(UroToday.com) The Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 held in Lugano, Switzerland was host to a session addressing the contemporary management of biochemically recurrent prostate cancer patients. Dr. Matthew Cooperberg discussed the role of genomic classifiers at the time of biochemical recurrence.
Dr. Cooperberg began by noting that although biochemical recurrence in the post-radical prostatectomy setting is defined by a serum PSA level ≥0.2 ng/ml, confirmed by a 2nd rising PSA level of >0.2 ng/ml, at least 30% of post-radical prostatectomy biochemical recurrences are over-diagnosed, with these patients unlikely to die of prostate cancer.1 As such, there is a need to judiciously incorporate biomarkers to guide the timing/intensity of secondary treatment.
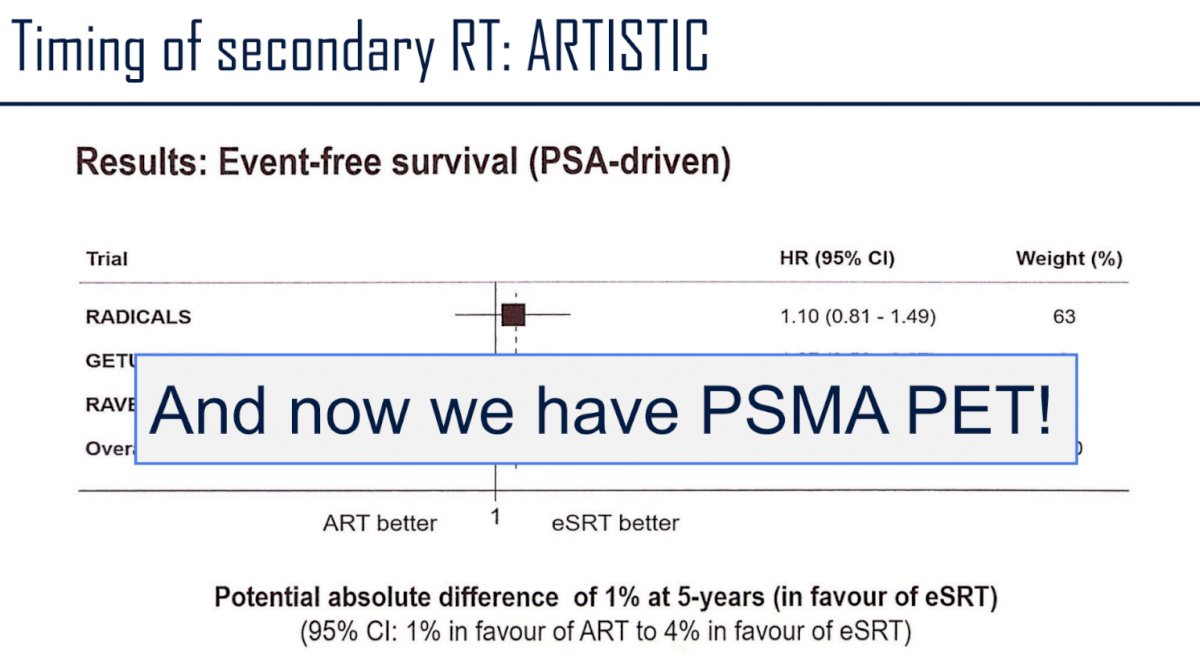
Currently, early salvage radiotherapy is preferred to adjuvant radiotherapy for the majority of prostate cancer patients in the post-radical prostatectomy setting. This recommendation is informed by the results of the ARTISTIC meta-analysis,2 which incorporated results from the RADICALS, RAVES, and GETUG-17 trials.3-5 With 1,075 patients included at a median follow-up of 60 to 78 months, this meta-analysis demonstrated no significant improvement in event-free survival with adjuvant radiotherapy, compared to early salvage treatment (HR: 0.95, 95% CI: 0.75-1.21, p=0.70), with only a single percentage point (95% CI: 2 - 3) improvement in the 5-year event-free survival (89% vs 88%).2
But, since the publication of these trials, we now have novel biomarkers that are available in this setting, including imaging, such as PSMA PET, to incorporate for risk stratification and disease localization in these patients.
