(UroToday.com) The 2025 APCCC Diagnostics annual meeting featured a session on what we should know for PSMA radioligand therapy and a presentation by Dr. Oliver Sartor discussing what clinicians need to know from the PSMA radioligand therapy selection PET scan. Dr. Sartor notes that a caveat is that the context of today and the context of tomorrow may be distinct.
Currently, there are many standard therapies in prostate cancer, both in the castrate sensitive and castrate resistant disease spaces: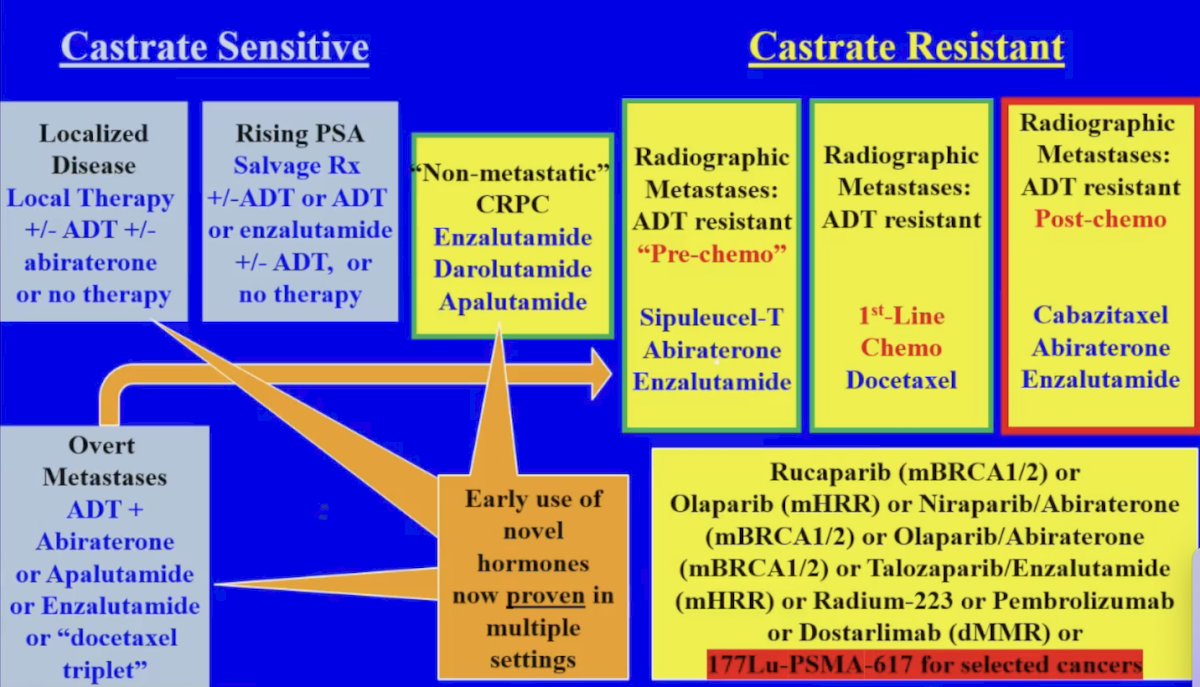
Dr. Sartor notes that one of the overriding concerns today is whether the patient is a candidate for radioligand therapy or not. With this question comes several other questions and considerations:
- Did the patient progress post-ADT/post androgen receptor pathway inhibitor and a taxane?
- Does the patient have metastatic disease with PSMA PET uptake greater than the liver?
- Does the patient have any exclusionary lesions with PSMA PET uptake less than the liver?
- Visceral lesions >=1 cm on CT/MRI?
- Soft tissue component of >1 cm (short axis)?
- Lymph node metastasis >= 2 cm?
- In VISION, about 13% of patients were excluded
- In PSMAfore, only about 8% of patients were excluded
When considering clinical decision making today for mCRPC, imaging is one parameter among many. Other parameters include:
- Availability of the treatment and costs: nothing happens if the patient cannot access the therapy
- Patient factors: performance status, age, comorbidities, laboratory assessments (WBC, platelets, liver function), and symptoms (how bad?)
