(UroToday.com) Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 held in Lugano, Switzerland was host to a session addressing the contemporary management of metastatic prostate cancer. Dr. Natacha Naoun discussed what imaging should be used in case of suspected metastases.
Why do we do conventional imaging? The objective has been to obtain important baseline staging information and combine that with relevant clinical information to reach the best treatment decision.
The treatment landscape for prostate cancer has significantly evolved over the past few decades. Previously, a dichotomous approach had been adopted, whereby patients with M+ disease on conventional imaging have been recommended for ADT, whereas those with M- disease were recommended for local therapy.

However, the prostate cancer landscape has evolved with the emergence of:
- New drugs: Androgen receptor pathway inhibitors (ARPIs), radioligand therapies, PARP inhibitors
- New techniques: PSMA PET, molecular testing
- New definitions of disease burden
And now, there are new challenges that require enhanced imaging:
Dr. Naoun noted that there are two distinct clinical pictures:
- De novo metastatic castrate-sensitive prostate cancer (mCSPC)
- Metachronous (i.e., recurrent) mCSPC
In the de novo mCSPC setting, intensified treatment with ADT + an ARPI +/-docetaxel is required for these patients, as per numerous international guidelines.

These recommendations are further tailored based on the burden of metastatic disease on conventional imaging, with prostate radiotherapy an option for CHAARTED low disease burden patients, based on the STAMPEDE Arm H data:1

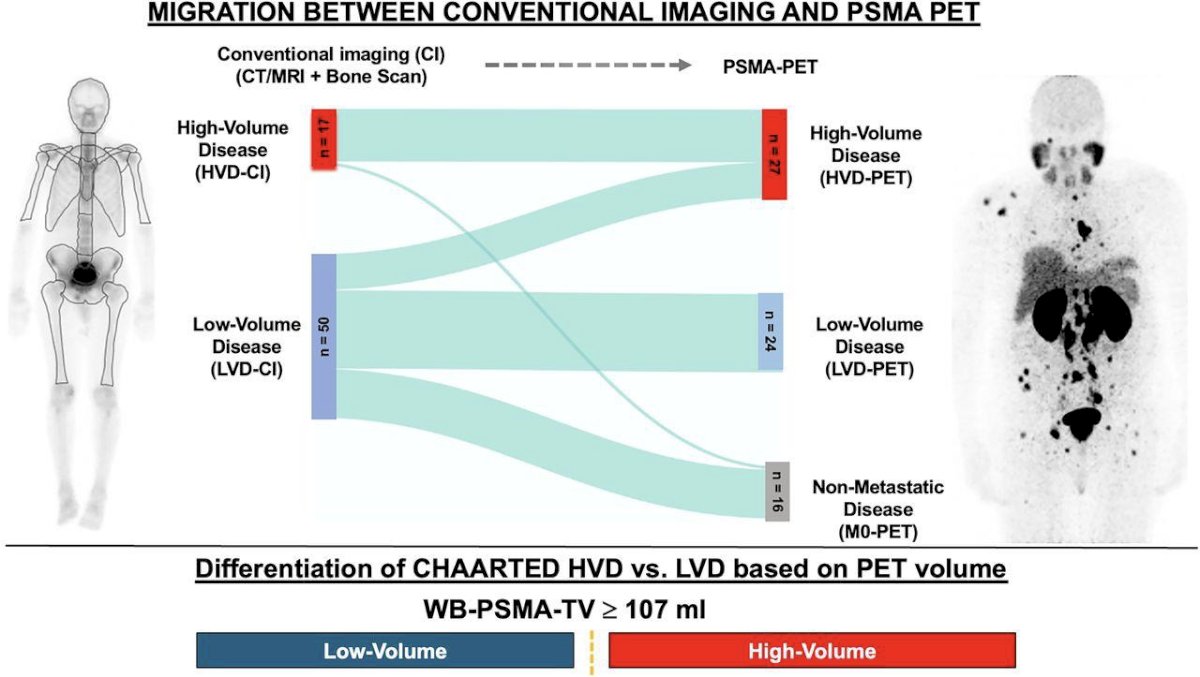
How do the results of conventional imaging translate to PSMA PET in patients with de novo mCSPC? In a 2025 study published in The Journal of Nuclear Medicine, Unterrainer et al. demonstrated that all patients with high-volume disease on conventional imaging were similarly found to have high volume disease on PET. Conversely, 20% of patients with conventional imaging-defined low volume disease had PET high volume disease, and 30% had non-metastatic disease (i.e., M0-PET).2
Dr. Naoun next discussed data from the PEACE-1 trial to highlight the importance of accurate staging in de novo mCSPC patients. The PEACE-1 trial employed a 2x2 design to assess, (separately and combined) the impact of adding abiraterone acetate + prednisone (AAP) and radiation therapy to standard of care therapy in men with de novo mCSPC. The control arm in this study evolved to reflect the contemporary standard of care. When the study began enrolling patients, the standard of care for first-line mCSPSC was ADT alone. With the publication of data from the STAMEDE and CHAARTED, standard of care was updated to include ADT plus docetaxel 75 mg/m2 every 3 weeks for 6 cycles. The two experimental treatments investigated in this study were:
1) AAP until disease progression or intolerance (concomitant to docetaxel)
2) RT of the prostate (74 Gy in 37 fractions after completion of docetaxel).

