(UroToday.com) The 2025 ASCO annual meeting featured a urothelial carcinoma oral abstract session and a presentation by Dr. Jeannie Hoffman-Censits discussing an interim analysis from the JAVELIN Bladder Medley phase 2 trial assessing avelumab + sacituzumab govitecan versus avelumab monotherapy as first-line maintenance treatment in patients with advanced urothelial carcinoma. In the JAVELIN Bladder 100 phase 3 trial, avelumab first-line maintenance + best supportive care significantly prolonged overall survival and progression free survival versus best supportive care alone in patients with advanced urothelial carcinoma without progression following first-line platinum-based chemotherapy.1
The JAVELIN Bladder Medley phase 2 trial is investigating the combination of avelumab with other antitumor agents in this patient population to assess efficacy and safety versus avelumab maintenance monotherapy. Sacituzumab govitecan is a Trop-2–directed antibody and topoisomerase inhibitor drug conjugate approved in various countries for specific populations of patients with previously treated advanced breast cancer. At the 2025 ASCO annual meeting, Dr. Hoffman-Censits reported an interim analysis of JAVELIN Bladder Medley assessing avelumab + sacituzumab govitecan versus avelumab monotherapy. Notably, this trial was initiated in August 2022, with the voluntary withdrawal of accelerated approve of sacituzumab govitecan for advanced urothelial carcinoma by the manufacturer in October 2024.
Eligible patients had unresectable locally advanced or metastatic urothelial carcinoma, ECOG performance status 0-1, and no disease progression after 4-6 cycles of first-line platinum-based chemotherapy. Patients were randomized 2:1 to avelumab + sacituzumab govitecan or avelumab monotherapy, stratified by presence of visceral metastases at start of first-line platinum-based chemotherapy. The trial design for JAVELIN Bladder Medley is as follows: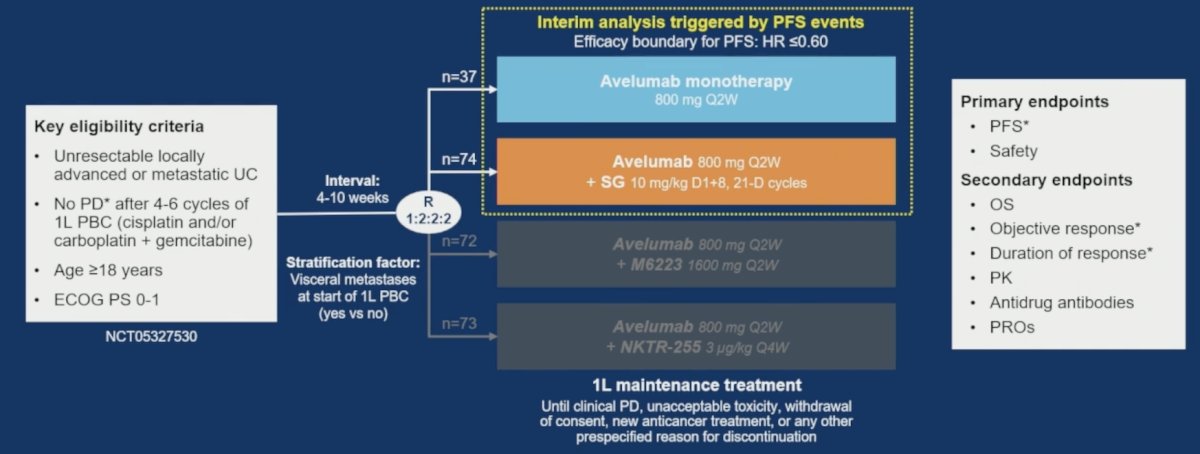
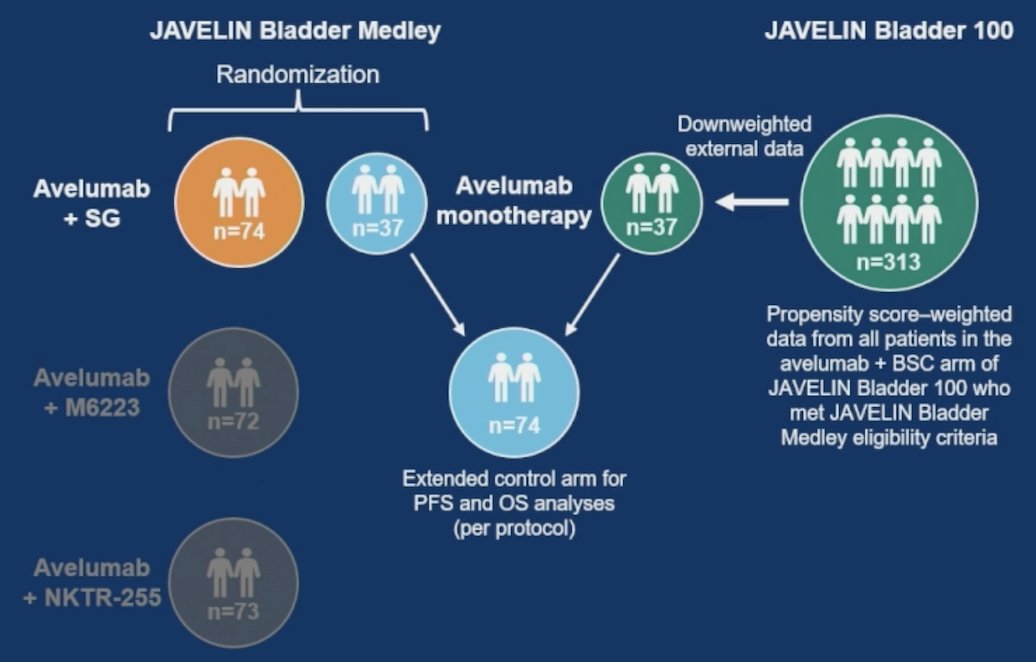
Primary endpoints were investigator-assessed progression free survival and safety, and overall survival was a secondary endpoint. Per protocol, progression free survival and overall survival data in the control arm were extended using external data form the JAVELIN Bladder 100 phase 3 trial. Patients who met JAVELIN Bladder Medley eligibility criteria were included (n = 313/350). To account for population differences, external patients were propensity-score weighted using predefined prognostic factors. The sum of external patients was down weighted to 37 to be equal to the number of randomized patients:
