(UroToday.com) The 2025 ASCO annual meeting featured a urothelial carcinoma rapid oral abstract session and a presentation by Dr. Andrea Necchi discussing the first results of SURE-02, a phase 2 study of neoadjuvant sacituzumab govitecan + pembrolizumab, followed by response-adapted bladder sparing and adjuvant pembrolizumab, in patients with muscle invasive bladder cancer.
Standard of care for muscle invasive bladder cancer is radical cystectomy with neoadjuvant chemotherapy, but ~50% of patients are ineligible for/refuse chemotherapy and survival for radical cystectomy alone is dismal. Neoadjuvant pembrolizumab and sacituzumab govitecan monotherapies showed activity in muscle invasive bladder cancer within PURE-011 and SURE-01 studies. SURE-02 is a phase 2 study of neoadjuvant sacituzumab govitecan + pembrolizumab and adjuvant pembrolizumab, including a bladder-sparing approach depending on clinical response. At the 2025 ASCO annual meeting, Dr. Necchi and colleagues reported results of a prespecified interim analysis.
Patients age ≥18 years, ECOG performance status 0-1, with histologically confirmed cT2-T4N0M0 muscle invasive bladder cancer, ineligible/refusing chemotherapy, and scheduled for radical cystectomy received 4 cycles of pembrolizumab 200 mg on day 1 and sacituzumab govitecan 7.5 mg/kg on day 1 and day 8, every 3 weeks, followed by postsurgical pembrolizumab x 13 cycles, every 3 weeks. A re-TURBT is allowed instead of radical cystectomy, followed by pembrolizumab x 13 cycles, for patients achieving a clinical complete response, stringently defined as a negative MRI and no residual viable tumor at re-TURBT (ypT0). The trial design for SURE-02 is as follows:
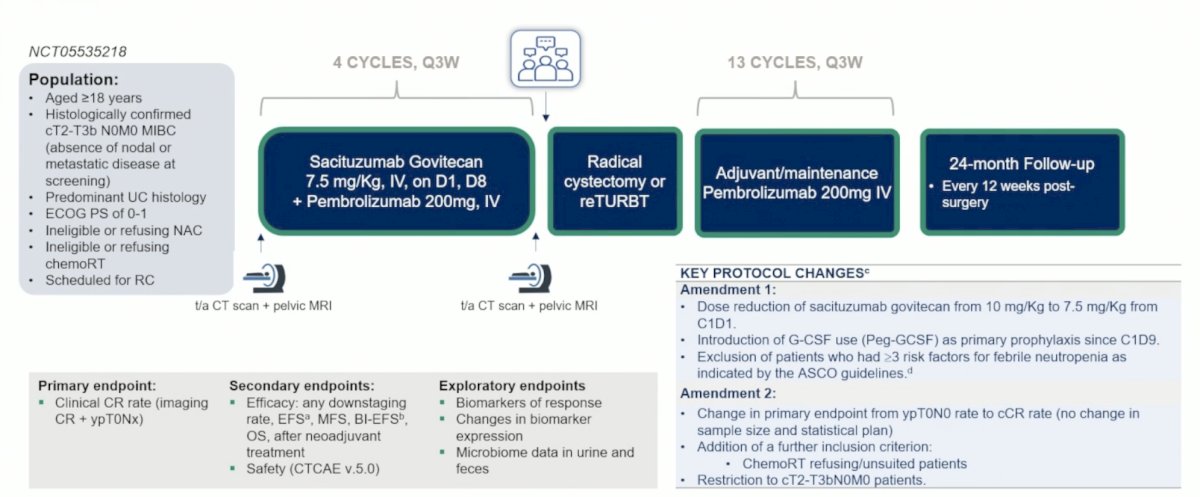
The primary outcome measure is clinical complete response rate, and other outcomes include ypT≤1N0-x rate including patients undergoing radical cystectomy, safety (CTCAE v.5.0), survival. The total sample size is 48 patients in a 2-stage design, with 23 patients enrolled at first stage (≥7 clinical complete response needed). Decipher Bladder was used for transcriptome-wide analyses of primary TURBT tissue.
