(UroToday.com) The 2025 APCCC Diagnostics annual meeting featured a session on what we should know for PSMA radioligand therapy and a presentation by Dr. Andrei Gafita discussing prognostic, predictive and response biomarkers for PSMA radioligand therapy.
With regards to the PSMAfore randomized trial,1 Dr. de Bono at ASCO 2024 presented results of the baseline ctDNA analysis and associations with outcomes in taxane-naïve patients with mCRPC treated with 177Lu-PSMA-617 versus change in androgen receptor pathway inhibitor. This analysis noted that 177Lu-PSMA-617 prolonged radiographic progression-free survival compared with androgen receptor pathway inhibitor change, regardless of baseline ctDNA fraction:

Additionally, higher baseline ctDNA fraction was associated with shorter radiographic progression-free survival regardless of treatment received:
Also at ASCO 2024, Kwon and colleagues presented results of ctDNA fraction as a predictor of treatment efficacy in the TheraP phase 2 trial of 177Lu-PSMA-617 versus cabazitaxel. The odds of a PSA50 response to 177Lu-PSMA-617 versus cabazitaxel were significantly higher for men with ctDNA <2% (p = 0.0067), with no significant difference at ctDNA >30% (OR 1.1, 95% CI 0.42 - 2.8). The PSA50 and PSA90 response stratified by ctDNA% categories are depicted below:
ctDNA <2% was also associated with a significant improvement when treated with 177Lu-PSMA-617 compared with cabazitaxel, with an 8.7 month increase in the median progression free survival (HR 0.12, 95% CI 0.04-0.38), which was confirmed on multivariable analysis adjusting for PSMA SUVmean and other clinical prognostic factors (HR 0.35, 95% CI 0.13-0.93; interaction p = 0.035):
Post-hoc work from the TheraP trial has assessed PSMA and FDG-PET as predictive and prognostic biomarkers in patients given 177Lu-PSMA-617 versus cabazitaxel for mCRPC.2 There were 35 (35%) of 99 men who were assigned 177Lu-PSMA-617, and 30 (30%) of 101 men who were assigned cabazitaxel that had high PSMA uptake (SUVmean of ≥10). The odds of PSA response to 177Lu-PSMA-617 versus cabazitaxel were significantly higher for men with SUVmean of 10 or higher compared with those with SUVmean of less than 10 (OR 12.19, 95% CI 3.42-58.76 versus OR 2.22, 95% CI 1.11-4.51; padj = 0.039 for treatment-by-SUVmean interaction). Among the SUVmean >= 10 patients, 177Lu-PSMA-617 had significantly improved PSA progression free survival compared to cabazitaxel (HR 0.45, 95% CI 0.25-0.80), which was not the case for SUVmean <10 (HR 0.77, 95% CI 0.53-1.12).
In work published in early 2024 in Lancet Oncology, Hofman and colleagues3 noted that after a median follow-up of 35.7 months (IQR 31.1 to 39.2) in TheraP, 77 (78%) participants had died in the 177Lu-PSMA-617 group and 70 (69%) participants had died in the cabazitaxel group. Overall survival was similar among those assigned to 177Lu-PSMA-617 versus those assigned to cabazitaxel (restricted mean survival time 19.1 months vs 19.6; difference -0.5 months; p = 0.77). Additionally, in this subsequent analysis, PSMA PET and FDG PET were both prognostic for overall survival (top row: PSMA PET; bottom row: FDG PET):

In 2021, Gafita and colleagues3 published in Lancet Oncology a nomogram of baseline characteristics for prediction of overall survival following 177Lu-PSMA-617. Among 270 patients, predictors included in the nomograms were time since initial diagnosis of prostate cancer, chemotherapy status, baseline hemoglobin, and 68Ga-PSMA-11 PET/CT parameters (molecular imaging TNM classification and tumour burden). The C-index of the overall survival model was 0.71 (95% CI 0.69-0.73):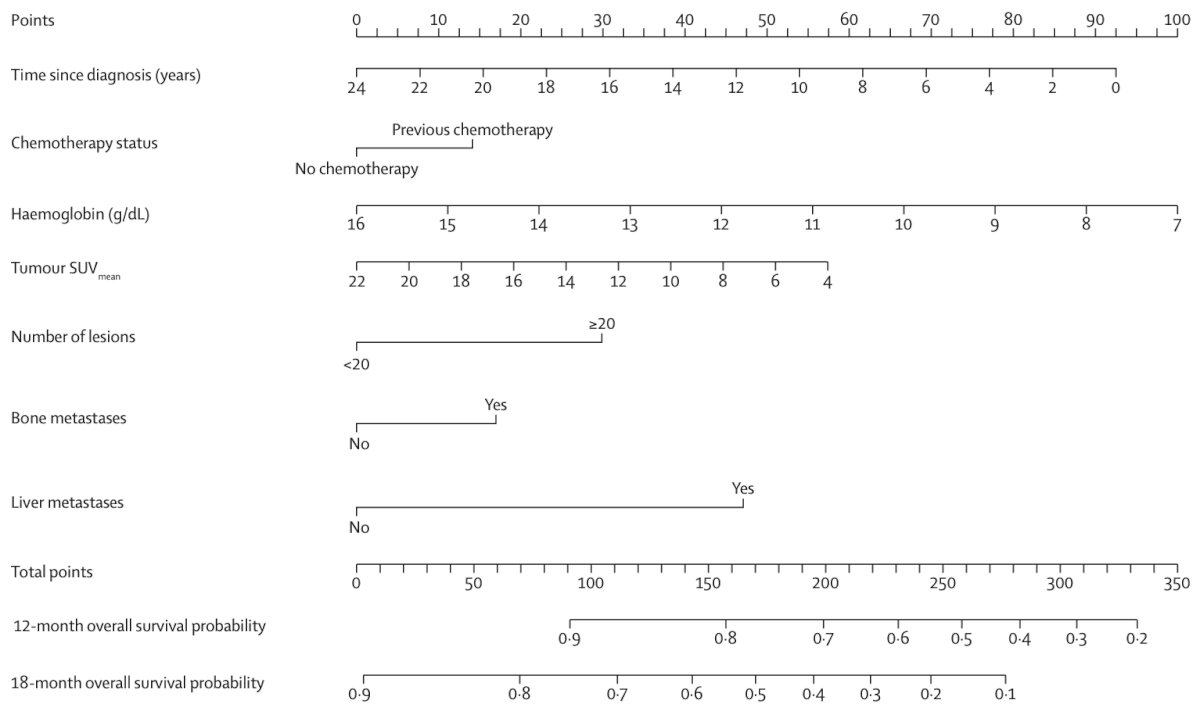
This was similar to the C-index of the PSA-progression-free survival model (0.70, 95% CI 0.68-0.72). Compared with high-risk patients, low-risk patients had significantly longer overall survival in the validation cohort (24.9 months versus 7.4 months; p < 0.0001):