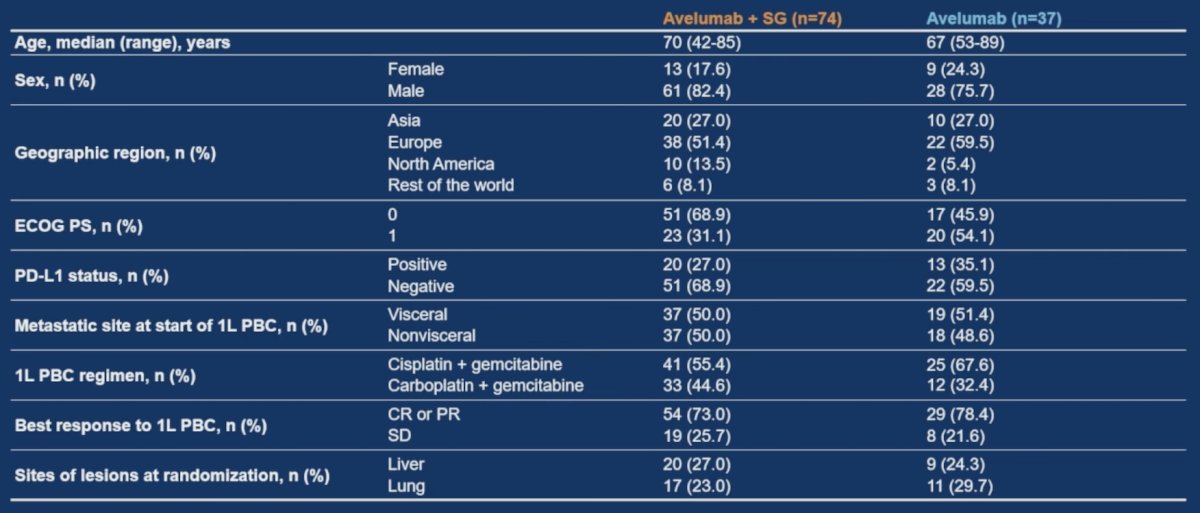
At the data cutoff of September 16, 2024, 38 of 74 patients (51.4%) in the avelumab + sacituzumab govitecan arm and 10 of 37 patients (27.0%) in the avelumab monotherapy arm were still receiving study treatment. In the avelumab + sacituzumab govitecan and avelumab monotherapy arms, respectively, the median age was 70 and 67 years, 50.0% and 51.4% had visceral metastases at start of first-line platinum-based chemotherapy, and a lower proportion of patients in the avelumab + sacituzumab govitecan arm had ECOG performance status of 1 (31.1% versus 54.1%):
The median progression free survival was 11.17 months (95% CI, 7.43-not estimable) with avelumab + sacituzumab govitecan versus 3.75 months (95% CI, 3.32-6.77) with avelumab monotherapy (HR 0.49, 95% CI, 0.31-0.76):

The investigator-assessed progression free survival subgroups generally showed a benefit for avelumab + sacituzumab govitecan: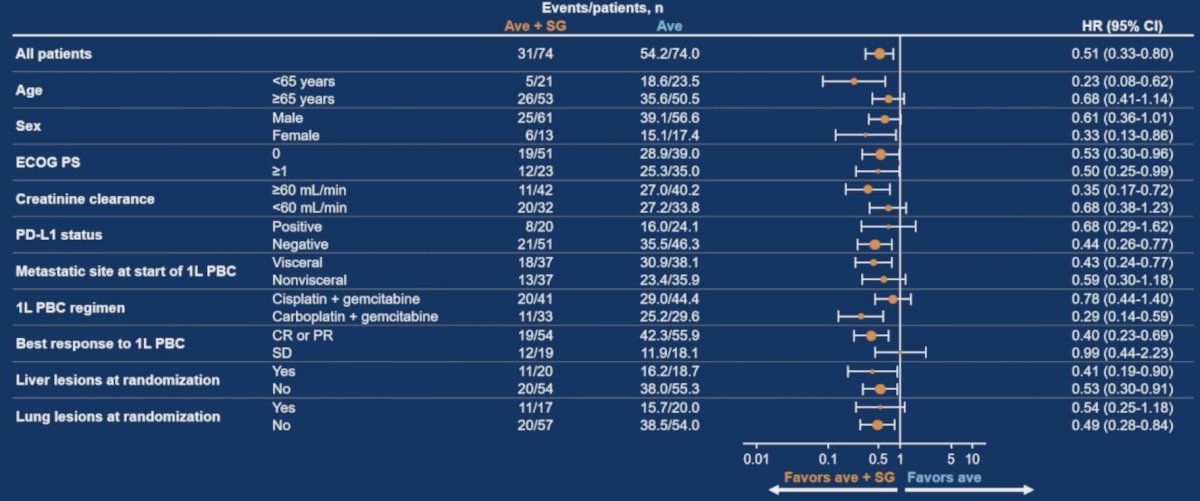
Overall survival data were immature at cutoff, with a median overall survival that was not reached (95% CI, 15.51-not estimable) in the avelumab + sacituzumab govitecan arm versus 23.75 months (95% CI, 18.79-30.82) in the avelumab monotherapy arm (HR 0.79, 95% CI, 0.42-1.50):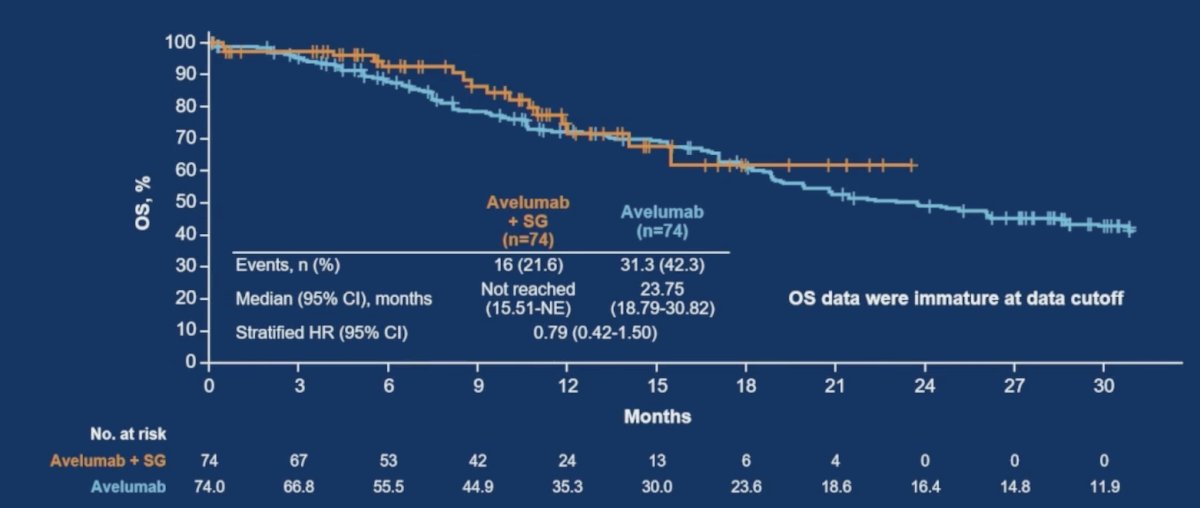