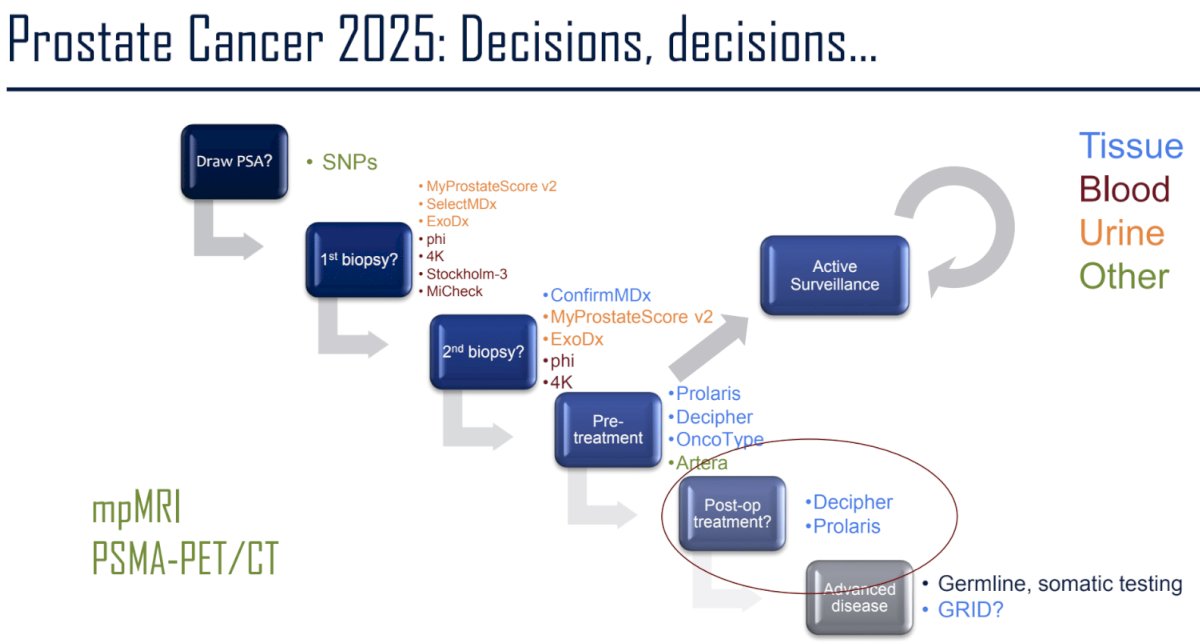
Additionally, there are now numerous tissue, blood, and urine-based biomarkers to help guide patient management across the prostate cancer landscape:
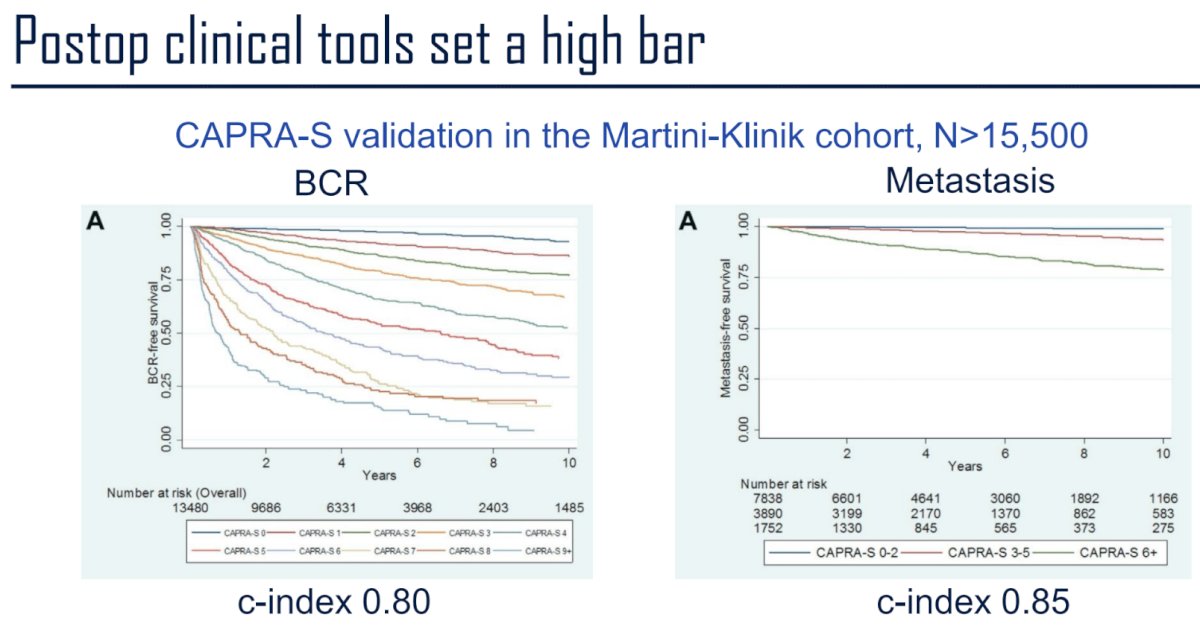
But, before incorporating these tools, many of which are expensive, we need to ask: “Do these biomarkers outperform commonly available clinical tools?”. In 2015, Tilki et al. validated the CAPRA-S score in a cohort of 14,532 patients from the Martini-Klinik who were treated with radical prostatectomy between January 1992 and August 2012 and followed for a median of 51 months. When stratifying patients by CAPRA-S risk group, the estimated 5-year biochemical recurrence-free survivals were 91.4%, 70.4%, and 29.3% in the low, intermediate, and high-risk groups, respectively. The CAPRA-S c-index to predict biochemical recurrence, metastasis, and cancer specific mortality was 0.80, 0.85, and 0.88, respectively
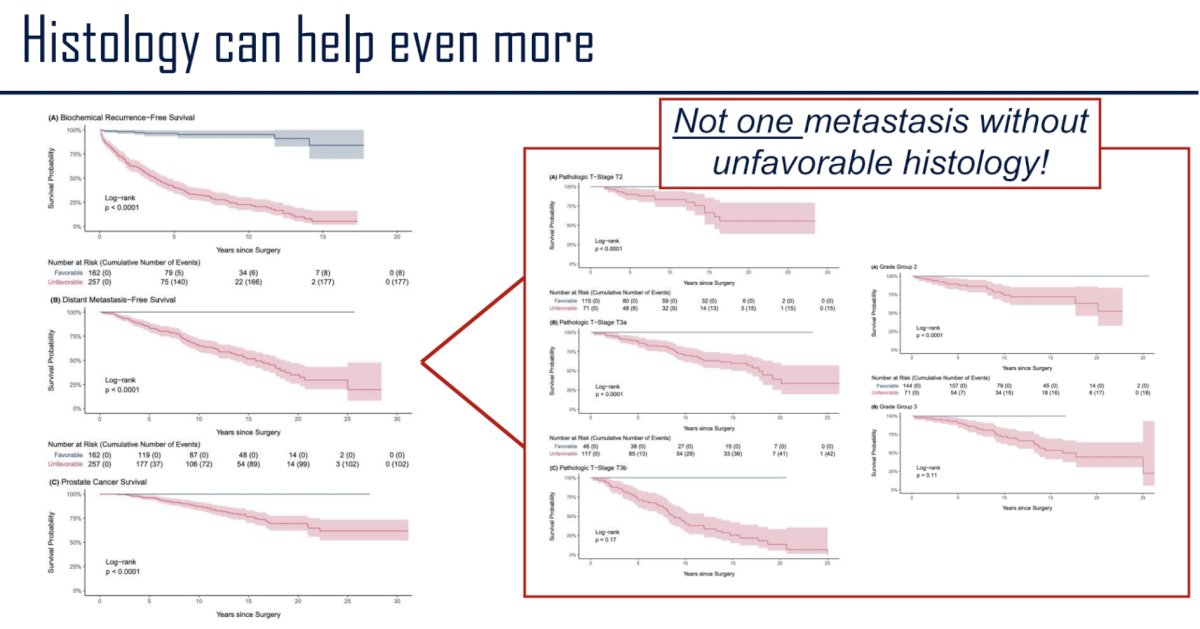
Histological grading is another powerful prognostic tool. In a pooled analysis of two post-radical prostatectomy cohorts (n=628), Nguyen et al. defined unfavorable histology using ≥1 of the following criteria:
- Gleason 5
- Large cribriform
- Intraductal
- Complex intraluminal papillary
- Grade 3 stromogenic
- Complex anastomosing cordlike

