(UroToday.com) The 2025 ASCO annual meeting featured a urothelial carcinoma oral abstract session and a presentation by Dr. Michiel van der Heijden discussing final results for cisplatin-ineligible patients from the CheckMate 901 trial assessing nivolumab + ipilimumab versus gemcitabine + carboplatin chemotherapy for previously untreated unresectable or metastatic urothelial carcinoma.
Cisplatin-based chemotherapy was the standard of care for unresectable or metastatic urothelial carcinoma for decades, but patients ineligible for cisplatin have historically worse outcomes and are treated with gemcitabine + carboplatin. Treatment options for metastatic urothelial carcinoma have expanded with the emergence of immune checkpoint inhibitors, including the recent approvals of enfortumab vedotin + pembrolizumab and nivolumab + chemotherapy in the first line setting. However, the role of anti-PD-1 + anti-CTLA-4 has not been established in metastatic urothelial carcinoma. The phase 3, global, open-label, randomized CheckMate 901 trial compared nivolumab + ipilimumab versus gemcitabine + carboplatin in cisplatin-ineligible patients with previously untreated unresectable or metastatic urothelial carcinoma.1 At the 2025 ASCO annual meeting, Dr. van der Heijden presented the final results of CheckMate 901.
Patients with previously untreated, histologically confirmed, unresectable or metastatic urothelial carcinoma who were cisplatin-ineligible (glomerular filtration rate ≥ 30 to < 60 mL/min) were randomized 1:1 to nivolumab 1 mg/kg + ipilimumab 3 mg/kg every 3 weeks up to 4 cycles, then nivolumab 480 mg every 4 weeks until disease progression/unacceptable toxicity or up to 2 years, or to gemcitabine + carboplatin every 3 weeks for up to 6 cycles: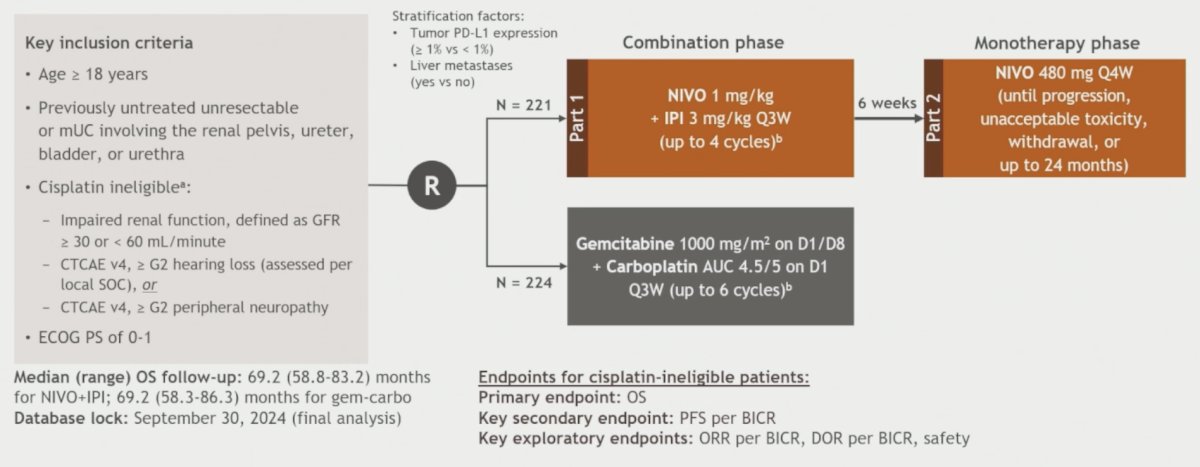
Patients were stratified by tumor PD-L1 expression and liver metastasis. The primary endpoint was overall survival, and progression-free survival by blinded independent central review (BICR) was a secondary endpoint. Objective response rate per BICR, duration of response per BICR, and safety were exploratory outcomes.