PEACE-1 was designed with two co-primary endpoints for the AAP analysis: (i) rPFS and (ii) OS. There were 1,173 patients randomized to standard of care alone (n=296), standard of care plus radiation therapy (n=293), standard of care plus AAP (n=292), and standard of care plus radiation therapy and AAP (n=291). Median follow-up was 3.5 years (IQR 2.8–4.6) for rPFS and 4.4 years (3.5–5.4) for OS. Adjusted Cox regression modeling revealed no interaction between abiraterone and radiotherapy, enabling the pooled analysis of these last two groups to assess abiraterone efficacy.
The addition of AAP to standard of care in the overall population resulted in a 46% improvement in rPFS (HR 0.54, 99.9% CI 0.41 to 0.71) and a 50% improvement in the ADT with docetaxel population (HR 0.50, 99.9% CI 0.34 to 0.71):

Similar results were observed for OS. In the overall study population (including both patients receiving radiation therapy and not receiving radiation therapy), the addition of AAP resulted in an 18% improvement in OS with median OS of 4.7 years on the standard of care arm and 5.7 years on the standard of care plus AAP arm (HR 0.82, 95.1% CI 0.69 to 0.98):3

In the updated analysis presented by Dr. Bossi a ASCO 2023 and since published in The Lancet,4 demonstrated that the addition of radiotherapy to standard of care therapy +/- abiraterone in the low-volume cohort was associated with significant improvements in the time to serious genitourinary events (p=0.0006). This overall benefit was consistent irrespective of whether patients had prostate radiotherapy added to standard of care + abiraterone (p=0.003) or standard of care alone (p=0.048).

What about the treatment paradigm of oligorecurrent metastatic disease? In this disease space, there are two notable trials that have evaluated metastasis-directed therapy: STOPMP and ORIOLE.4,5

