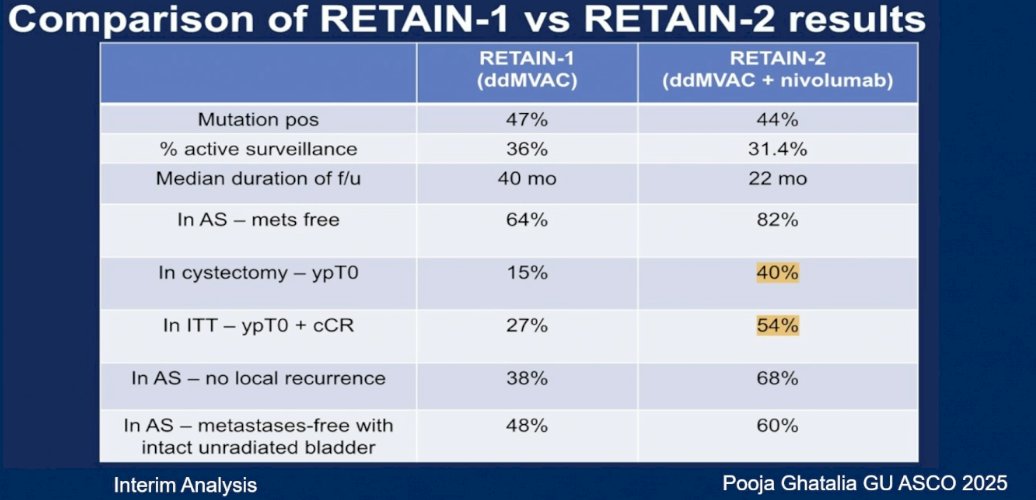
At GU ASCO, a comparison between RETAIN-1 and RETAIN-2 was presented. In RETAIN-2, 40% of patients who underwent cystectomy were found to have ypT0 compared to only 15% in the RETAIN-1 study. Additionally, 54% of patients in the intention-to-treat (ITT) population of RETAIN-2 achieved ypT0 and a cCR status, versus 27% in the ITT population of RETAIN-1. Highlighting fundamental differences between these two trials.
The GU-257 trial evaluates a "sandwich" peri-nonoperative immunotherapy approach in patients with MIBC. This phase II study assesses outcomes in patients who achieve a clinical complete response after neoadjuvant gemcitabine, cisplatin, and nivolumab, followed by maintenance nivolumab. The co-primary endpoints include the cCR rate and the positive predictive value of cCR for 2-year metastasis-free survival in patients who either avoid radical cystectomy or undergo RC with <ypT1N0 disease. Patients undergo rigorous restaging with MRI, biopsy, and cytology; those achieving cT0 are eligible for bladder preservation and receive eight cycles (4 months) of maintenance nivolumab.
In the GU-257 trial, a total of 76 patients were enrolled and randomized. Of these, 33 (43%) achieved a clinical complete response (cT0) following neoadjuvant therapy. Among those who achieved cT0, 8 patients (25%) eventually underwent RC, 2 due to non–muscle-invasive recurrence and 2 due to metastatic progression. Importantly, 25 patients (75% of those who were cT0) remained alive with their bladders intact, supporting the feasibility of a selective bladder-sparing approach in well-selected responders.