There were 445 patients randomized (nivolumab + ipilimumab, n = 221; gemcitabine + carboplatin, n = 224). The baseline characteristics in cisplatin ineligible patients is highlighted as follows: 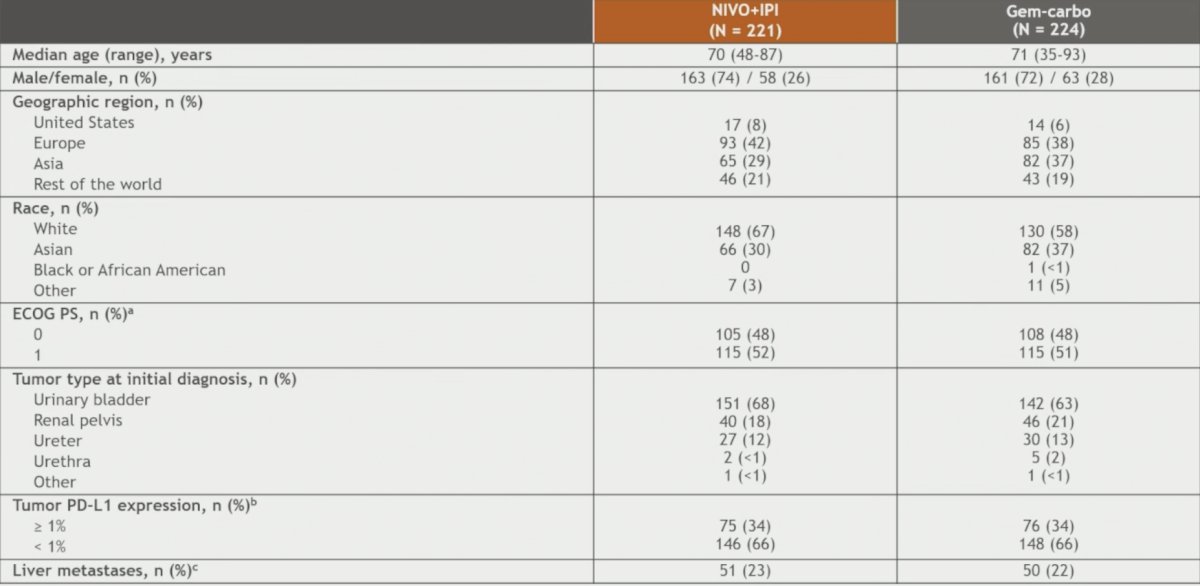
The median time to treatment discontinuation was 2.2 (2.1–3.5 95% CI) months with nivolumab + ipilimumab versus 3.8 (3.5–3.9 95% CI) months with gemcitabine + carboplatin. A total of 119 (55%) patients had a duration of treatment with nivolumab + ipilimumab less than 3 months: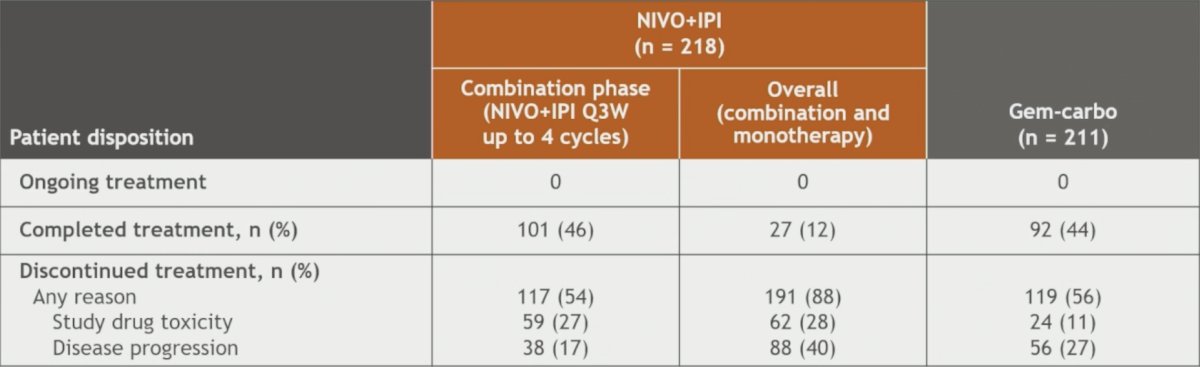
After minimum follow-up (58.3 months), the primary endpoint of overall survival did not meet the threshold for significance: median 19.1 months with nivolumab + ipilimumab versus 13.2 months with gemcitabine + carboplatin (HR 0.79, 98.27% CI, 0.61–1.01; p = 0.0245):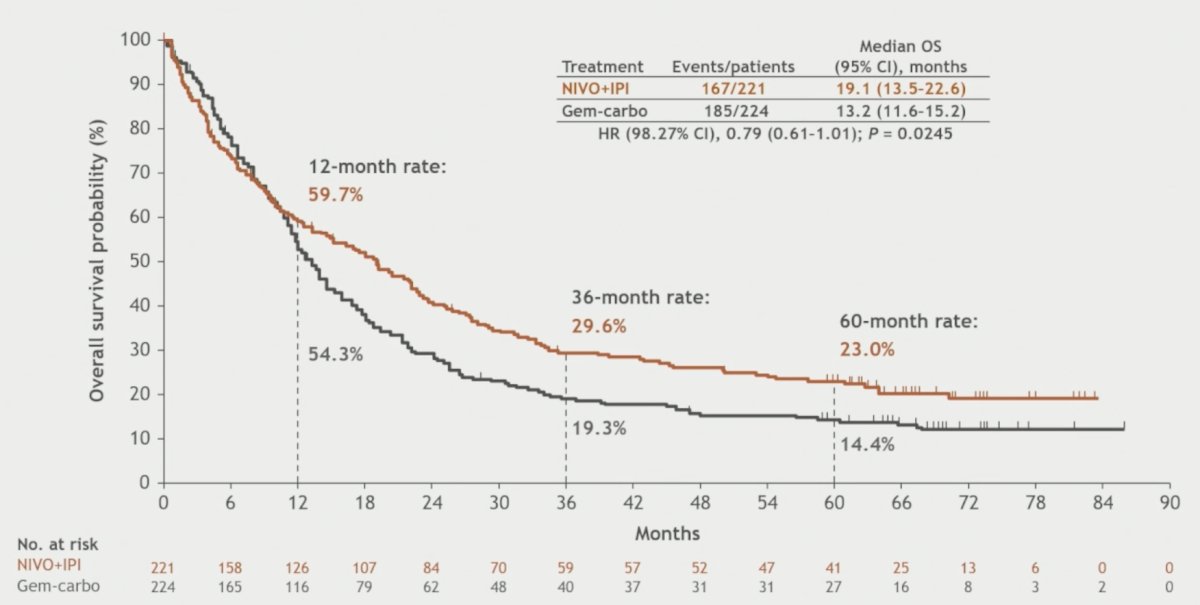