The STOMP trial was a multicenter, randomized phase II trial that prospectively evaluated the effects of MDT for patients with evidence of oligometastatic disease on choline PET/CT (up to three extracranial sites) who had received prior treatment with curative intent and had evidence of biochemical recurrence with testosterone >50 ng/ml (i.e. metachronous, oligometastatic mCSPC). Between 2012 and 2015, 62 patients were randomized 1:1 and MDT was either SBRT or metastasectomy. The primary endpoint was time to initiation of ADT (called ADT-free survival). ADT was initiated for symptoms, progression beyond three metastases, or local progression of known metastatic disease. Time to castration resistance was a secondary endpoint (called CRPC-free survival). With a median follow up of 5.3 years, the five-year ADT-free survival was 8% in the surveillance arm compared to 34% for the MDT group (HR: 0.57, 95% CI: 0.38-0.84, log-rank p=0.06). No differences were seen between groups when stratified by nodal versus non-nodal metastases. Secondary endpoint of CRPC-free survival at 5 years was 53% in subjects under surveillance and 76% in those receiving MDT (HR: 0.62, 80% CI: 0.35-1.09.4
The ORIOLE trial was a randomized phase II trial of 54 men with metachronous, oligometastatic mCSPC (up to three sites). Metastatic sites were diagnosed via conventional imaging (CT, MRI, and/or radionuclide bone scan). Between 2016 and 2018, patients were randomized in a 2:1 fashion to receive SABR or observation. The primary outcome was progression at 6 months, defined as serum PSA increase, progression detected by conventional imaging, symptomatic progression, ADT initiation for any reason, or death. Progression at six months occurred in 7 of 36 patients (19%) receiving SABR and 11 of 18 patients (61%) undergoing observation (p=0.005). Treatment with SABR improved median PFS (not reached versus 5.8 months; HR: 0.30; 95% CI: 0.11 – 0.81; p=0.002). No grade ≥3 toxic effects were observed.5
What do the experts recommend in the oligorecurrent metastatic setting? When queried at the 2024 APCCC regarding the management of patients with metachronous, low-burden mCSPC on conventional imaging, 88% noted that they would treat patients using the conventional imaging findings only if no relevant additional and/or untreatable lesions were confirmed by next-generation imaging.

For patients with metachronous, low-burden mCSPC on next-generation imaging and negative conventional imaging findings, 69% voted that they would recommend systemic therapy plus metastasis-directed therapy.

For patients with metachronous low burden mCSPC on conventional imaging being recommended for systemic therapy, 51% responded that they would recommend lifelong treatment with ADT +/- an ARPI or an ARPI alone, with 32% recommending a similar approach for 2-3 years, as opposed to lifelong treatment.