- Germline and somatic genotype (ie. BRCA, etc)
- Pathology, histologic, and cytologic classification (as well as artificial intelligence)
- Prior therapies: types and timing, response, resistance, duration, and tolerance
- Burden of disease (oligometastatic versus more) and tumor volume
- Phenotype of disease: adenocarcinoma, neuroendocrine, amphicrine, etc
- Disease characteristics and kinetics: location of disease (bone, liver, nodes, prostate only, etc), kinetics of disease response/progression (rapid or slow), and new lesions (How many? Systemic or focal progression?)
- Image based biomarkers (ie. PSMA, FDG, etc), SUVmean
- Availability of clinical trial options
- Patient preferences
What the reader may tell clinicians currently is more than likely related to the VISION criteria,1 including (i) are metastatic lesions with uptake greater than the liver? and (ii) lesions on cross-sectional imaging not visualized on the PSMA PET (viscera, large nodes, soft tissue of lytic bone lesions). However, Dr. Sartor emphasizes that there is more to the story:
- Number of lesions (oligo or polymetastatic disease)
- Location of lesions (bone, nodes, liver, etc)
- Size of selected lesions
- SUVmean and SUVmax
- Total tumor volume
- Heterogeneity/homogeneity of lesions (more work is needed)
- Comparisons to other PETs (FDG, etc)
- Comparisons to the last PET (total tumor volume, new lesions, etc)
Previous work from the VISION trial presented at ASCO 2022, assessed the prognostic ability of the baseline 68Ga-PSMA-11 PET scan. This analysis showed that a higher whole-body SUVmean was associated with improved radiographic progression free survival: highest SUVmean quartile - 14.1 months versus lowest quartile - 5.8 months (multivariable analysis: HR 0.86, 95% CI 0.82 - 0.90):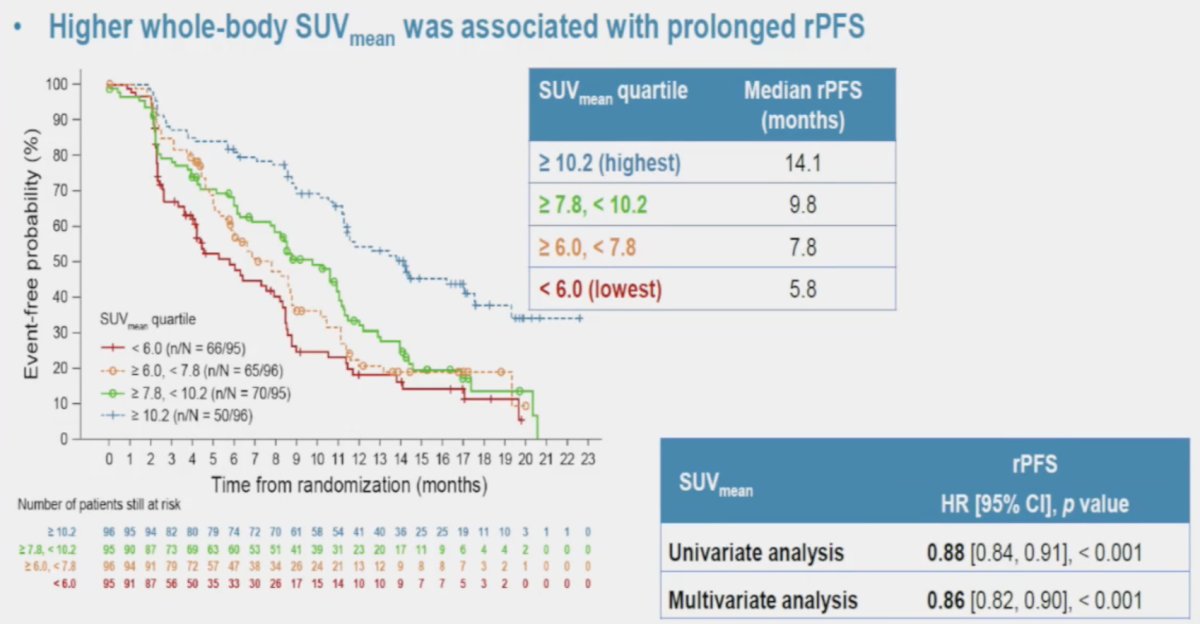