At 15 years, unfavourable histology predicted biochemical recurrence, with sensitivity of 93% and specificity of 88%, metastatic disease at 100% and 48%, and death at 100% and 46%. Grade Group 2 prostate cancers with unfavourable histology were associated with metastasis, independent of pathological stage, while those without had no risk. Notably, not one metastasis was observed in the absence of unfavorable histology. Multivariable Cox proportional hazards models demonstrated that unfavourable histology significantly improved the discriminatory power of the MSKCC post-prostatectomy nomogram for biochemical failure (likelihood ratio test p<0.001).7
He argued, however, that genomics can ‘definitely’ clear that bar set by clinical tools and pathology. Dr. Cooperberg’s team has previously demonstrated that incorporating the cell-cycle progression (CCP) score can enhance the prognostic utility of the CAPRA-S score alone to predict biochemical recurrence in radical prostatectomy patients.8 Similarly, the Decipher score has been shown to correlate with risk of metastasis following a radical prostatectomy.9

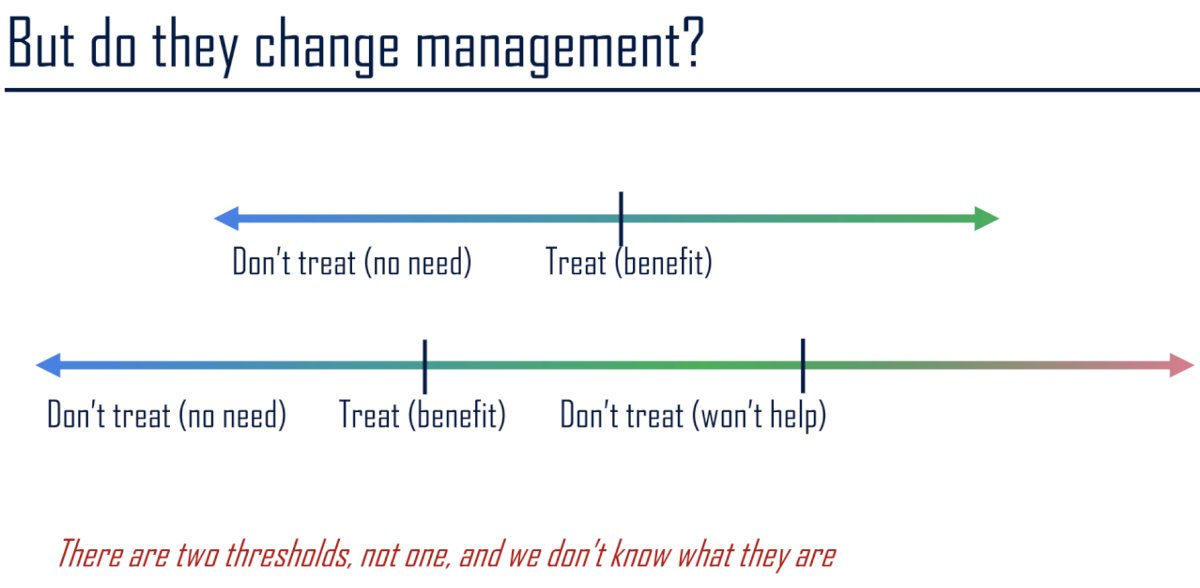
Ultimately, the important question is: Do these biomarkers/tools change management? There are two different thresholds here. Beyond the simple ‘treat patients with higher risk disease versus don’t treat those with lower risk disease’, we need to consider the fact that many patients with adverse prognoses may be ‘beyond salvageable’ and, despite their adverse prognoses, may not benefit from early aggressive treatment. As such, there are 2 thresholds, as depicted in the schematic below:
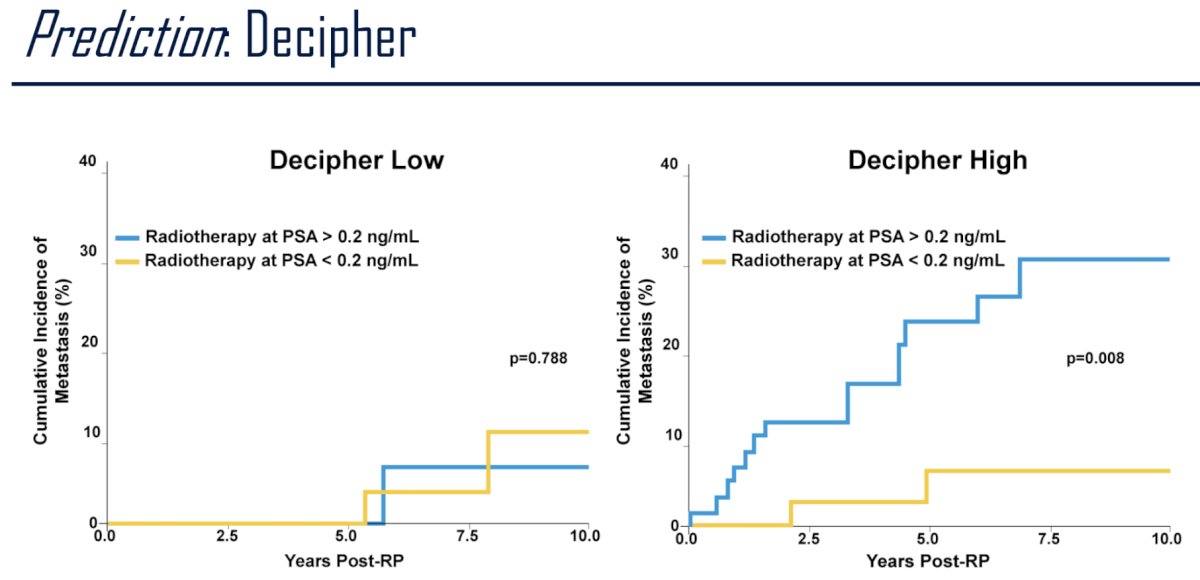
Moving to predictive biomarkers, Decipher has been shown to be predictive of treatment response to salvage radiotherapy in the post-prostatectomy setting. In Decipher low score patients, the incidence of distant metastases was the same irrespective of whether patients received radiotherapy at a PSA > or < 0.2 ng/ml. Conversely, for Decipher high score patients, those who received salvage radiotherapy at a PSA <0.2 ng/ml had significantly lower rates of developing metastases, compared to Decipher high score patients who received salvage radiotherapy at a PSA >0.2 ng/ml (p=0.008).10
Feng et al. have similarly validated the Decipher Genomic Classifier (GC) score in randomized phase III trial (NRG/RTOG 9601) demonstrating that the GC score (continuous variable, per 0.1 unit) was independently associated with distant metastases (HR: 1.17; p=0.006), prostate cancer-specific mortality (HR: 1.39; p<0 .001), and overall survival (HR: 1.17; p=0.002) after adjusting for age, race/ethnicity, Gleason score, T stage, margin status, entry prostate-specific antigen, and treatment arm. They additionally demonstrated that the absolute benefit of bicalutamide on 12-year overall survival was less when comparing patients with lower versus higher GC scores (2.4% vs 8.9%).11