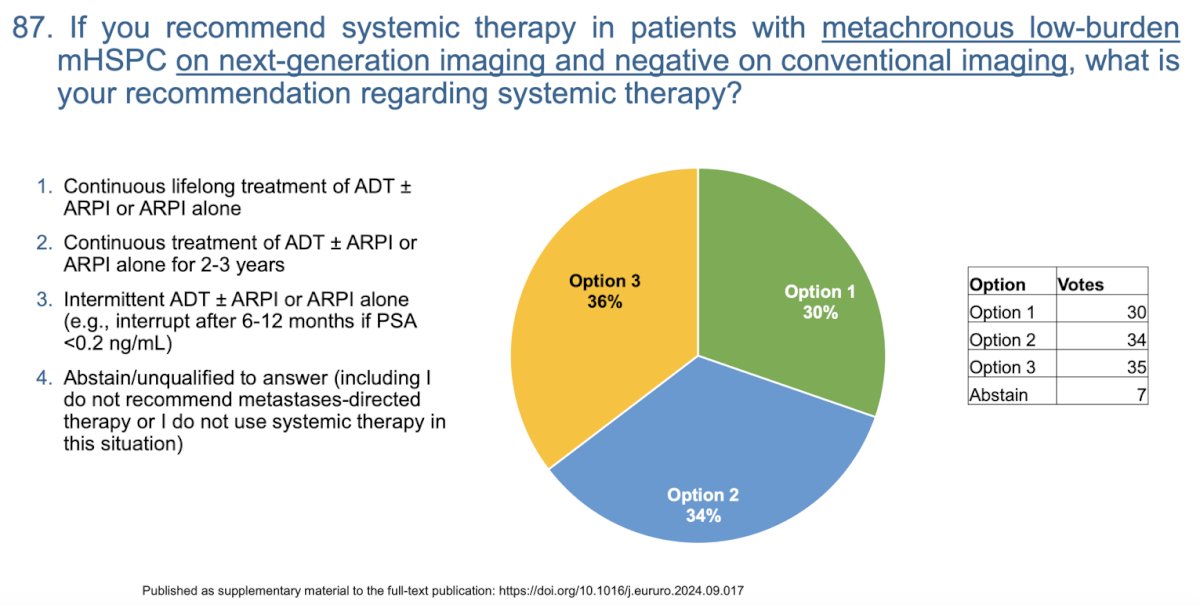
For metachronous low burden mCSPC patients on next generation imaging and negative conventional imaging being recommended for systemic therapy, the experts were split on whether to recommend:
- Continuous life-long treatment with ADT +/- an ARPI or an APRI alone (30%)
- Continuous treatment with ADT +/- an ARPI or an APRI alone for 2-3 years (34%)
- Intermittent ADT +/- an ARPI or an ARPI alone, with interruption at 6-12 months if PSA levels are undetectable (36%)
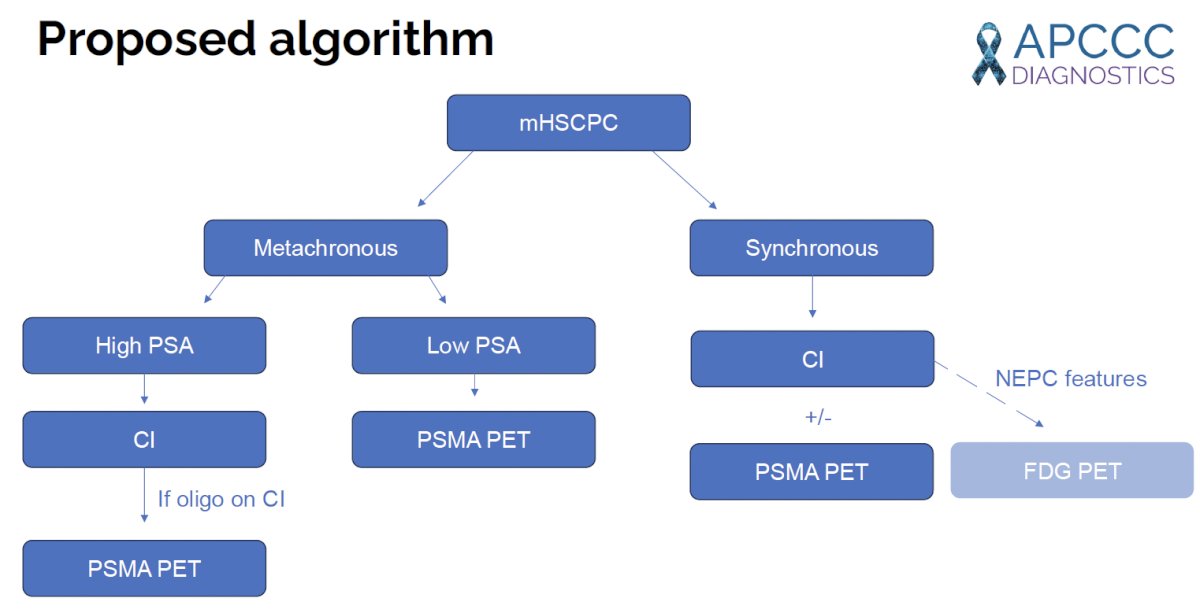
Based on the current evidence, Dr. Naoun concluded with her proposed algorithm for imaging mHSPC patients, based on disease timing and PSA levels:
Presented by: Natacha Naoun, MD, MSc, Medical Oncology Department, Gustave Roussy Cancer Campus, 94805 Villejuif, France.
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.
References:
- Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): A randomized controlled phase 3 trial. Lancet. 2018; 392(10162): 2353-66.
- Unterrainer LM, Hope TA, Fendler WP, et al. Low- and High-Volume Disease in Metastatic Hormone-Sensitive Prostate Cancer: From CHAARTED to PSMA PET-An International Multicenter Retrospective Study. J Nucl Med. 2025; 66(1):54-60.
- Fizazi K, Foulon S, Carles J, Roubaud G, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomized, phase 3 study with a 2 x 2 factorial design. Lancet. 2022; 399(10336): 1695-1707.
- Ost P, Reynders D, Decaestecker K, et al. Surveillance of metastasis-directed therapy for oligometastatic cancer recurrence: A prospective, randomized, multicenter phase II trial. J Clin Oncol. 201; 36(5):446-453.
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol. 2020; 6(5) :650-659.