Overall survival in cisplatin-ineligible subpopulations is noted: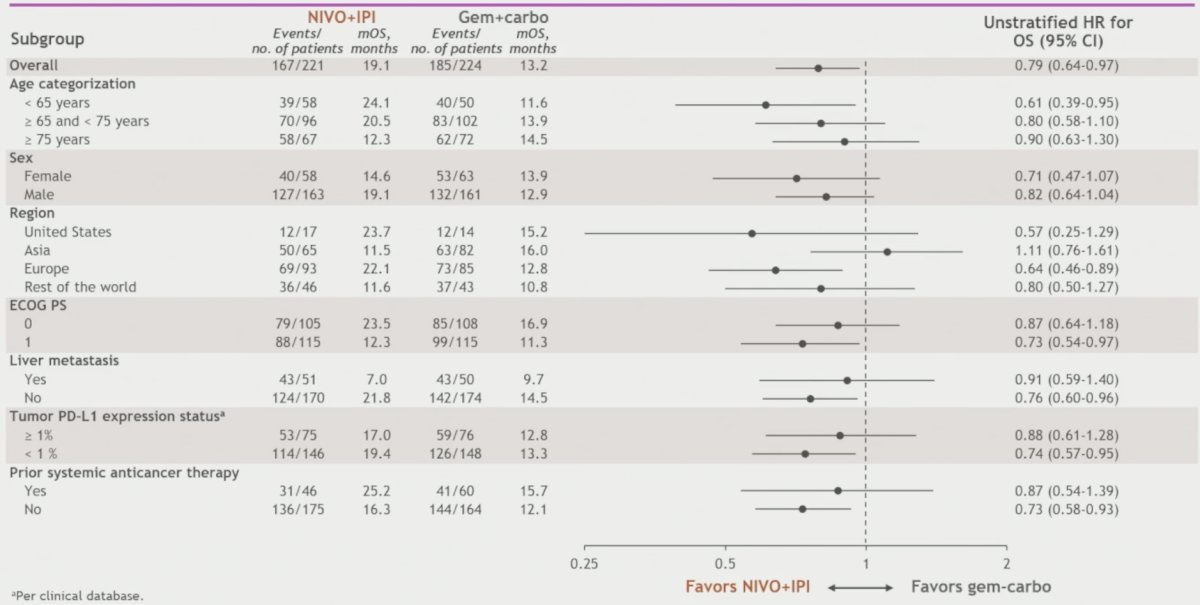
Dr. Van der Heijden also reported overall survival in PD-L1 >=1% and all randomized patients (cisplatin-eligible and cisplatin-ineligible patients): the hazard ratio for overall survival in PD-L1 >= 1% (primary endpoint) patients was 0.87 (97.48% 0.61-1.23) and for all randomized patients (secondary endpoint) was 0.78 (95% CI 0.66-0.92):

Progression-free survival in the cisplatin-ineligible patients (secondary endpoint) was also not statistically significant (HR 0.90, 95% CI 0.72-1.12):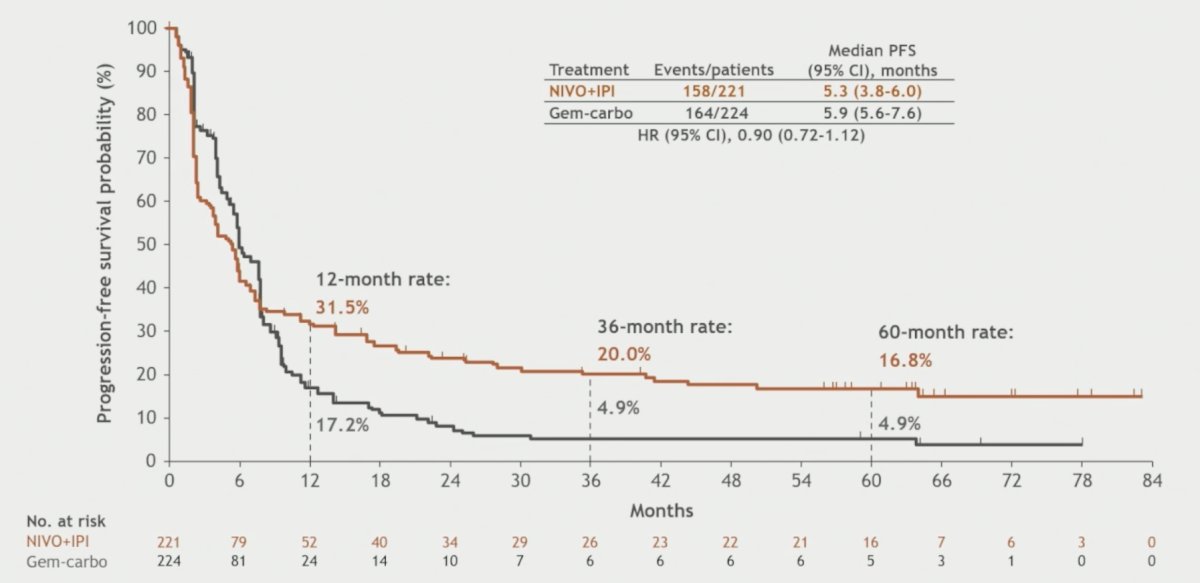