The objective response rate for avelumab + sacituzumab govitecan was 24.3% versus 2.7% in the avelumab monotherapy compared with baseline post first line platinum based chemotherapy. Additionally, the disease control rate was 68.9% versus 42.3% for avelumab + sacituzumab govitecan versus avelumab monotherapy: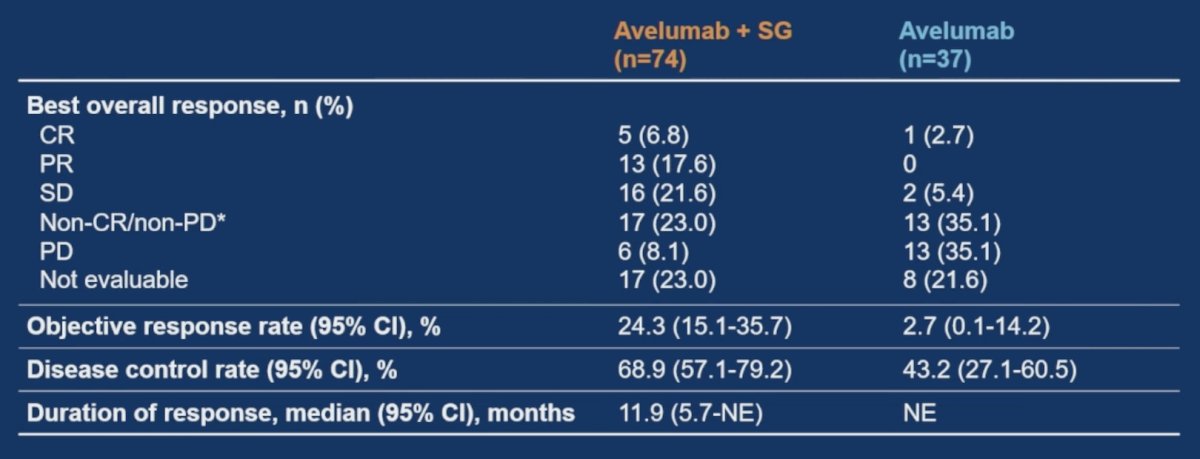
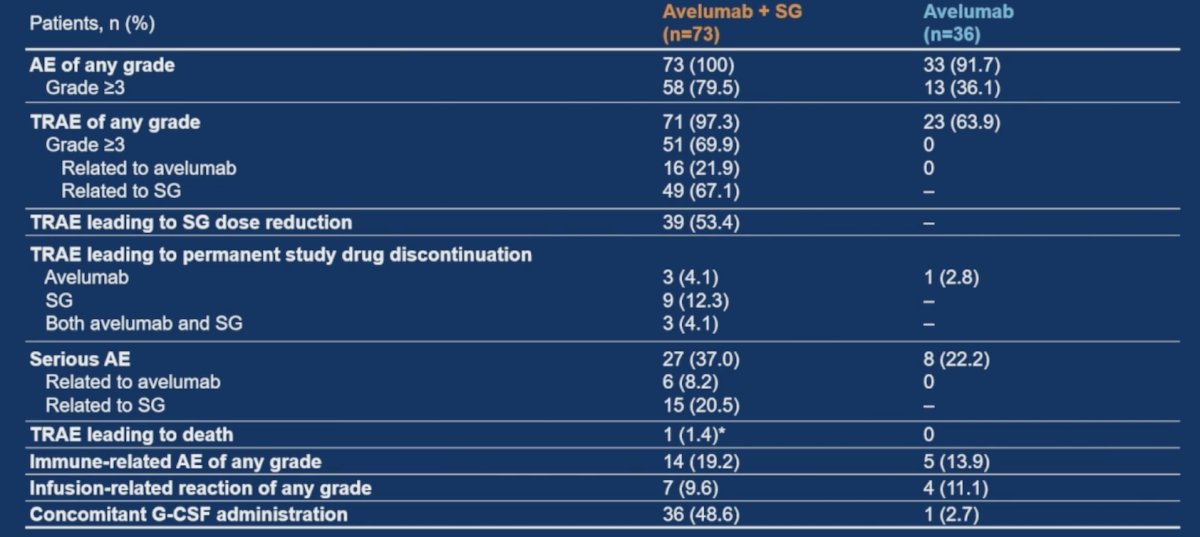
In the avelumab + sacituzumab govitecan and avelumab monotherapy arms, respectively, treatment-related adverse events of any grade occurred in 71 (97.3%) versus 23 patients (63.9%), and were grade ≥3 in 51 (69.9%) versus 0 patients. Treatment-related adverse events led to discontinuation of both avelumab + sacituzumab govitecan in 4.1% (sacituzumab govitecan only in 12.3%) versus avelumab monotherapy in 2.8%. One patient in the avelumab + sacituzumab govitecan arm had a sacituzumab govitecan-related adverse events that led to death (acute subarachnoid hemorrhage in the setting of sepsis and pancytopenia):
Dr. Hoffman-Censits concluded her presentation discussing an interim analysis from the JAVELIN Bladder Medley phase 2 trial with the following take-home points:
- In the interim analysis of the JAVELIN Bladder Medley randomized phase 2 trial of first line maintenance treatment in patients with advanced urothelial carcinoma without progression after first line platinum based chemotherapy:
- Progression free survival was improved with avelumab + sacituzumab govitecan versus avelumab monotherapy (stratified HR 0.49, 95% CI 0.31-0.76)
- Progression free survival was observed across various patient subgroups
- Overall survival data were immature at data cutoff and longer follow-up is required
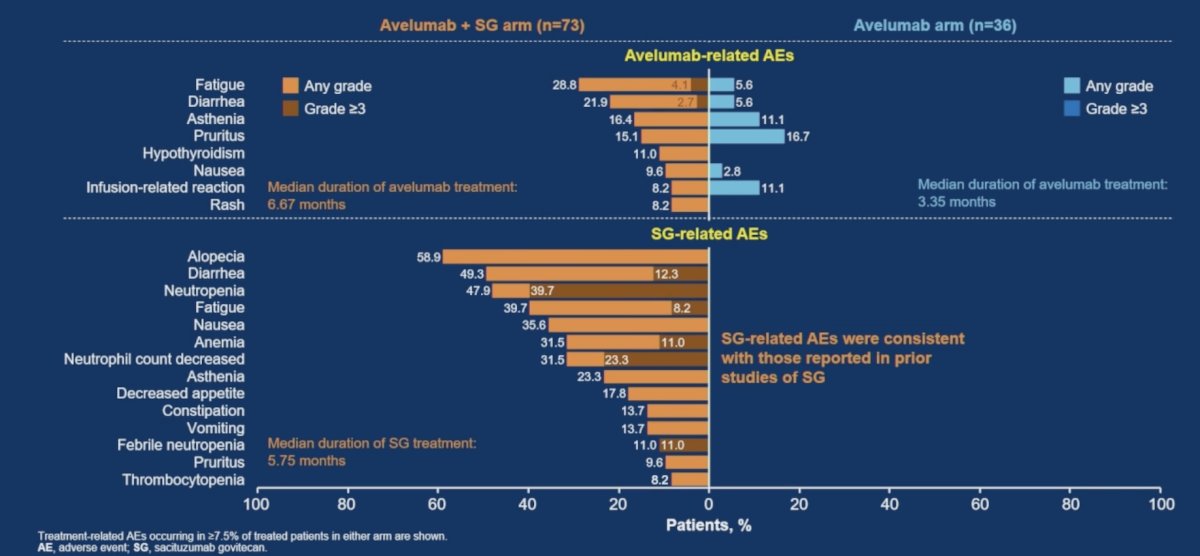
- Treatment related adverse events were more frequent in the combination arm and were consistent with the known safety profiles of avelumab + sacituzumab govitecan
- These findings suggest that combining avelumab with anti-Trop-2 antibody drug conjugates may be a promising strategy to improve patient outcomes in advanced urothelial carcinoma
Presented by: Jeannie Hoffman-Censits, MD, The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Johns Hopkins Greenberg Bladder Cancer Institute, Baltimore, MD
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: Medley Study Demonstrates Improved PFS of Avelumab-Sacituzumab in Maintenance Setting - Jean Hoffman-Censits
References:
- Powles T, Park SH, Voog E, et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N Engl J Med 2020 Sept 24;383(13):1218-1230.