When assessing the association of these quartiles of whole body SUVmean with overall survival, again, there was a significant stratification between the groups. Notably, among these patients who received 177Lu-PSMA-617, those with the highest SUVmean levels had the longest overall survival (21.4 months; multivariable analysis HR 0.88, 95% CI 0.84 - 0.91):
At ASCO 2024, Kwon and colleagues presented data from the TheraP trial2 assessing ctDNA fraction as a predictor of treatment efficacy of 177Lu-PSMA-617 versus cabazitaxel. ctDNA <2% was associated with a significant improvement when treated with 177Lu-PSMA-617 compared with cabazitaxel, with an 8.7 month increase in the median progression free survival (HR 0.12, 95% CI 0.04-0.38), which was confirmed on multivariable analysis adjusting for PSMA SUVmean and other clinical prognostic factors (HR 0.35, 95% CI 0.13-0.93; interaction p = 0.035):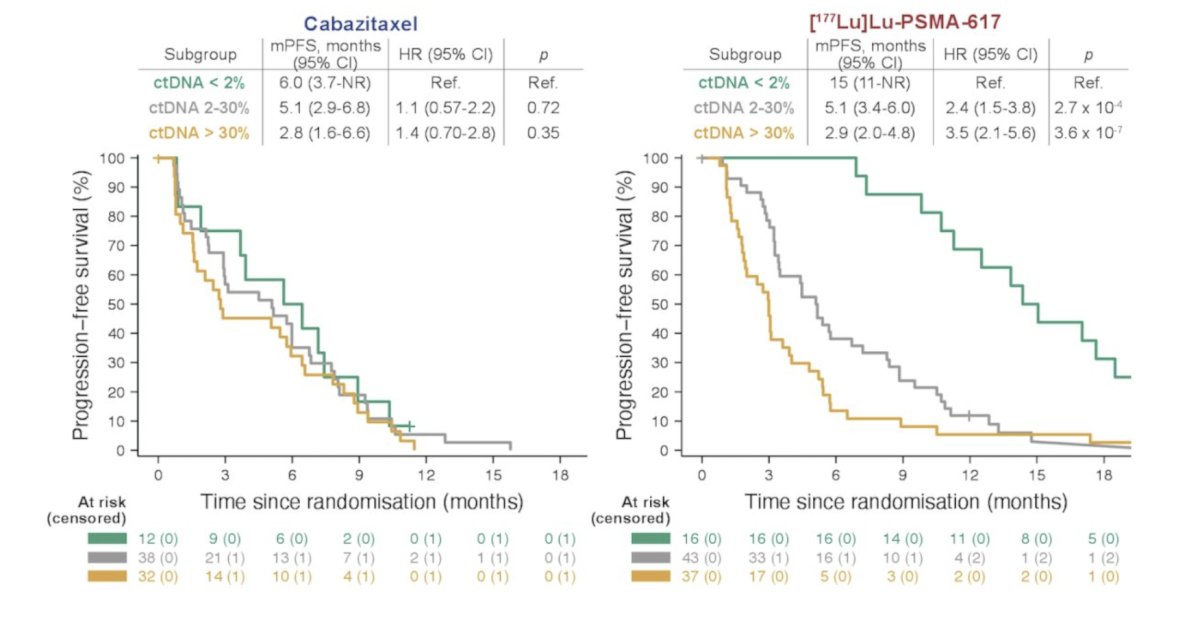
Dr. Sartor concluded his presentation discussing what clinicians need to know from the PSMA radioligand therapy selection PET scan with the following take-home points:
- The clinician will view the images, taking into account many other variables, to decide on the therapy that is best for the patient
- That therapy may or may not including radioligand therapy
- In the future, we will need to assess criteria again, but much progress has been made to date
Presented by: A. Oliver Sartor, MD, Medical Oncologist, Professor of Medicine, Urology and Radiology, Director, Radiopharmaceutical Trials, Mayo Clinic, Rochester, MN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.