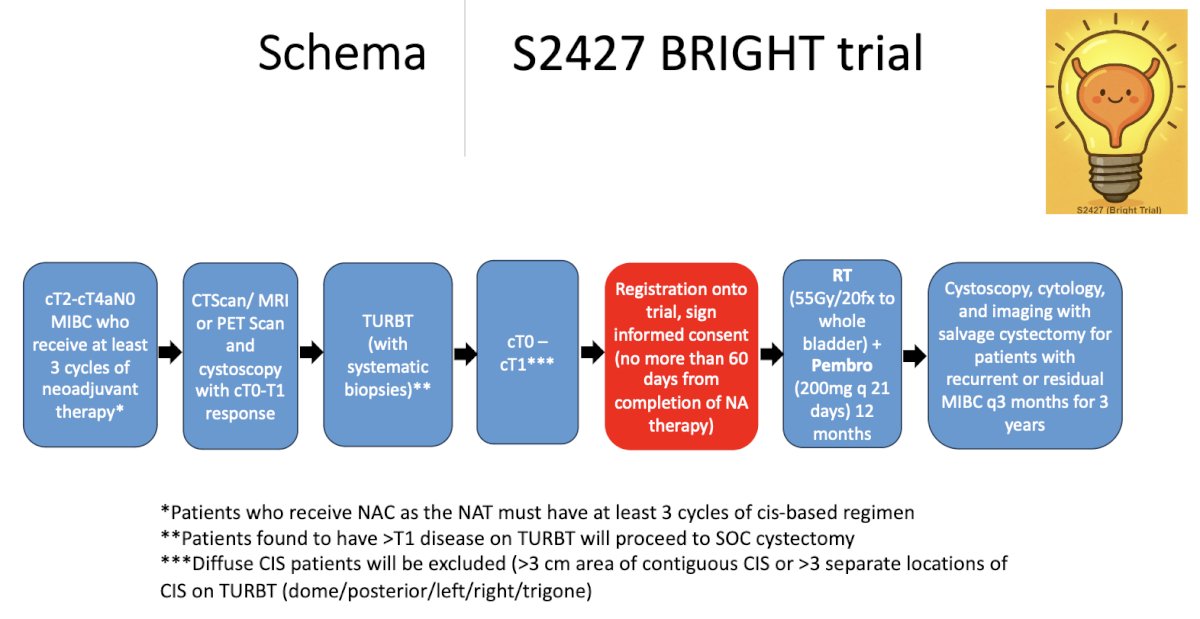
Dr. Schuckman highlighted the S2427 BRIGHT trial, a bladder-preservation study designed for patients with cT2–T4aN0 MIBC who achieve a clinical response (cT0–T1) after receiving at least three cycles of neoadjuvant therapy. After confirming response via imaging and TURBT with systematic biopsies, eligible patients are enrolled within 60 days of completing neoadjuvant therapy. They then receive bladder-directed radiation (55 Gy in 20 fractions) combined with pembrolizumab for 12 months. The study schema is shown below.
Dr. Schuckman closed by emphasizing several unanswered questions that should guide future research in bladder cancer. These include distinguishing the relative benefit of neoadjuvant versus adjuvant immunotherapy, determining when treatment escalation or de-escalation is appropriate, and using biomarkers to guide surveillance in low-risk patients. She also noted the need to better define optimal adjuvant therapy duration, particularly as overtreatment, toxicity, and patient preference remain major barriers to systemic therapy.
Dr. Schuckman concluded her presentation with the following key takeaway points:
- Neoadjuvant cisplatin-based chemotherapy followed by radical cystectomy with risk-adapted immunotherapy remains the standard of care for localized MIBC.
- Biomarkers such as ctDNA and gene mutations (DDR alterations, HER2) show promise for personalizing treatment but are not yet ready for clinical use.
- Future directions include expanding bladder-sparing strategies and incorporating novel agents such as antibody-drug conjugates, which may reshape the treatment landscape for MIBC.
Presented by: Anne K. Schuckman, MD, FACS, Associate Professor of Urology at the University of Southern California, Los Angeles, CA.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30 and June 3.
References:
- Grossman HB, Natale RB, Tangen CM, Speights VO, Vogelzang NJ, Trump DL, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. 2003;349(9):859–66.
- Powles T, Catto JWF, Galsky MD, Al-Ahmadie H, Meeks JJ, Nishiyama H, Vu TQ, Antonuzzo L, Wiechno P, Atduev V, Kann AG, Kim TH, Suárez C, Chang CH, Roghmann F, Özgüroğlu M, Eigl BJ, Oliveira N, Buchler T, Gadot M, Zakharia Y, Armstrong J, Gupta A, Hois S, van der Heijden MS; NIAGARA Investigators. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(19):1773-1786. doi: 10.1056/NEJMoa2408154. Epub 2024 Sep 15. PMID: 39282910.