Objective response rates were 35.3% for patients receiving nivolumab + ipilimumab versus 38.8% for those receiving gemcitabine + carboplatin. Time to and duration of responses favored the nivolumab + ipilimumab arm: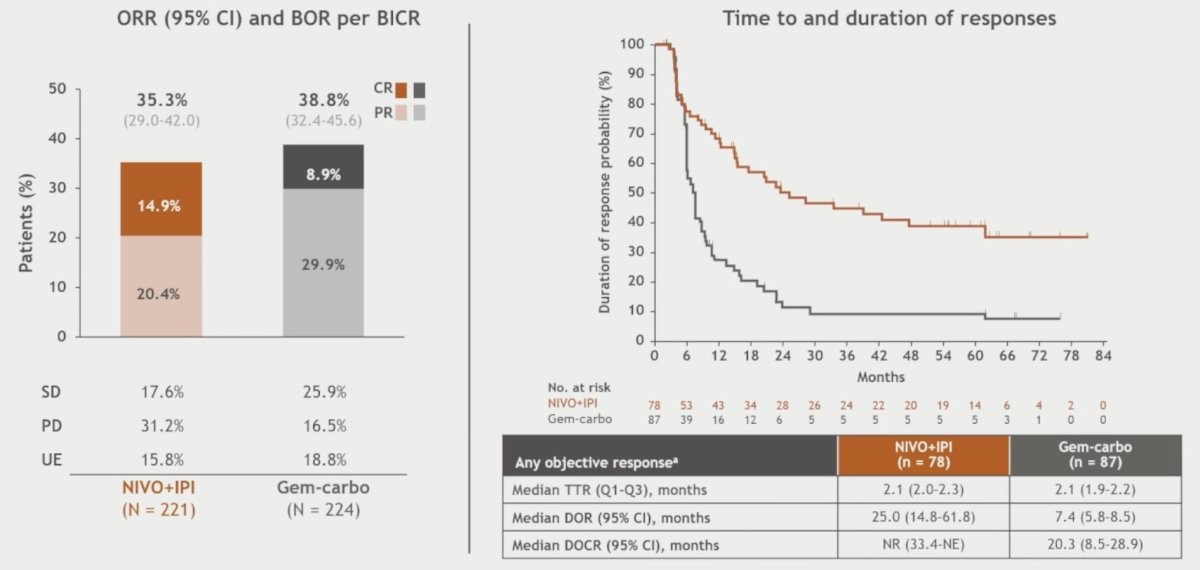
The treatment free interval and response outcomes among cisplatin-ineligible patients with complete response are highlighted below:
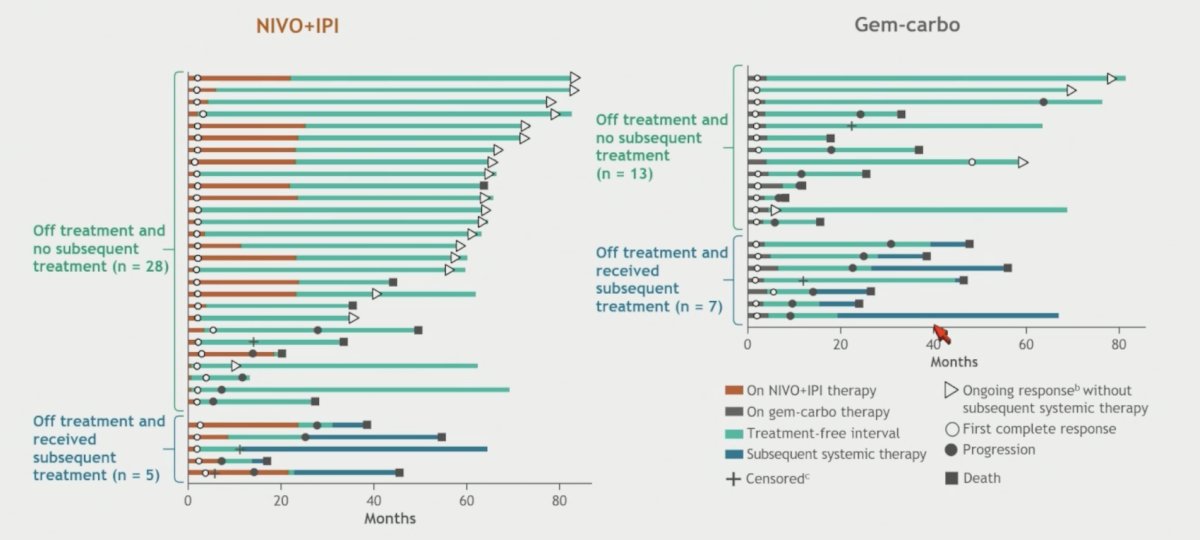
Among subsequent systemic therapy in the cisplatin-ineligible patients, the most commonly used was platinum-based chemotherapy in the nivolumab + ipilimumab arm, compared to anti-PD-1 therapy in the gemcitabine + carboplatin arm: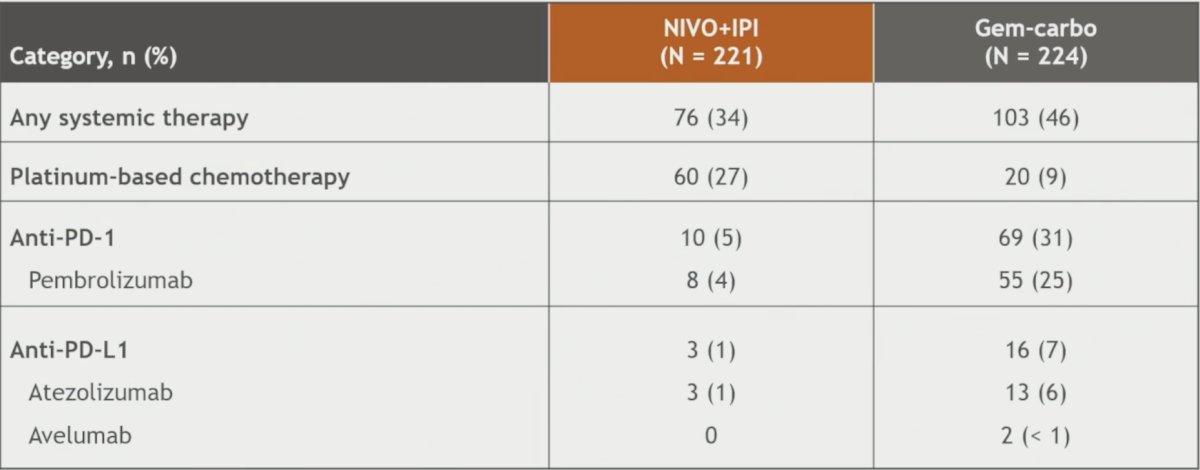
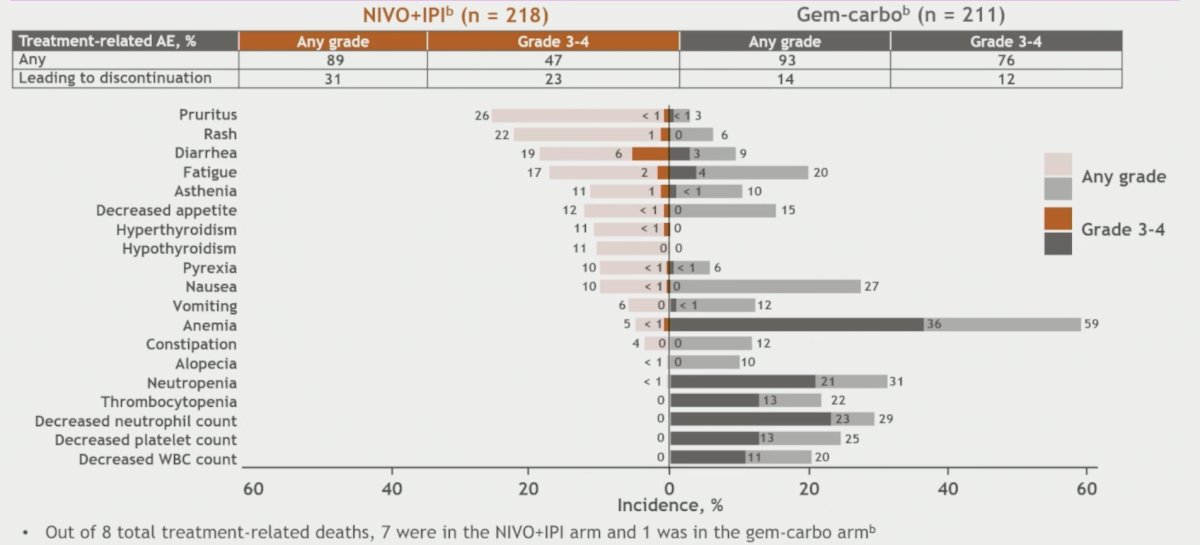
Any-grade treatment-related adverse events occurred in 89.0% (grade 3–4, 47.2%) of nivolumab + ipilimumab-treated and 92.9% (grade 3–4, 76.3%) of