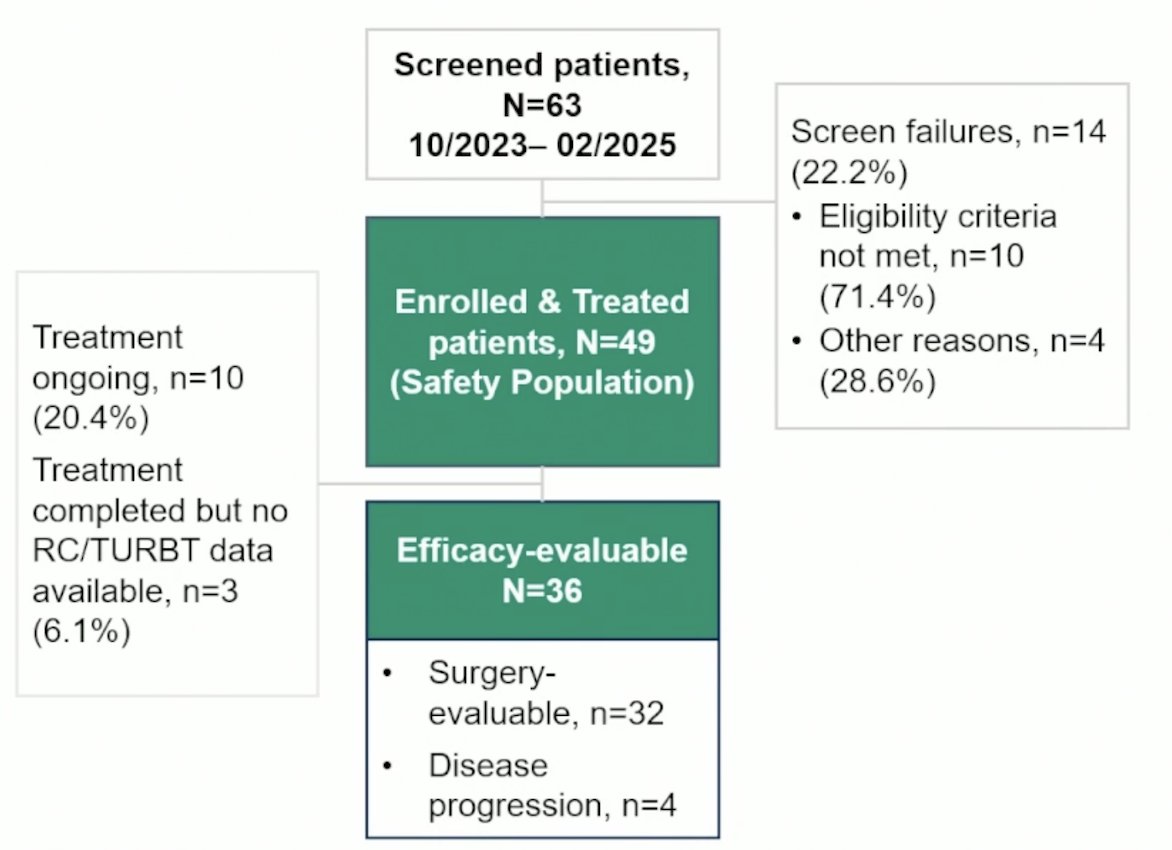
From October 2023 to February 2025, 49 patients were treated and 36 were efficacy evaluable:
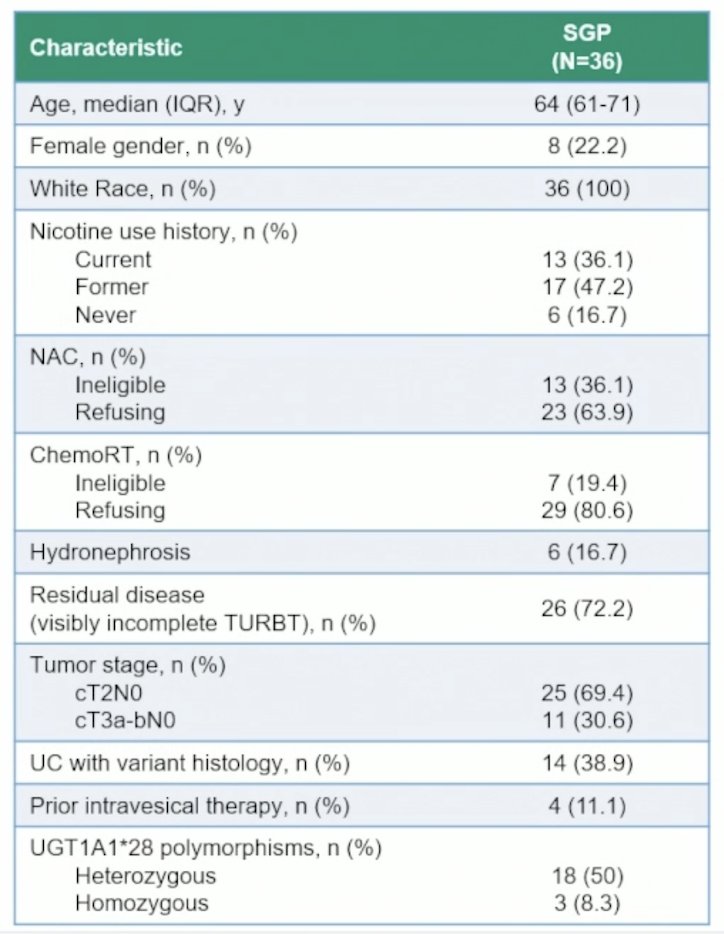
Overall, 25 (69.4%) patients had a cT2 stage and 14 (38.9%) had a centrally confirmed variant histology:
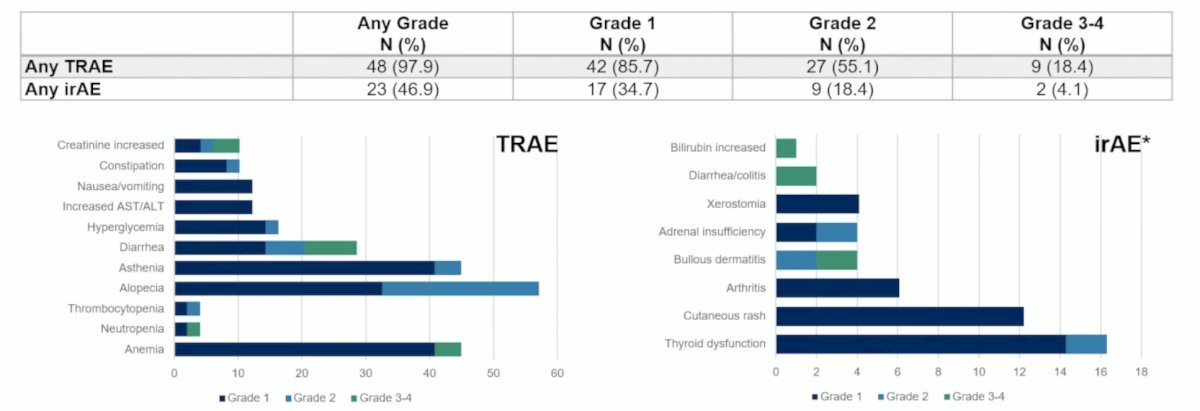
Grade ≥3 treatment-related adverse-events occurred in 9 patients (18.4%), 3 dose omissions of sacituzumab govitecan and 4 dose delays (1 week) were recorded. No sacituzumab govitecan dose-reduction was needed:
The clinical complete response-rate was 44.4% (n = 16; 95% CI: 27.9-61.9), of which all of these patients underwent a re-TURBT, with a ypT≤1N0-x rate of 55.6% (n =20):
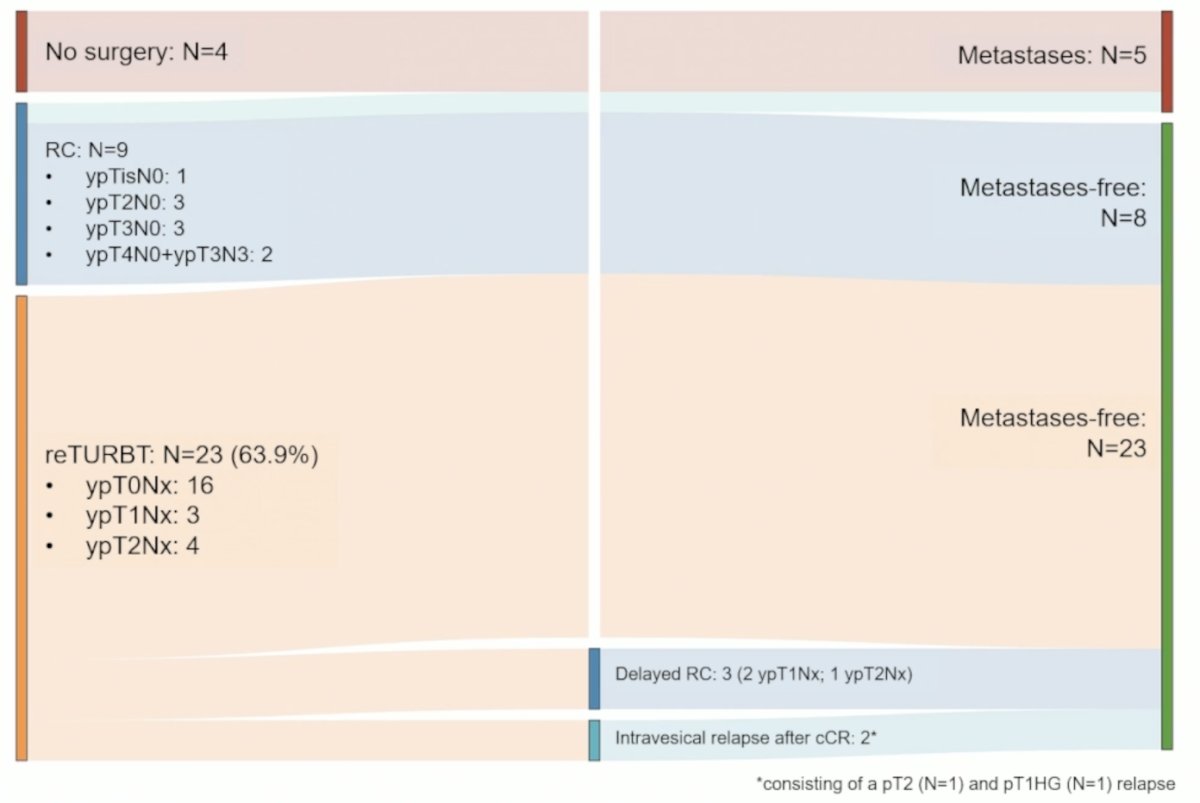