- Chawdhury et al, Understanding Patient Perspectives in the Management of Their Muscle-Invasive Bladder Cancer. Presented at GU ASCO 2025.
- Necchi A, Anichini A, Raggi D, Briganti A, Massa S, Lucianò R, Colecchia M, Giannatempo P, Mortarini R, Bianchi M, Farè E, Monopoli F, Colombo R, Gallina A, Salonia A, Messina A, Ali SM, Madison R, Ross JS, Chung JH, Salvioni R, Mariani L, Montorsi F. Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients With Muscle-Invasive Urothelial Bladder Carcinoma (PURE-01): An Open-Label, Single-Arm, Phase II Study. J Clin Oncol. 2018 Dec 1;36(34):3353-3360. doi: 10.1200/JCO.18.01148. Epub 2018 Oct 20. PMID: 30343614.
- Pfister C, Gravis G, Fléchon A, Soulié M, Guy L, Laguerre B, Mottet N, Joly F, Allory Y, Harter V, Culine S; VESPER Trial Investigators. Randomized Phase III Trial of Dose-dense Methotrexate, Vinblastine, Doxorubicin, and Cisplatin, or Gemcitabine and Cisplatin as Perioperative Chemotherapy for Patients with Muscle-invasive Bladder Cancer. Analysis of the GETUG/AFU V05 VESPER Trial Secondary Endpoints: Chemotherapy Toxicity and Pathological Responses. Eur Urol. 2021 Feb;79(2):214-221. doi: 10.1016/j.eururo.2020.08.024. Epub 2020 Aug 28. PMID: 32868138.
- Szabados B, Kockx M, Assaf ZJ, van Dam PJ, Rodriguez-Vida A, Duran I, Crabb SJ, Van Der Heijden MS, Pous AF, Gravis G, Herranz UA, Protheroe A, Ravaud A, Maillet D, Mendez MJ, Suarez C, Linch M, Prendergast A, Tyson C, Stanoeva D, Daelemans S, Rombouts M, Mariathasan S, Tea JS, Mousa K, Sharma S, Aleshin A, Banchereau R, Castellano D, Powles T. Final Results of Neoadjuvant Atezolizumab in Cisplatin-ineligible Patients with Muscle-invasive Urothelial Cancer of the Bladder. Eur Urol. 2022 Aug;82(2):212-222. doi: 10.1016/j.eururo.2022.04.013. Epub 2022 May 14. PMID: 35577646.
- Mitra AP, Cai J, Miranda G, Bhanvadia S, Quinn DI, Schuckman AK, Djaladat H, Daneshmand S. Management Trends and Outcomes of Patients Undergoing Radical Cystectomy for Urothelial Carcinoma of the Bladder: Evolution of the University of Southern California Experience over 3,347 Cases. J Urol. 2022 Feb;207(2):302-313. doi: 10.1097/JU.0000000000002242. Epub 2021 Nov 8. PMID: 34994657; PMCID: PMC8746892.
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021;384(22):2102–2114.
- Powles T, Kopyltsov E, Hwang EC, et al. Adjuvant pembrolizumab versus observation in muscle-invasive urothelial carcinoma (AMBASSADOR): a phase 3, randomized, open-label trial. J Clin Oncol. 2024;42(4_suppl):LBA531.
- Bellmunt J, Hussain M, Gschwend JE, et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021;22(4):525–537.
- Jensen JB, Nielsen ME, Osther PJ, et al. Circulating tumor DNA-guided adjuvant immunotherapy in muscle-invasive bladder cancer: the TOMBOLA trial. Eur Urol. 2024;85(5):567–576.
- Smith ZL, Patel HD, Johnson MH, et al. MODERN: a phase 2/3 randomized trial of ctDNA-guided adjuvant immunotherapy in muscle-invasive bladder cancer. J Clin Oncol. 2025;43(5_suppl):LBA552.