(UroToday.com) The 2025 APCCC Diagnostics annual meeting featured a session on what we should know for PSMA radioligand therapy and a presentation by Dr. Joe O'Sullivan discussing what we should have reported in an MRI and PSMA PET. Dr. O’Sullivan started his presentation by noting several assumptions when discussing what we want to have reported, such as (i) that we are talking about patients being considered for PSMA targeted radioligand therapy (2nd or 3rd line mCRPC), (ii) we are talking about whole body MRI, and (iii) we are in a routine clinic as opposed to a research setting.
However, before the what we want reported comes the why, which is to acquire information about the cancer in order to help make decisions. This is particularly important given how many therapy options there currently are: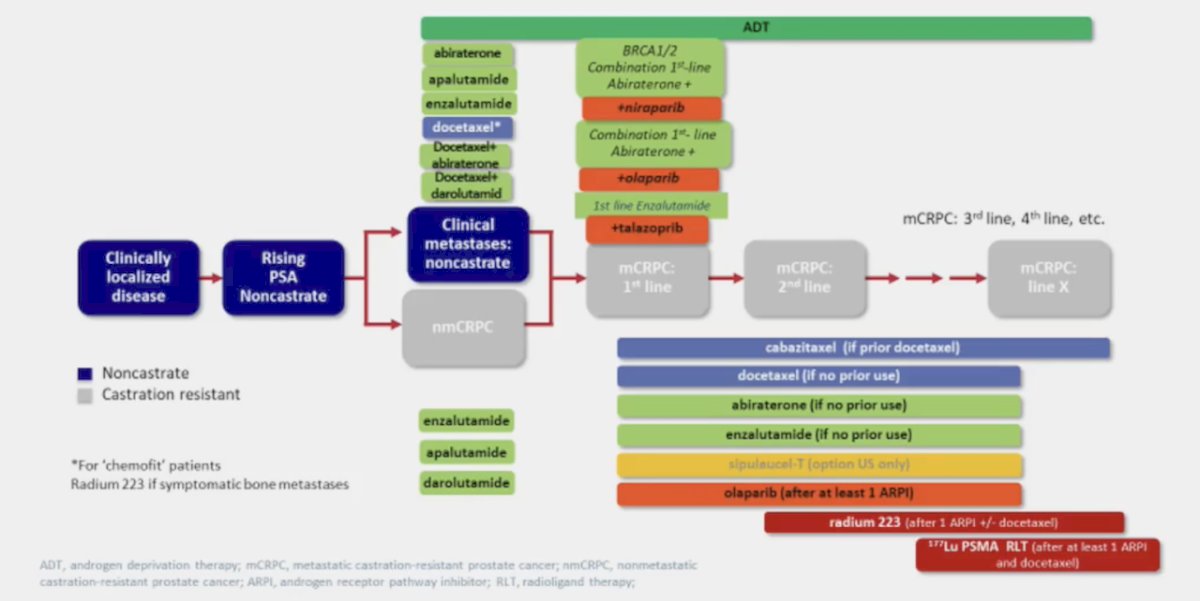
Notably, there is limited window, since patients are at the 2nd or 3rd line stage of mCRPC and are heavily pretreated, with a median overall survival of ~12 months, and many being symptomatic from their phase of illness. Dr. O’Sullivan emphasized that what you want to have reported in an MRI and PSMA PET depends on who you are, namely the patient or the clinician. Information needed by the patient includes:
- Am I dying?
- How long do I have to live?
- Is my treatment working?
- What other treatments are available?
- What is the best treatment right now?
- Can I reduce and/or avoid treatment? Especially castration and cytotoxic chemotherapy
- Why is my PSA rising?
- Why do I have pain?
Information needed by clinicians is similar, but in a different context:
- Estimated prognosis
- Response assessment
- Is the patient suitable for radioligand therapy?
- Is oligometastatic disease amenable to stereotactic ablative radiotherapy?
- Why is his PSA rising?
- What is the location of the metastases?
- What is the aggressiveness of the metastases?
- Are there signs/risk of cord compression?
