

Patients received olaparib 300 mg twice a day notably without any ADT, until their prostate-specific antigen (PSA) doubled or they had evidence of metastatic disease. The primary endpoint was a confirmed PSA50. Of note, there was no biomarker-based pre-selection of patients but correlative studies were conducted including analysis of somatic DNA, RNA expression, and IHC for DNA damage markers. Baseline characteristics are shown below:
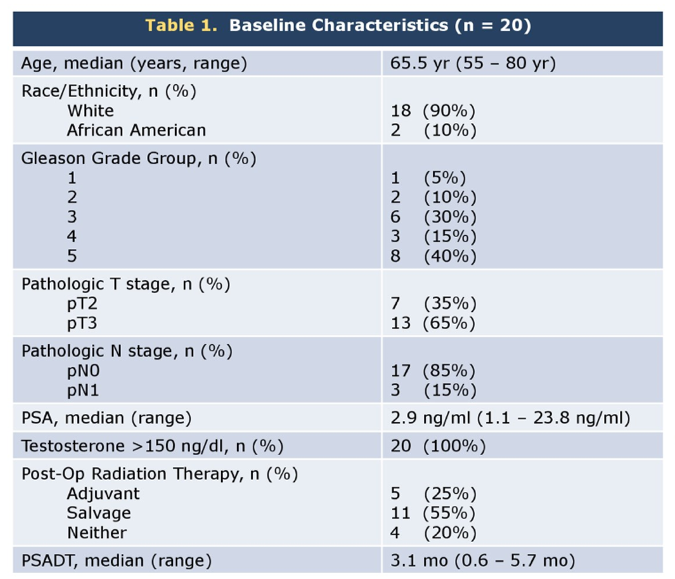
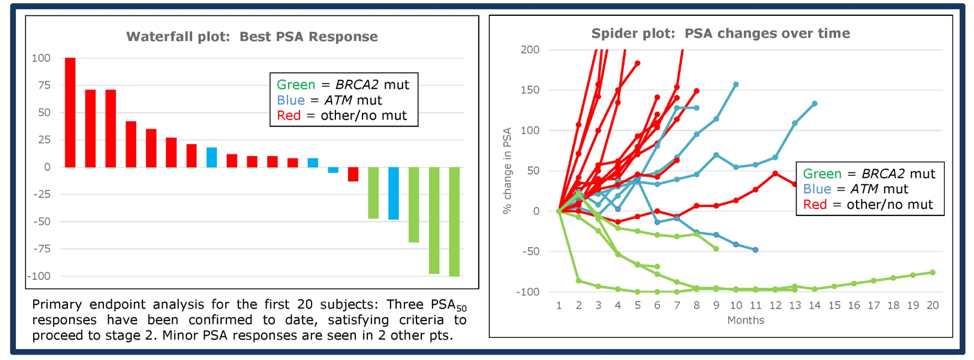
In this cohort of patients, the median PSADT was 3.1 months and 55% of patients had a Gleason of 8 or higher. 35% of men had a BRCA2 or ATM variant. Three men had a PSA50, all of whom had a BRCA2 mutation. Four other men had PSA declines. The median PSA PFS was greater in men with BRCA2/ATM mutations compared to those without.
The most common toxicities of olaparib included fatigue, nausea, anemia, and leukopenia and two patients required dose reductions due to toxicity.
Timing and duration of treatment of men with biochemically recurrent prostate cancer are controversial. Patients at high risk for metastatic progression includes the patients included in this study - those with high Gleason scores and those with low PSADTs. Currently, the standard of care includes either continuous or intermittent ADT.2 However, as this study shows, there may be a subset of patients (those with DNA damage repair defects) who may respond to PARP inhibition. However, this appears to trade the toxicity of ADT (hot flashes, fatigue, loss of libido) for the toxicities of PARP inhibition (myelosuppression). Of note, one rare side effect of PARP inhibition is treatment-related AML and this factor should be considered if patients are to be placed on continuous PARP inhibition for biochemically recurrent prostate cancer.3
Presented by: Emmanuel S. Antonarakis, MD, Associate Professor of Oncology, Johns Hopkins Medicine, Baltimore, MD
Written by: Jason Zhu, MD. Fellow, Division of Hematology and Oncology, Duke University, @TheRealJasonZhu at the 2019 ASCO Annual Meeting #ASCO19, May 31- June 4, 2019, Chicago, IL USA
References:
- Antonarakis ES, Feng Z, Trock BJ, et al. The natural history of metastatic progression in men with prostate‐specific antigen recurrence after radical prostatectomy: long‐term follow‐up. BJU international 2012;109:32-9.
- Crook JM, O'callaghan CJ, Duncan G, et al. Intermittent androgen suppression for rising PSA level after radiotherapy. New England Journal of Medicine 2012;367:895-903.
- Zhu J, Tucker M, Wang E, et al. Acute Myeloid Leukemia After Olaparib Treatment in Metastatic Castration-Resistant Prostate Cancer. Clinical genitourinary cancer 2017;15:e1137-e41.