gemcitabine + carboplatin-treated patients. Any-grade treatment-related adverse events leading to discontinuation occurred in 31.2% and 14.2% of patients, respectively. There were 8 deaths related to toxicity (7 - nivolumab + ipilimumab; 1 - gemcitabine + carboplatin):
Dr. van der Heijden concluded his presentation discussing final results for cisplatin-ineligible patients from the CheckMate 901 trial with the following take-home points:
- The prespecified thresholds for statistical significance were not met for the dual primary endpoints of overall survival in cisplatin-ineligible and tumor PD-L1 >=1% patients
- For cisplatin-ineligible patients, the hazard ratio was 0.79 (p = 0.0245, p value boundary of 0.0173)
- For tumor PD-L1 >=1% patients, the hazard ratio was 0.87 (p = 0.364, p value boundary of 0.0252)
- Durable response with nivolumab + ipilimumab and favorable landmark overall survival after 12 months show meaningful activity from a chemotherapy-free regimen in cisplatin-ineligible patients
- The safety profile of nivolumab + ipilimumab was consistent with that observed in other studies and no new safety signals were identified
Presented by: Michiel S. van der Heijden, MD, PhD, Netherlands Cancer Institute, Amsterdam, The Netherlands
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: Exploring Immunotherapy Outcomes in Cisplatin-Ineligible Bladder Cancer - Michiel Van Der Heijden
References:
- Van der Heijden MS, Sonpavde G, Powles T, et al. Nivolumab plus Gemcitabine-Cisplatin in Advanced Urothelial Carcinoma. N Engl J Med. 2023 Nov 9;389(19):1778-1789.