PSA-progression-free survival (6.6 months versus 2.5 months; p = 0.022). Dr. Gafita’s group have also recently published TheraP validation of prognostic and predictive models for therapeutic response.5 In this analysis, the probability of PSA50 in patients classified as having a favorable outcome was greater in the 177Lu-PSMA-617 group than in the cabazitaxel group (OR 6.36, 95% CI 1.69-30.80 versus 0.96, 95% CI 0.32-3.05). Additionally, the PSA50 rate in patients with a favorable outcome for 177Lu-PSMA-617 versus cabazitaxel was 62/88 (70%) versus 31/85 (36%). The decision curve analysis indicated that the use of the PSA50 model had a clinical net benefit when the probability of a PSA response was ≥30%.
In 2024, Herrmann and colleagues6 reported the first multivariable models of outcomes with 177Lu-PSMA-617 built using data from VISION. The overall survival nomogram (C-index, 0.73; 95% CI, 0.70-0.76) included whole-body SUVmax, time since diagnosis, opioid analgesic use, aspartate aminotransferase, hemoglobin, lymphocyte count, presence of PSMA-positive lesions in lymph nodes, lactate dehydrogenase, alkaline phosphatase, and neutrophil count. Additionally, the radiographic progression free survival nomogram had a C-index of 0.68 and the PS50 nomogram an AUC of 0.72:
To explore the association between quantitative baseline 68Ga-PSMA-11 PET/CT parameters and treatment response and outcomes in the VISION trial, Kuo et al. found that whole-body tumor SUVmean was the best predictor of 177Lu-PSMA-617 efficacy, with a HR range of 0.86-1.43 for all outcomes (all p < .001) .7 A 1-unit whole-body tumor SUVmean increase was associated with a 12% and 10% decrease in risk of a radiographic progression free survival event and death, respectively. Higher baseline PSMA-positive tumor volume and tumor load were associated with worse radiographic progression free survival (HR range, 1.44-1.53 [p < 0.05] and 1.02-1.03 [p < 0.001], respectively) and overall survival (HR range, 1.36-2.12 [p < 0.006] and 1.04 [p < 0.001], respectively):![To explore the association between quantitative baseline 68Ga-PSMA-11 PET/CT parameters and treatment response and outcomes in the VISION trial, Kuo et al. found that whole-body tumor SUVmean was the best predictor of 177Lu-PSMA-617 efficacy, with a HR range of 0.86-1.43 for all outcomes (all p < .001) .7 A 1-unit whole-body tumor SUVmean increase was associated with a 12% and 10% decrease in risk of a radiographic progression free survival event and death, respectively. Higher baseline PSMA-positive tumor volume and tumor load were associated with worse radiographic progression free survival (HR range, 1.44-1.53 [p < 0.05] and 1.02-1.03 [p < 0.001], respectively) and overall survival (HR range, 1.36-2.12 [p < 0.006] and 1.04 [p < 0.001], respectively)](/images/com-doc-importer/194-apccc-diagnostics-2025/apccc-diagnostics-2025-prognostic-predictive-and-response-biomarkers-during-psma-rlt/image-8.jpg)
Finally, Dr. Gafita discussed his groups initial experience with 177Lu-PSMA-617 after regulatory approval for mCRPC.8 Baseline PSMA PET/CT images were analyzed using SelectPSMA, an artificial intelligence algorithm, to predict treatment outcome. Among 76 patients, the median PSA progression free survival was 4.1 months (95% CI, 2.0-6.2 months), and the median overall survival was 13.7 months (95% CI, 11.3-16.1 months). There were 25% of patients classified by SelectPSMA as non-responders that had significantly lower rates of PSA response than patients classified as likely responders (6% vs. 51%; P < 0.001), a shorter PSA progression free survival (median, 1.3 versus 6.3 months; p < 0.001), and a shorter overall (median, 6.3 versus 14.5 months; p = 0.046).