Over a median follow-up of 10 months (IQR 7.3-13), the 12 month event free survival rate was 71.3% (95% CI 55.7-91.2), the 12 month metastasis free survival rate was 84.2% (95% CI 72-98.5), the 12 month bladder intact event free survival in patients with a clinical complete response was 100%, and the 12 month bladder intact event free survival in re-TURBT patients (n = 23) was 74% (95% CI 54.8 – 99). The landscape of genomic alterations in baseline TURBT samples in clinical complete response versus non clinical complete response patients is as follows:
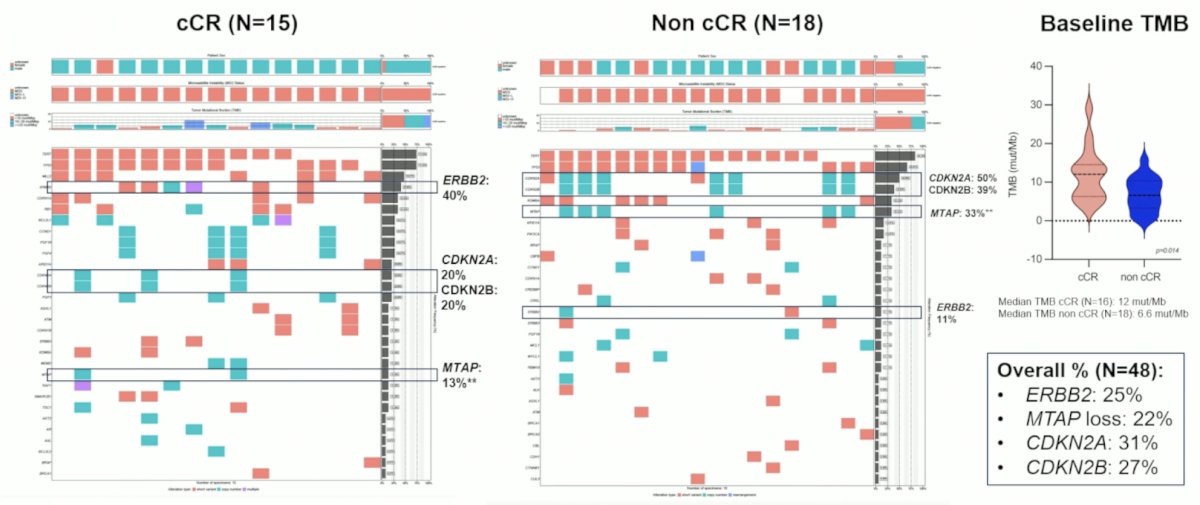
Transcriptome results showed that complete pathologic (ypT0) responses varied by Genomic Subtyping Classifier groups with luminal tumors showing higher ypT0 rates versus non-luminal (73 versus 25%, p = 0.04). Similarly, based on Lund subtypes, genomically unstable tumors