(UroToday.com) Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 held in Lugano, Switzerland was host to a session addressing the contemporary management of metastatic prostate cancer. Dr. Michael Hofman discussed how we can translate the findings of next-generation imaging to conventional imaging for treatment decision-making.

What are the ABCs of next-generation imaging?
- Abandon the obsolete imaging approaches
- Be aware of the capabilities and limits of next-generation imaging
- Consider next-generation imaging whenever patient management is to be modified
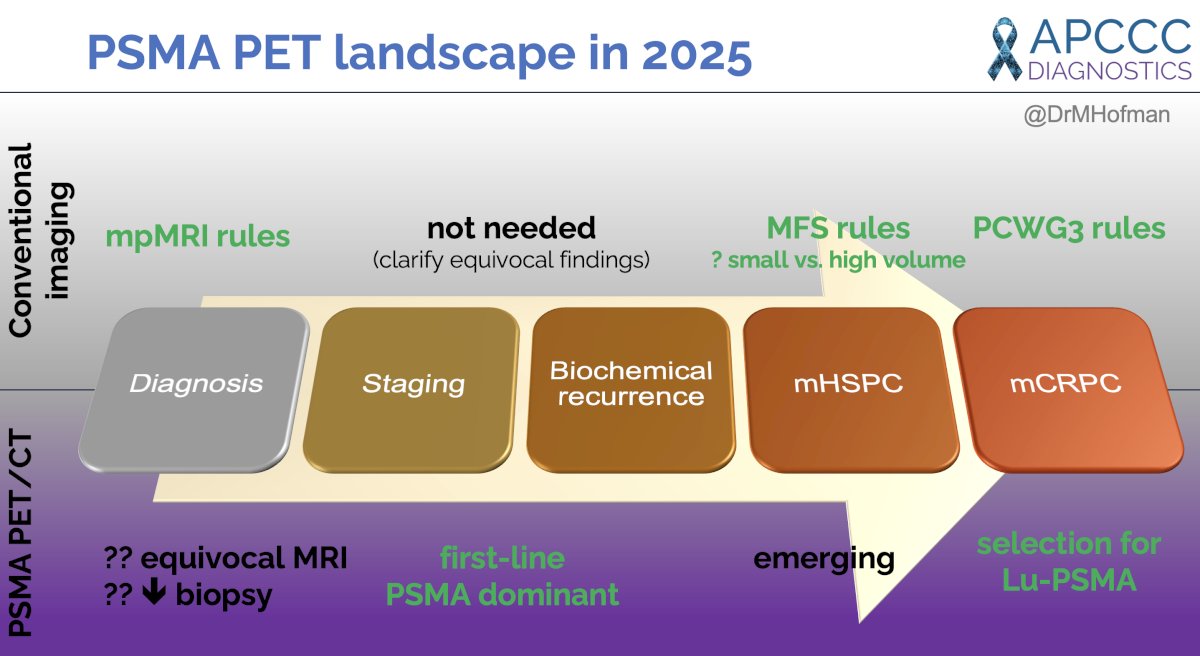
What is the current landscape of PSMA PET in 2025? Conventional imaging currently ‘rules’ in the diagnosis (mpMRI), metastatic hormone-sensitive, and castrate-resistant setting (CT abdomen/pelvis + bone scan).
PSMA/PET may be used in the diagnosis setting in cases of equivocal MRI results and may decrease the frequency of biopsies required in select patients.1 It is currently ‘dominant’ for staging intermediate and high-risk patients, an emerging tool for staging metastatic hormone-sensitive patients, and a critical tool for selecting eligible mCRPC patients for Lu-PSMA therapy.
As such, is PSMA PET imaging a ‘biomarker’ or an extension of the ‘physical examination’? Either way – ‘The PSMA train has left the station’.