In 2016, Zhao et al. developed a 24-gene Post-Operative Radiation Therapy Outcomes Score (PORTOS), derived from Decipher GRID, to predict which patients would benefit most from postoperative radiotherapy. They demonstrated that among patients with high PORTOS scores, patients who received radiotherapy had significantly lower rates of distant metastases. Conversely, among low PORTOS score patients, there was no benefit to radiotherapy.12
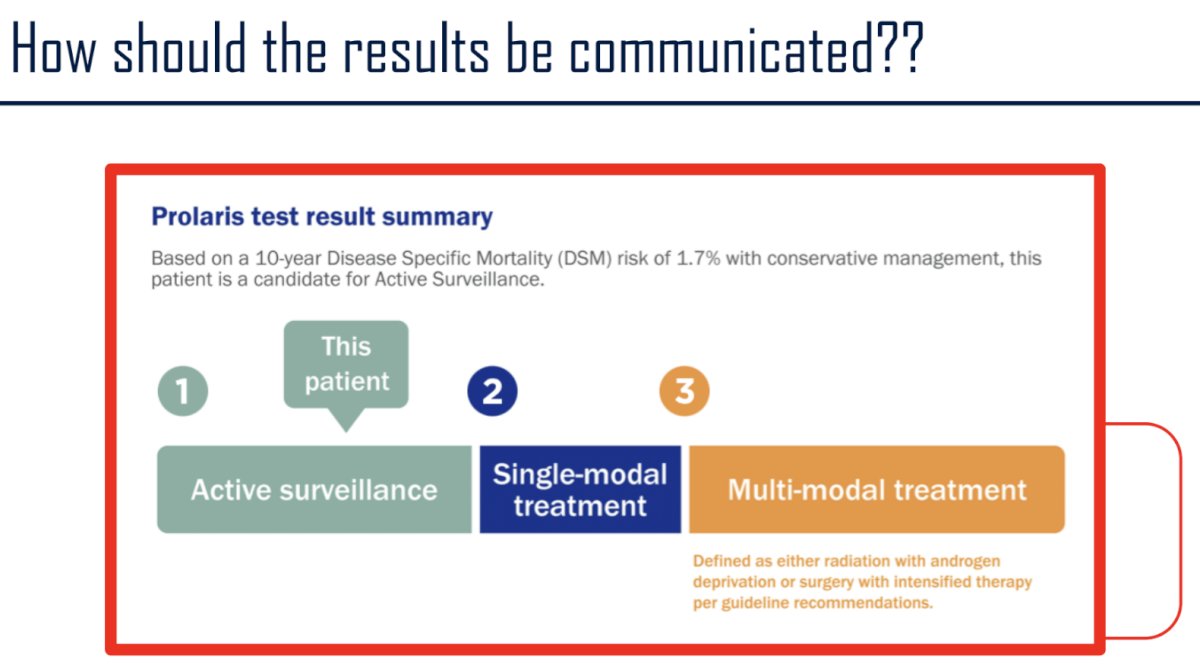
Finally, we cannot underestimate the way these results should be communicated to our patients:
Dr. Cooperberg concluded with the following remarks:
- The clearest role for markers in the post-operative biochemically recurrent setting in 2025 is the use of Decipher to guide intensification of salvage radiotherapy with ADT
- PORTOS and related signatures may help determine who should consider going straight to systemic treatment (i.e., per EMBARK)
- The interaction between genomics and PSMA PET is poorly elucidated so far
- We need more emphasis on the lower threshold—i.e., identifying those patients who should just stop checking PSA
Presented by: Matthew R. Cooperberg. MD, MPH, Professor of Urology and Epidemiology & Biostatistics and Helen Diller Family Chair in Urology at the University of California, San Francisco, CA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.
