(UroToday.com) The 2025 ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Kevin Reyes discussing circulating tumor DNA (ctDNA) monitoring in patients with advanced urothelial carcinoma treated with enfortumab vedotin +/- pembrolizumab. ctDNA is an emerging biomarker in advanced urothelial carcinoma, but its role for patients receiving enfortumab vedotin + pembrolizumab is unclear.
The investigators undertook a retrospective analysis of patients with advanced urothelial carcinoma who were longitudinally tested for ctDNA (MTM/mL) with a tumor-informed assay while on treatment with enfortumab vedotin +/- pembrolizumab. Patient data were abstracted from the electronic medical record, and outcomes were compared based on changes in ctDNA from pre-treatment baseline, using Kaplan-Meier method and Cox proportional hazards test to assess progression free survival and overall survival.
Longitudinal ctDNA data were available for 36 patients (treatment: 28 enfortumab vedotin + pembrolizumab; 8 enfortumab vedotin) between August 2022 and November 2024. Patients had a median of 3 ctDNA tests (range: 2-14) over 8 months of median follow-up. At pre-treatment baseline, 33/36 (92%) patients had detectable ctDNA. Patient characteristics and outcomes are shown in the following table:
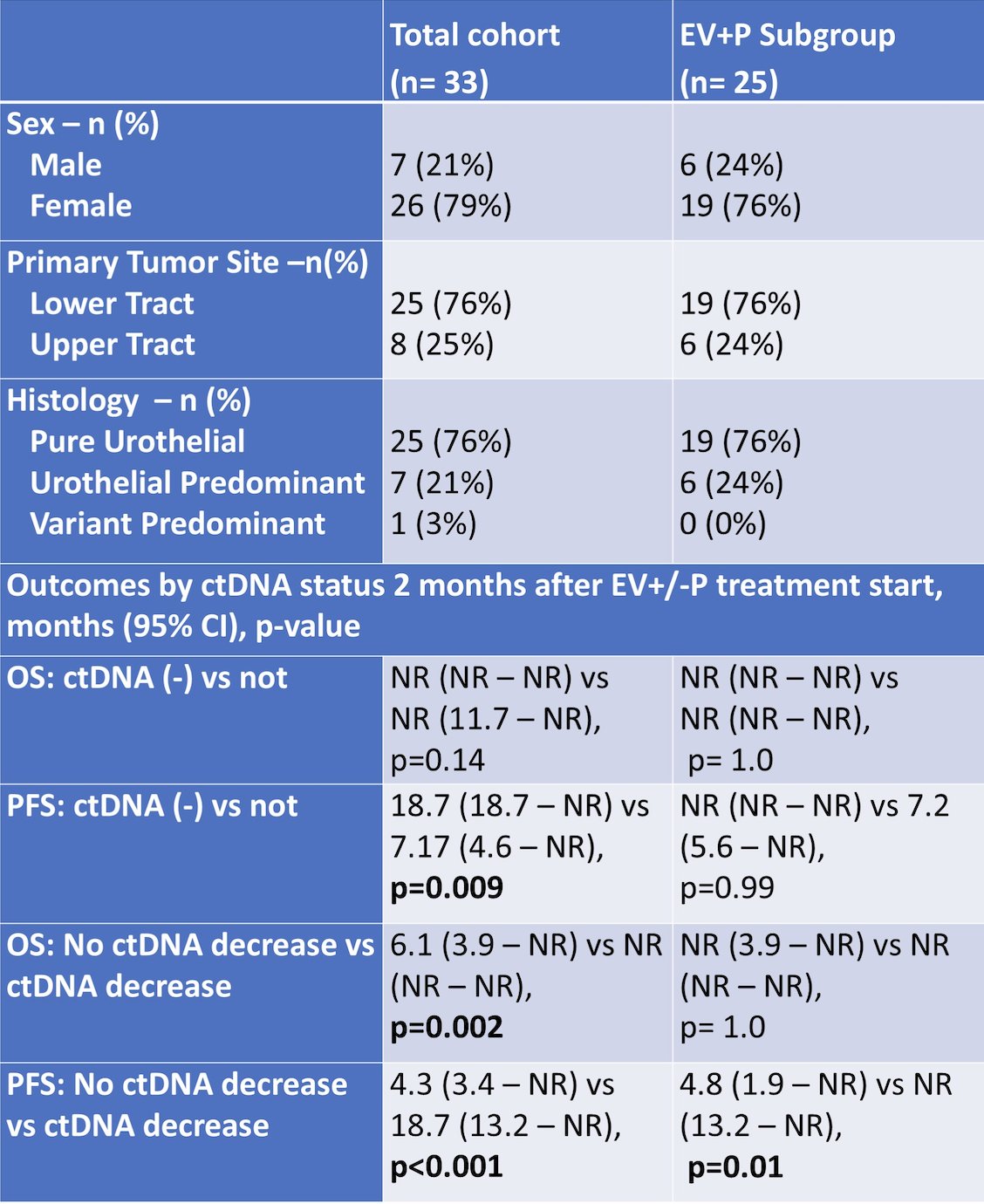
After treatment start, 26 patients (79%) had a decrease in ctDNA (median time to decrease 50 days), and 11 patients (33%) achieved negative ctDNA (-) after a median of 54 days. The 11 patients with ctDNA (-) had a response rate of 91% (complete response: 6, partial response: 4, stable disease: 1). Among 14 patients with ctDNA nadir followed by a rise, 8 patients (57%) had progressive disease on next scan, and median time from initial ctDNA rise to progressive disease was 124 days. Patients who achieved ctDNA (-) within 2 months of treatment (n = 8) had improved progression free survival relative to patients with ctDNA data (n = 21) who did not (HR 0.08, 95% CI 0.01 – 0.59, p = 0.01). Patients with no decrease in ctDNA within 2 months of treatment start (n = 7) had inferior progression free survival (HR 5.9, 95% CI 1.9 – 19.2, p < 0.01) and overall survival (HR 20.8, 95% CI 2.3 – 192, p < 0.01) versus patients with a ctDNA decrease (n = 22):
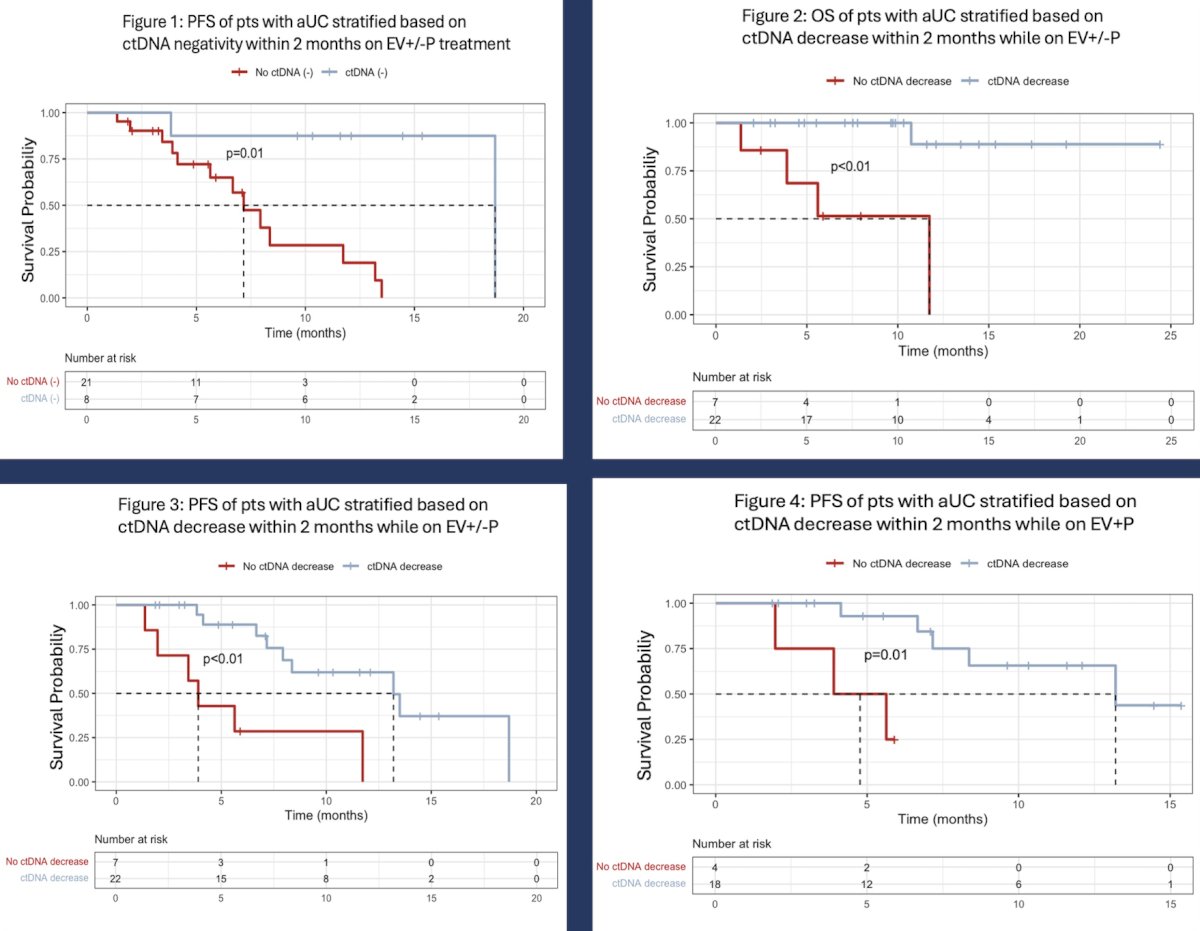
In the enfortumab vedotin + pembrolizumab group, patients with no ctDNA decrease within 2 months (n = 4) had inferior progression free survival (HR 15.9, 95% CI 1.6 - 154, p = 0.01) versus patients with a decrease (n = 18).
Dr. Reyes concluded his presentation discussing circulating tumor DNA monitoring in patients with advanced urothelial carcinoma treated with enfortumab vedotin +/- pembrolizumab with the following take home points:
- In this retrospective analysis of patients treated with enfortumab vedotin +/- pembrolizumab, 92% had detectable ctDNA and 79% had a ctDNA decrease after treatment start
- Within 2 months of treatment start, patients who achieved ctDNA (-) had improved progression free survival, while patients who did not have ctDNA decrease had inferior progression free survival and overall survival
- These hypothesis-generating results warrant validation in larger prospective cohorts and can inform clinical decision-making
Presented by: Kevin R. Reyes, MD, UCSF, San Francisco, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.