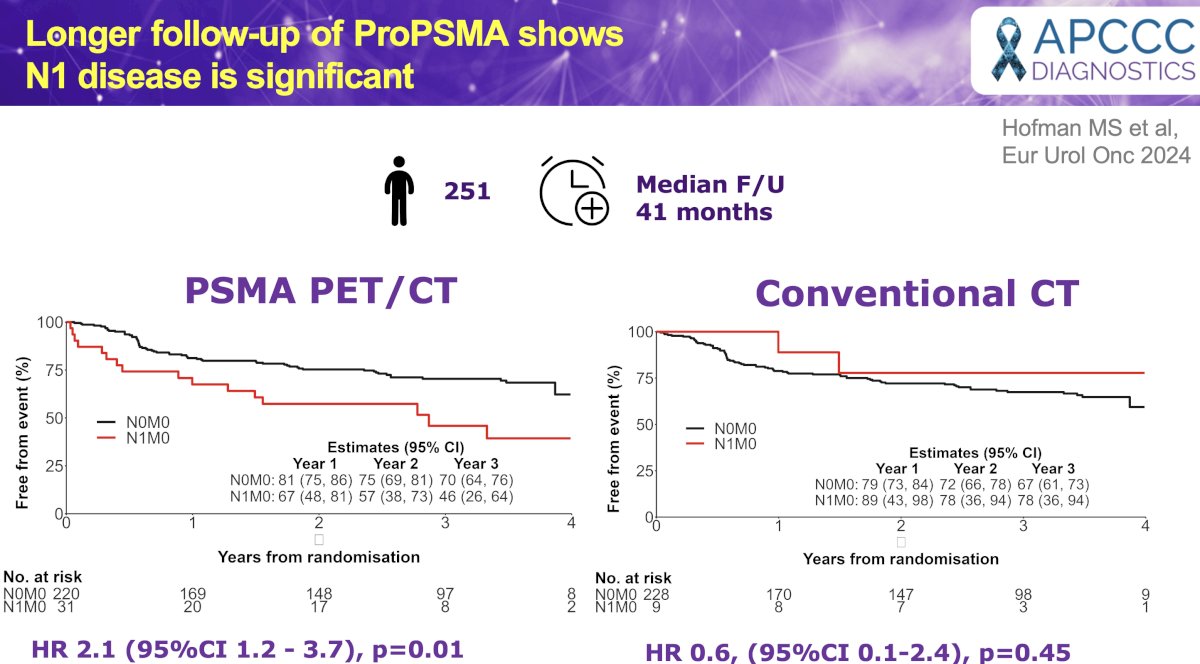
He emphasized his belief that the findings on PSMA PET add valuable clinical information and do not represent a simple stage migration phenomenon. This is highlighted by a recently published long-term follow-up of the ProPSMA trial that shows that patients with PSMA PET-detected N1 disease have significantly worse event-free survival rates, compared to those with PSMA PET-defined N0M0 disease (HR: 2.1, p=0.01). Conversely, there were no significant differences in event-free survival rates between conventional imaging-defined cN1M0 and cN0M0 patients (HR: 0.60, p=0.05).1 Thus, it is clear that this additional information provided by PSMA PET is critical for providing accurate staging information of prognostic significance.
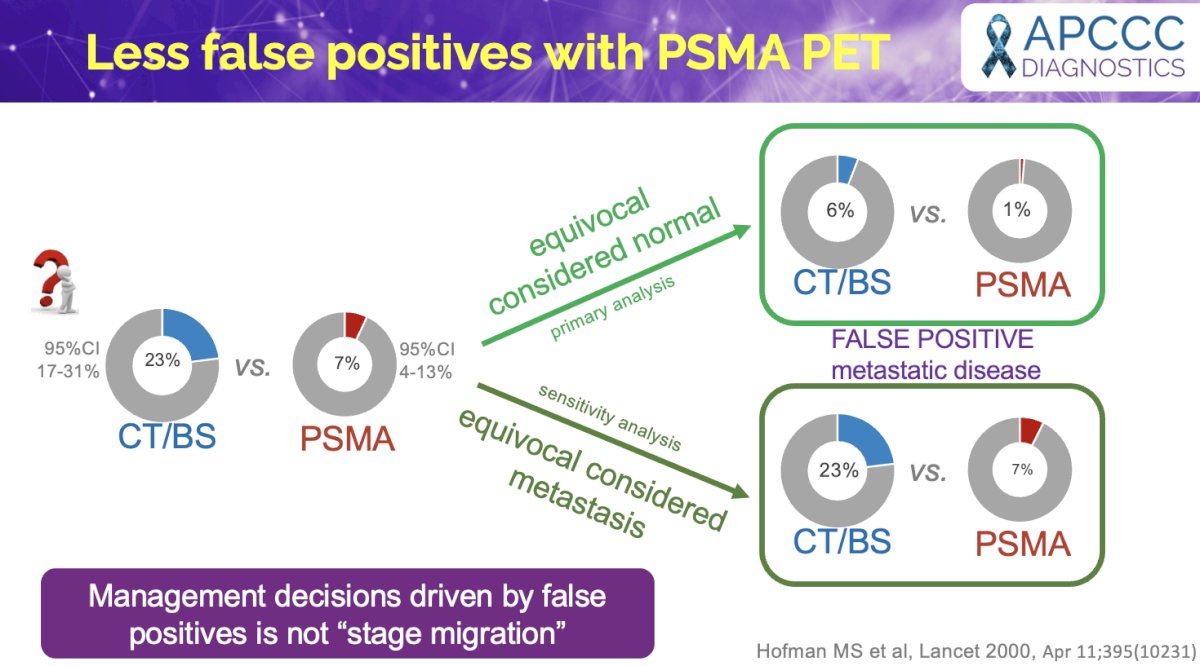
In addition to its enhanced sensitivity, an important advantage of PSMA PET imaging is the lower incidence of false positives (i.e., improved specificity), compared to conventional imaging. Dr. Hofman highlighted a case example of a proPSMA trial participant who had evidence of bone and liver metastases on conventional imaging, but on PSMA PET/CT, had no evidence of regional or distant metastases.