With regards to the information, Dr. O’Sullivan started by discussing prognosis: (i) sites of metastasis - both whole body MRI and PSMA PET are adequate, with PSMA PET slightly better, (ii) extent of metastasis - both whole body MRI and PSMA PET are adequate, with PSMA PET slightly better, (iii) rate of progression - both whole body MRI and PSMA PET are adequate, with PSMA PET slightly better and iv) potential issues ahead (ie. cord impingement) - both whole body MRI and PSMA PET are adequate, with whole body MRI slightly better: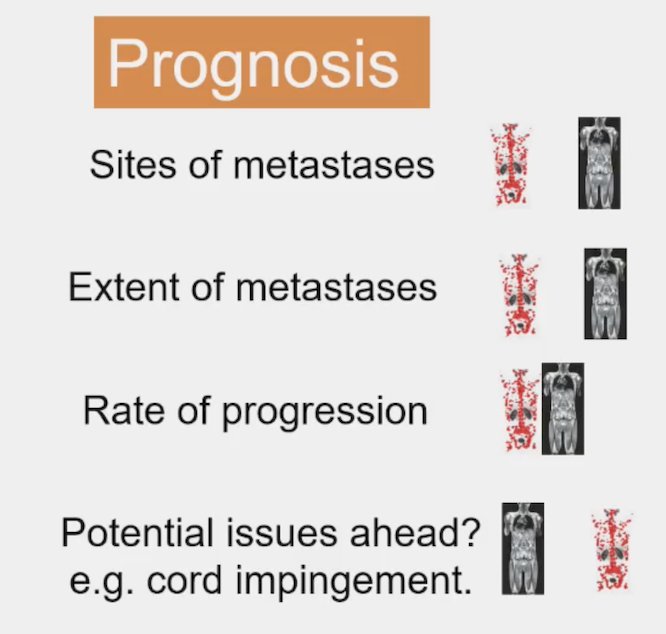
For selecting the choice of treatment: (i) is PSMA-targeted radioligand therapy an option? PSMA PET is clearly better; (ii) are there metastases without PSMA uptake? Both whole body MRI and PSMA PET are adequate, with whole body MRI slightly better, (iii) extent of metastases - both whole body MRI and PSMA PET are adequate, with PSMA PET slightly better, (iv) what is the likelihood of a response (compared to an alternative therapy)? PSMA PET is clearly better: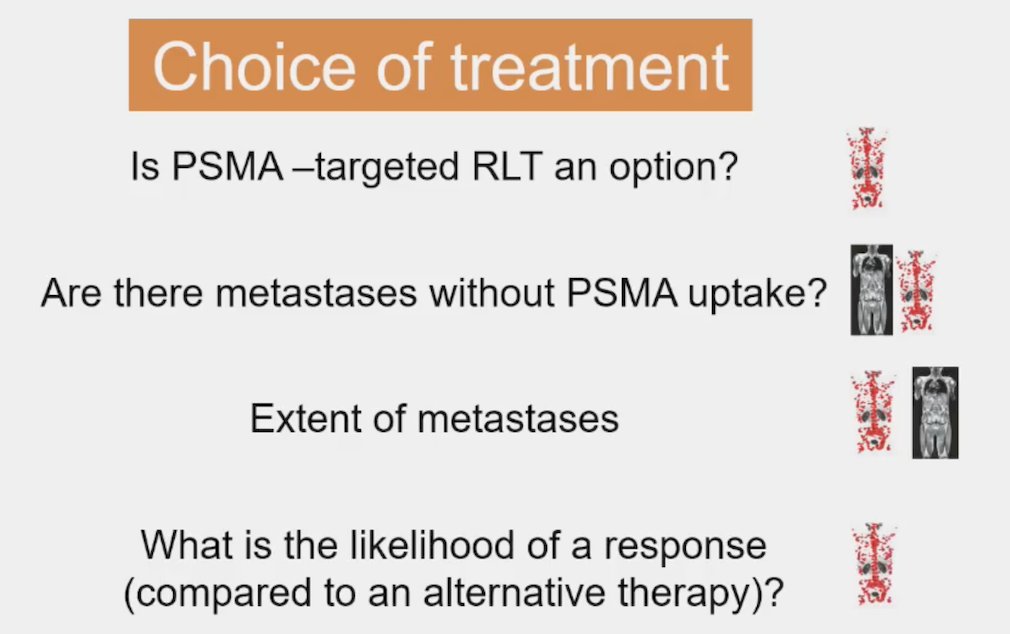
For managing treatment, Dr. O’Sullivan notes: (i) is treatment working? both whole body MRI and PSMA PET are adequate, with whole body MRI slightly better, (ii) are there potential issues ahead (ie. cord impingement)? Both whole body MRI and PSMA PET are adequate, with whole body MRI slightly better, (iii) should I have another cycle of radioligand therapy? PSMA PET is clearly better:
Ultimately, what we want reported in an MRI and PSMA PET is as much information as possible, primarily to help with decision making (treatment choice/life planning). Imaging also is key in the role of metastasis directed therapy, helping imaging experts understand the needs of oncologists (and their patients), and helping oncologists understand what is possible from imaging (and what is not possible). Moreover, we need to avoid unnecessary information, especially as more patients can now see their reports.
Dr. O’Sullivan concluded his presentation discussing what we should have reported in an MRI and PSMA PET by emphasizing what could we want to have reported:
- Standardized reports are needed
- Prospective trials must include molecular imaging
- Real world data
- Correlation between imaging data and other ‘omics’
Presented by: Joe O'Sullivan, MD, Patrick G. Johnston Centre for Cancer Research, Queen’s University Belfast and Northern Ireland Cancer Centre, Belfast, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.