The following highlights the adapted PCWG3 and RECIP 1.0 algorithm:
Dr. Gafita concluded his presentation discussing prognostic, predictive and response biomarkers for PSMA radioligand therapy with the following take-home points:
- Baseline ctDNA fraction is a prognostic biomarker for radiographic progression free survival and may be a predictive biomarker for radiographic progression free survival after PSMA radioligand therapy versus taxanes
- 177Lu-PSMA-617 nomograms and tumor SUVmean are prognostic but not predictive biomarkers for survival outcome after PSMA radioligand therapy versus best standard of care/cabazitaxel
- FDG PET is a prognostic but not predictive biomarker, however it’s added value in patient selection has yet to be proven
- Artificial intelligence technology SelectPSMA may shape future selection of patients for PSMA radioligand therapy if proven to be a predictive biomarker for overall survival
- RECIP 1.0 is an evidence based response biomarker during PSMA radioligand therapy and clinical implementation is ongoing
Presented by: Andrei Gafita, MD, Department of Radiology and Radiological Sciences, Johns Hopkins Thernostics Center, Baltimore, MD
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.
References:
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.
- Buteau JP, Martin AJ, Emmett L, et al. PSMA and FDG-PET as predictive and prognostic biomarkers in patients given [177Lu]Lu-PSMA-617 versus cabazitaxel for metastatic castration-resistant prostate cancer (TheraP): A biomarker analysis from a randomized, open-label, phase 2 trial. Lancet Oncol. 2022 Nov;23(11):1389-1397.
- Hofman MS, Emmett L, Sandhu S, et al. Overall survival with [177Lu]Lu-PSMA-617 versus cabazitaxel in metastatic castration-resistant prostate cancer (TheraP): Secondary outcomes of a randomized, open-label, phase 2 trial. Lancet Oncol. 2024 Jan;25(1):99-107.
- Gafita A, Calais J, Grogan TR, et al. Nomograms to predict outcomes after 177Lu-PSMA therapy in men with metastatic castration-resistant prostate cancer: An international, multi-centre, retrospective study. Lancet Oncol. 2021 Aug;22(8):1115-1125.
- Gafita A, Martin AJ, Emmett L, et al. Validation of prognostic and predictive models for therapeutic response in patients treated with [177Lu]Lu-PSMA-617 versus Cabazitaxel for metastatic castration-resistant prostate cancer (TheraP): A post-hoc analysis from a randomized, open-label, phase 2 trial. Eur Urol Oncol. 2025 Feb;8(1):21-28.
- Herrmann K, Gafita A, de Bono JS, et al. Multivariable models of outcomes with [177Lu]Lu-PSMA-617: Analysis of the phase 3 VISION trial. EClinicalMedicine. 2024 Oct 4:77:102862.
- Kuo PH, Morris MJ, Hesterman J, et al. Quantitative 68Ga-PSMA-11 PET and Clinical Outcomes in Metastatic Castration-resistant prostate cancer following 177Lu-PSMA-617 (VISION Trial). Radiology. 2024 Aug;312(2):e233460.
- Gafita A, Voter A, Shesadri S, et al. Initial experience with [177Lu]Lu-PSMA-617 after regulatory approval for metastatic castration-resistant prostate cancer: Efficacy, safety, and outcome prediction. J Nucl Med. 2024 Nov 1;65(11):1724-1730.