In the proPSMA trial, more equivocal findings for identifying any metastatic disease were seen with conventional imaging, compared with PSMA PET-CT (23% versus 7%, p<0.001).3
But could these false positive findings commonly seen on conventional imaging (CT/bone scan) explain the results of some important trials in the advanced prostate cancer space? In STAMPEDE Arm H, pelvic radiotherapy improved overall survival outcomes in patients with conventional imaging-defined CHAARTED low metastatic burden (HR: 0.68, p<0.05), but not those with a CHAARTED high disease burden.4
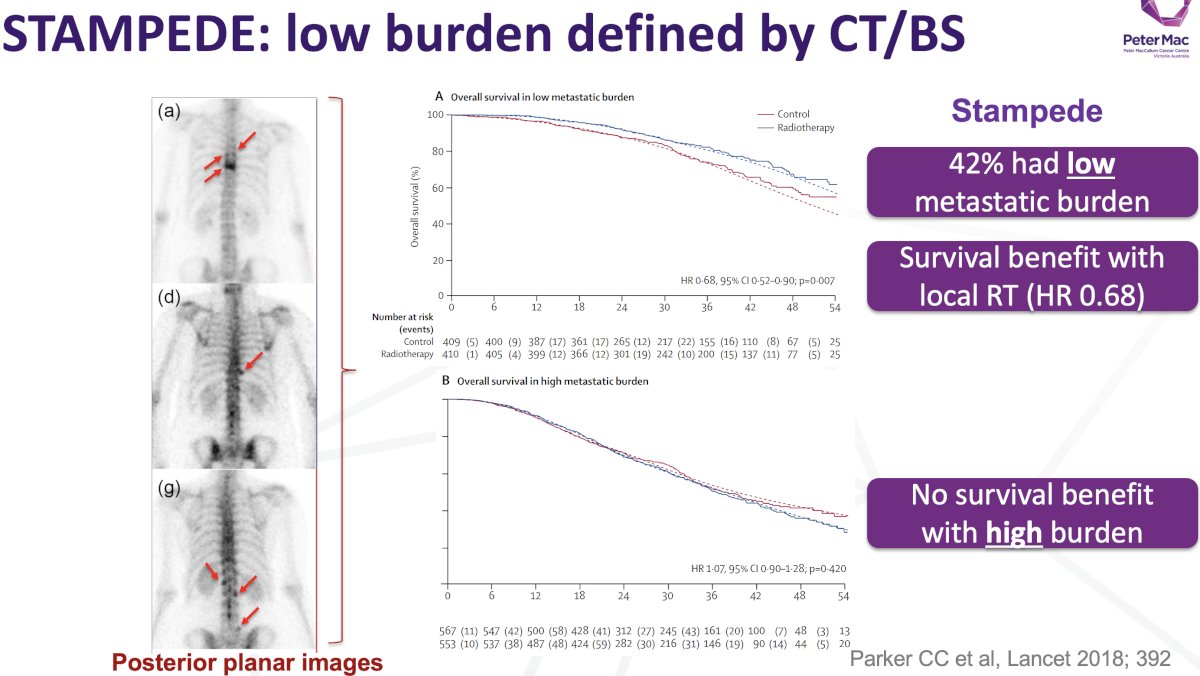
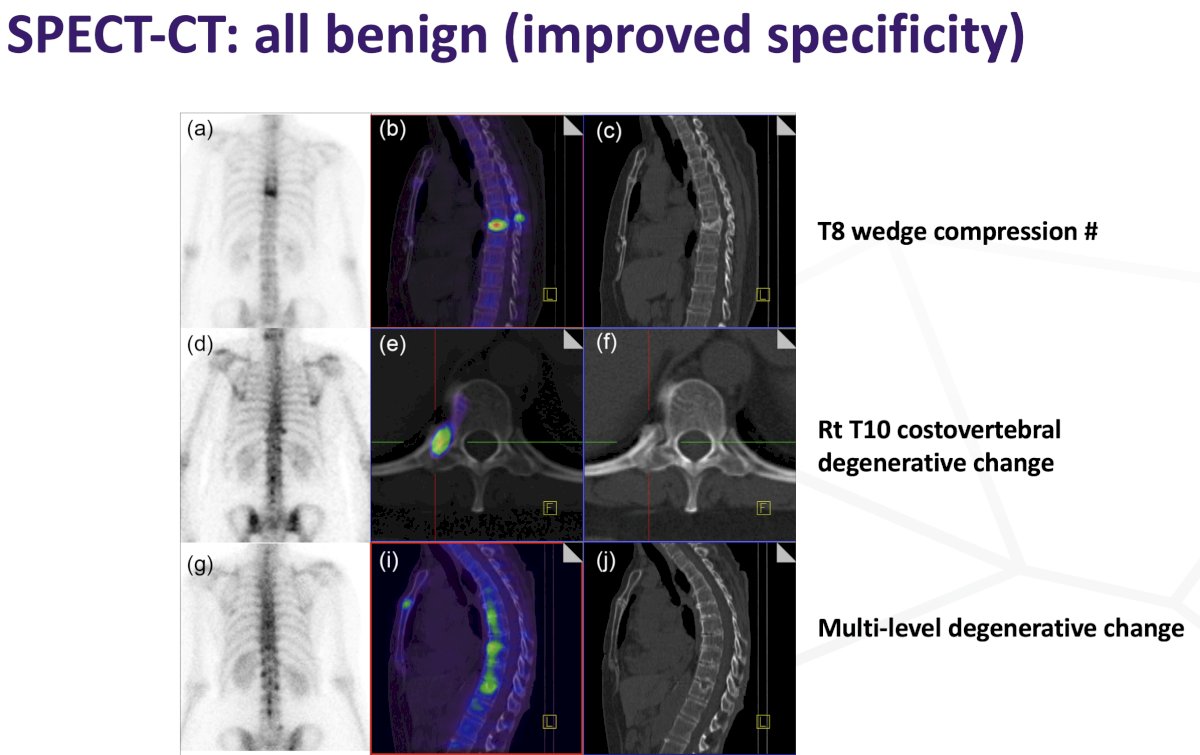
Dr. Hofman emphasized once again that many of these positive findings on conventional imaging may actually represent false positives. He highlighted three examples of commonly seen false positives on SPECT-CT commonly mistaken for bone metastases:
- Spinal wedge compression fractures
- Costovertebral degenerative changes
- Multi-level degenerative changes
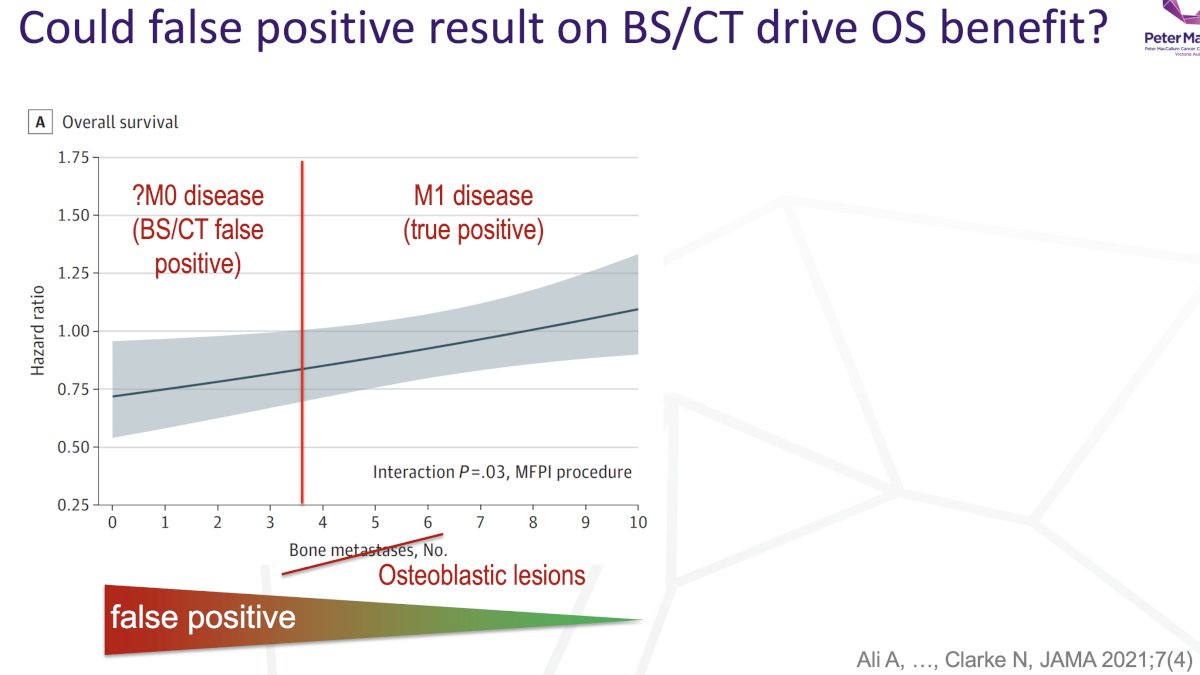