had ypT0 response in 67%, compared to 57% for urothelial-like, 20% for basal/squamous, and 0% for neuroendocrine-like. Higher stromal signature (> median) was associated with non-ypT0 response (p = 0.004), while neither Trop2 (p = 0.15) nor TOP1 (p = 0.79) gene expression were associated with ypT0 response.
Dr. Necchi concluded his presentation discussing the first results of SURE-02 with the following take home points:
- Perioperative sacituzumab govitecan + pembrolizumab revealed a compelling clinical complete response rate (44%), with a manageable safety profile, allowing a bladder preservation in 74% of patients refusing radical cystectomy
- The SURE-02 trial provided a safe and effective approach in patients who had no standard of care therapy at the time of radical cystectomy refusal
- Interim translational findings revealed putative tumor biomarkers associated with both therapeutic components: luminal subtype recapitulated features associated with sacituzumab govitecan response
- Limitations are primarily represented by the interim nature of the results and the relatively small numbers
Presented by: Andrea Necchi, MD, IRCCS San Raffaele Hospital, Vita-Salute San Raffaele University, Milan, IT
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: SURE-02 Trial: A Patient-Driven, Bladder-Sparing Approach for MIBC - Andrea Necchi
References:
- Necchi A, Anichini A, Raggi D, et al. Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients with Muscle-Invasive Urothelial Bladder Carcinoma (PURE-01): An Open-Label, Single-Arm, Phase II Study. J Clin Oncol 2018 Dec 1;36(34):3353-3360.