References:
- Xia J. Trock BJ, Mallinger L, et al. Overdetection of Recurrence after Radical Prostatectomy: Estimates Based on Patient and Tumor Characteristics. Clin Cancer Res. 2014; 20(20): 5302-10.
- Vale CL, Fisher D, Kneebone A, et al. Adjuvant or early salvage radiotherapy for the treatment of localised and locally advanced prostate cancer: a prospectively planned systematic review and meta-analysis of aggregate data. Lancet. 2020;396(10260):1422-1431.
- Parker CC, Clarke NW, Cook AD, et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): a randomised, controlled phase 3 trial. Lancet. 2020; 396(10260): 1413-1421.
- Kneebone A, Fraser-Browne C, Duchesne GM, et al. Adjuvant radiotherapy versus early salvage radiotherapy following radical prostatectomy (TROG 08.03/ANZUP RAVES): a randomised, controlled, phase 3, non-inferiority trial. Lancet Oncol. 2020; 21(10): 1331-1340.
- Sargos P, Chabaud S, Latorzeff I, et al. Adjuvant radiotherapy versus early salvage radiotherapy plus short-term androgen deprivation therapy in men with localised prostate cancer after radical prostatectomy (GETUG-AFU 17): a randomised, phase 3 trial. Lancet Oncol. 2020 ;21(10): 1341-1352.
- Tilki D, Mandel P, Schlomm T, et al. External validation of the CAPRA-S score to predict biochemical recurrence, metastasis and mortality after radical prostatectomy in a European cohort. J Urol. 2015; 193(6): 1970-5.
- Nguyen JK, Harik LR, Klein EA, et al. Proposal for an optimised definition of adverse pathology (unfavourable histology) that predicts metastatic risk in prostatic adenocarcinoma independent of grade group and pathological stage. Histopathology. 2024; 85(4):598-613.
- Cooperberg MR, Simko JP, Cowan JE, et al. Validation of a cell-cycle progression gene panel to improve risk stratification in a contemporary prostatectomy cohort. J Clin Oncol. 2013; 31(11): 1428-34.
- Ross AE, Johnson MH, Yousefi K, et al. Tissue-based Genomics Augments Post-prostatectomy Risk Stratification in a Natural History Cohort of Intermediate- and High-Risk Men. Eur Urol. 2016; 69(1):157-65.
- Den RB, Yousefi K, Trabulsi EJ, et al. Genomic Classifier Identifies Men With Adverse Pathology After Radical Prostatectomy Who Benefit From Adjuvant Radiation Therapy. J Clin Oncol. 2015; 33(8): 944-51.
- Feng FY, Huang HC, Spratt DE, et al. Validation of a 22-Gene Genomic Classifier in Patients With Recurrent Prostate Cancer: An Ancillary Study of the NRG/RTOG 9601 Randomized Clinical Trial. JAMA Oncol. 2021; 7(4): 544-52.
- Zhao SG, Changg SL, Spratt DE, et al. Development and validation of a 24-gene predictor of response to postoperative radiotherapy in prostate cancer: a matched, retrospective analysis. Lancet Oncol. 2016; 17(11): 1612-20.