Thus, with this in mind, could a number of patients in the STAMPEDE low metastatic burden cohort have actually had localized, non-metastatic disease, with the treatment benefit observed with pelvic radiotherapy in this subgroup just actually representing the benefits of pelvic radiotherapy in patients with prostatic fossa-limited disease? Ad hoc analysis from STAMPEDE Arm H identified that the benefit of pelvic radiotherapy decreased as the number of osteoblastic lesions increased past 3-4 bone metastases.5 Does this simply reflect a higher likelihood of false positives in patients with a lesser number of osteoblastic lesions, compared to those with a higher burden of conventional imaging-defined bone metastases?
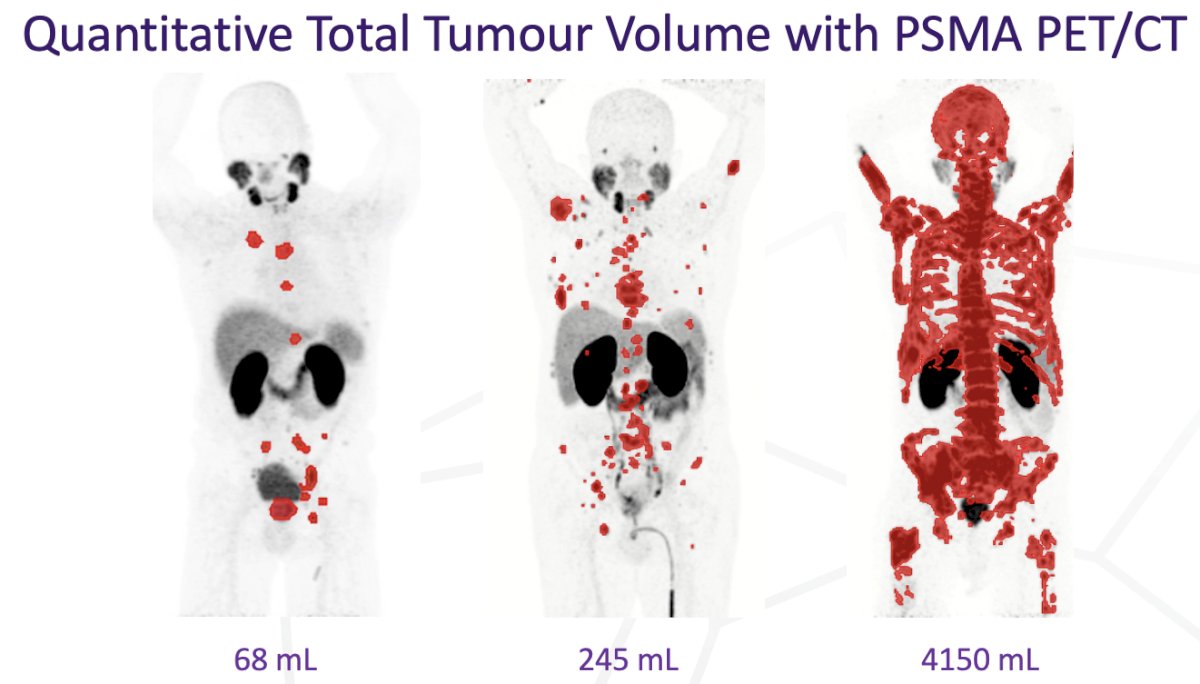
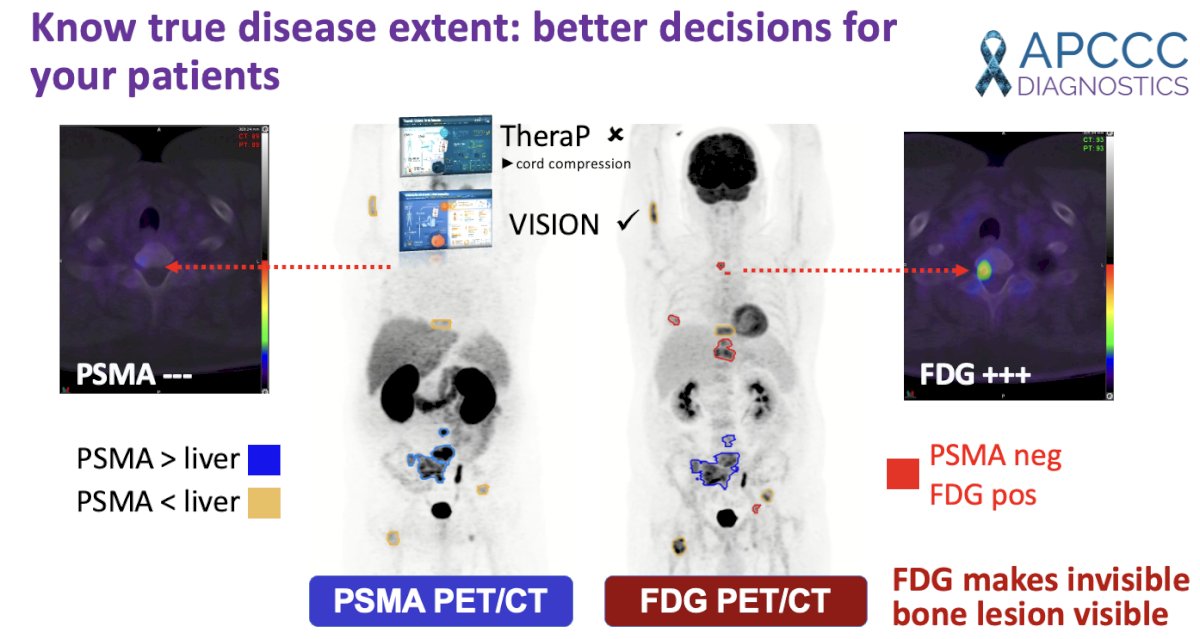
An additional advantage of PSMA PET imaging is the ability to visually quantify tumor volume:
When different next-generation imaging modalities are combined, the diagnostic yield can be further improved:
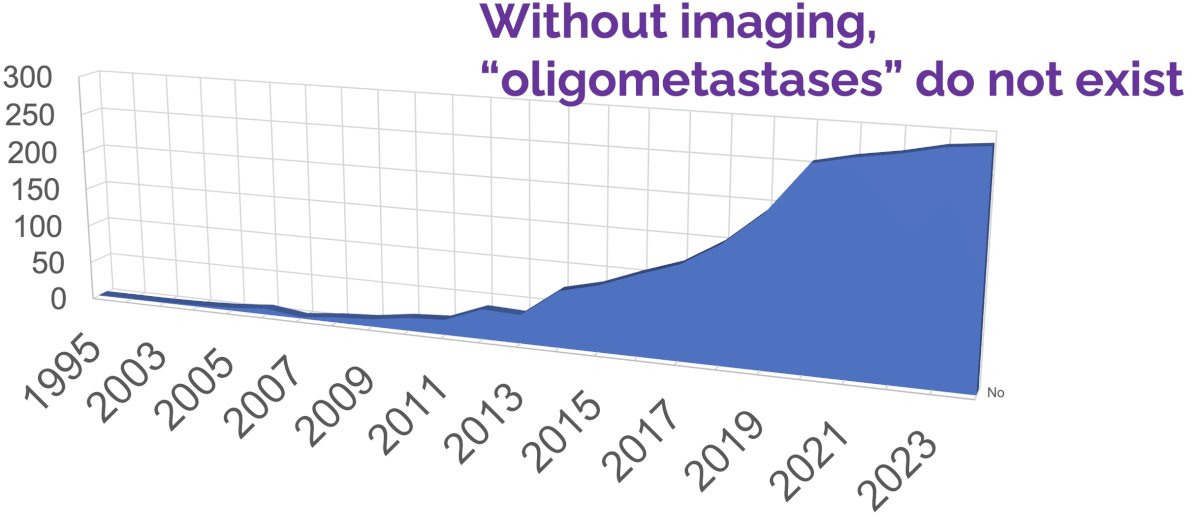
The increased uptake of next-generation imaging has also been directly related to the emergence of the prominent oligometastatic disease state.
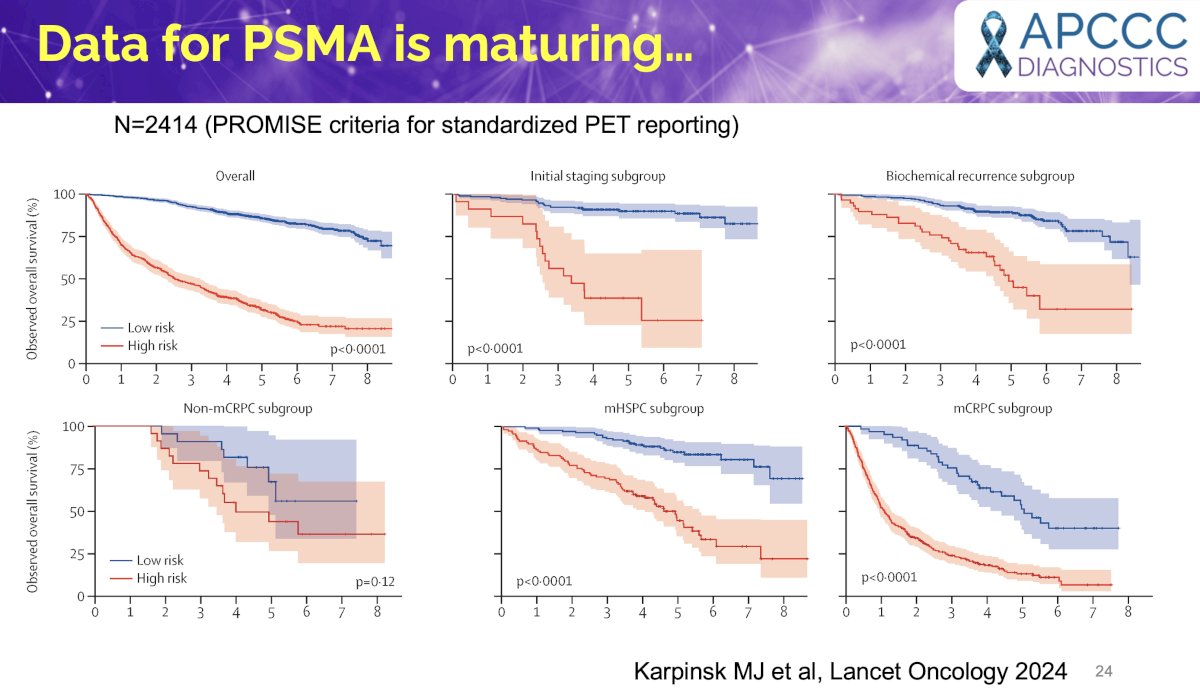
Importantly, our ability to interpret PSMA PET findings is maturing. The Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE) criteria were proposed to standardise PSMA-PET reporting. Karpinski et al. compared the prognostic value of PSMA-PET by PROMISE stage with established clinical nomograms in a large prostate cancer dataset with follow-up data for overall survival. They demonstrated that these PSMA-PET by PROMISE stage nomograms accurately stratify high-risk and low-risk groups for overall survival in early and late stages of prostate cancer and yield equal or superior prediction accuracy compared with established clinical risk tools.6
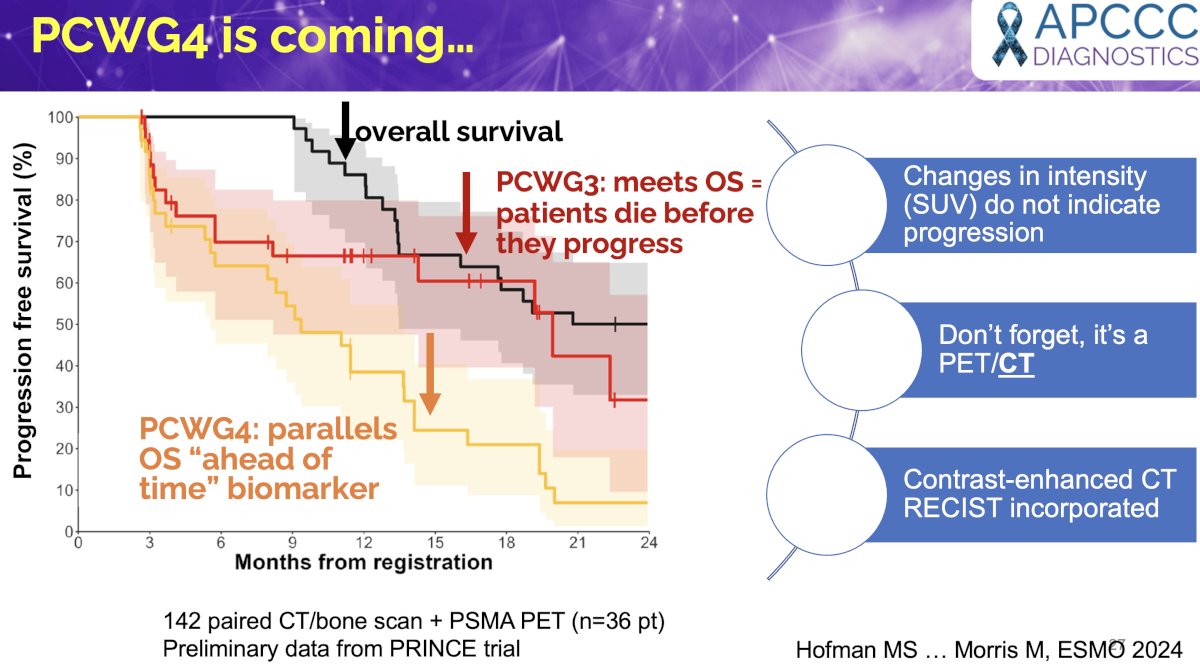
Dr. Hofman cautioned however that PSMA PET is not a validated endpoint for clinical trials, but that the Prostate Cancer Working Group 4 (PCWG4) criteria are soon coming and will incorporate PSMA PET/CT findings.

Dr. Hofman concluded his presentation as follows:
- PSMA PET findings are more real than conventional imaging:
- PSMA PET has superior sensitivity and specificity compared to conventional imaging
- Conventional imaging has higher “false positive” findings
- These do not improve outcomes
- Like a physical exam, imaging directs individual patient management
- Do not treat blindly
- Biomarker data are emerging but conventional imaging-defined metastasis-free survival and PCWG3 still rule.
- Let’s collect more data together…
Presented by: Michael Hofman, MBBS, FRACP, FAANMS, FICIS, GAICD, Prostate Cancer Theranostics and Imaging Centre of Excellence, Peter MacCallum Cancer Center, Melbourne, Australia
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.
References:
- Emmett L, Papa N, Buteau J, et al. The PRIMARY Score: Using Intraprostatic 68Ga-PSMA PET/CT Patterns to Optimize Prostate Cancer Diagnosis. J Nucl Med. 2022; 63(11): 1644-50.
- Hofman MS, Kasivisvanathan V, Link E, et al. Baseline Nodal Status on 68Ga-PSMA-11 Positron Emission Tomography/Computed Tomography in Men with Intermediate- to High-risk Prostate Cancer Is Prognostic for Treatment Failure: Follow-up of the proPSMA Trial. Eur Urol Oncol. 2024: S2588-9311(24)00251-7.
- Hofman MS, Lawrentschuk N, Francis, RJ, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomized, multicentre study. Lancet. 2020; 395(10231): 1208-1216.
- Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): A randomized controlled phase 3 trial. Lancet. 2018; 392(10162) :2353-2366.
- Ali A, Hoyle A, Haran AM, et al. Association of Bone Metastatic Burden with Survival Benefit from Prostate Radiotherapy in Patients with Newly Diagnosed Metastatic Prostate Cancer: A Secondary Analysis of a Randomized Clinical Trial. JAMA Onc. 2021; 7(4): 555-563.
- Karpinski MJ, Husing J, Claassen K, et al. Combining PSMA-PET and PROMISE to re-define disease stage and risk in patients with prostate cancer: a multicentre retrospective study. Lancet Oncol. 2024; 25(9): 1188-1201.