(UroToday.com) The 2025 APCCC Diagnostics annual meeting featured a session on how to stage and estimate risk for prostate cancer and a presentation by Dr. Daniel Spratt discussing the added value of risk stratification using a genomic classifier for localized prostate cancer.
Dr. Spratt started his presentation by emphasizing a statement from the NCCN 2025 Guidelines regarding the personalizing treatment of localized prostate cancer: “The primary method for personalization of treatment from localized to advanced prostate cancer is based on prognostic risk stratification.” This rationale for prognostication and personalization is assuring appropriate treatment (active surveillance versus intervention) with the appropriate treatment modality when indicated, in an attempt to not over/under treat patients. This is highlighted in the following figure, emphasizing the number needed to treat: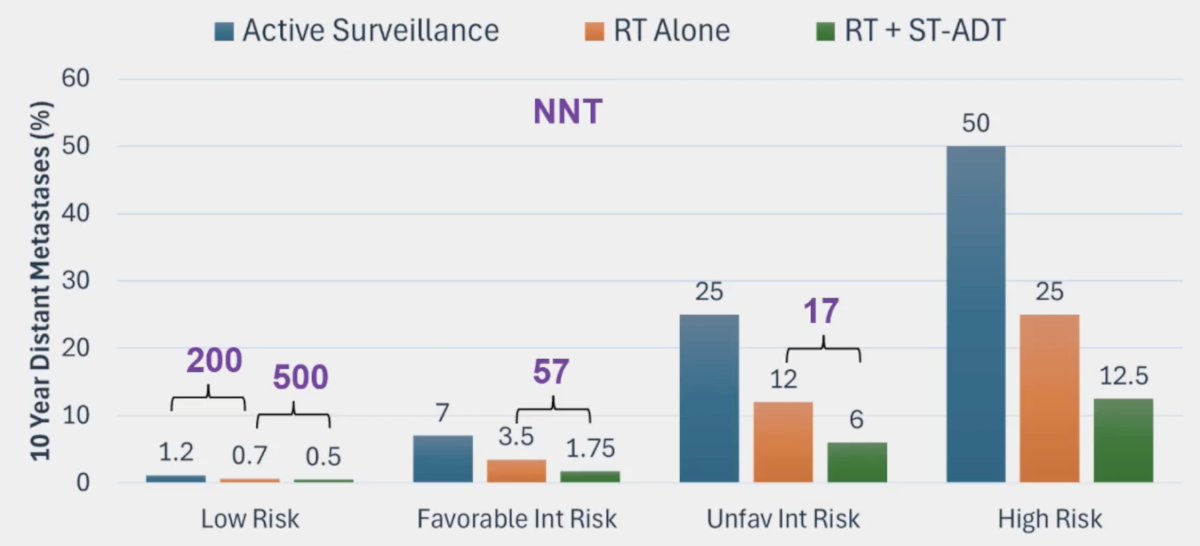
How do we personalize treatment in localized prostate cancer? Dr. Spratt notes that the NCCN 2025 guidelines have standard tools (TNM stage, grade group, PSA, percent positive cores), clinical and pathologic tools (multivariable models, nomograms, histologic features, PSA kinetics), as well as advanced tools (genetics/genomics, digital pathology-based artificial intelligence, circulating markers):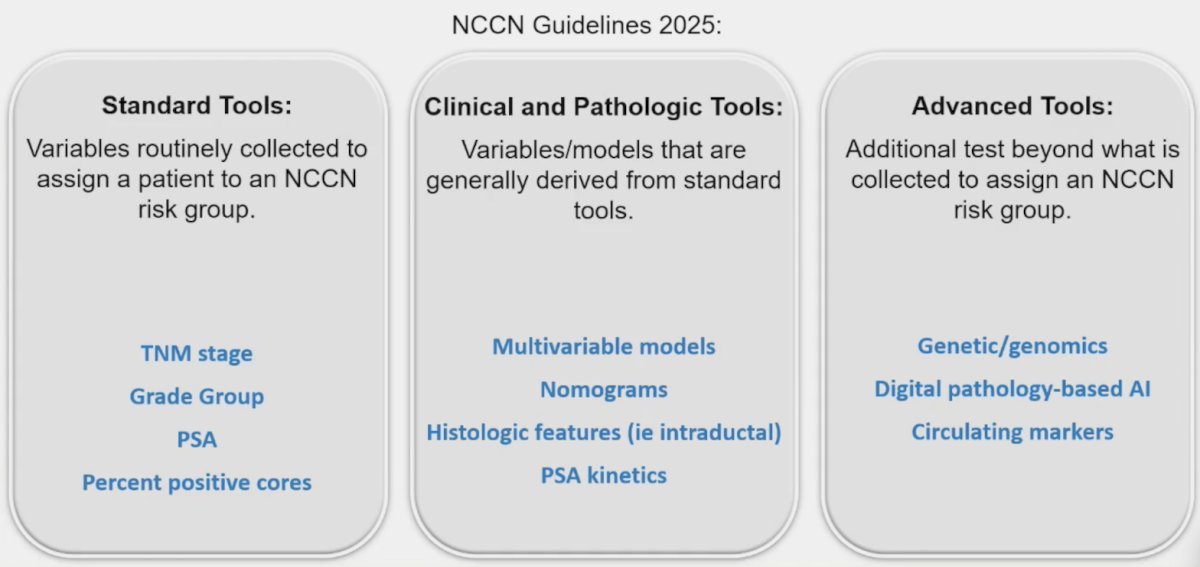
The standard tools are variables routinely collected to assign a patient to an NCCN risk group and are not optimized for prognostication. Dr. Spratt also notes that the clinical and pathologic tools are variables/models that are generally derived from standard tools, and as such, are also not optimized for prognostication. The NCCN 2025 guidelines make the following statements for select advanced tools to improve risk stratification:
- “There are an extensive number of these tools created with substantial variability in quality of reporting and model design, endpoint selection, and quality of validation.”
- “It is recommended to use models that have robust validation, ideally with high quality, long-term clinical trial data, which usually comes from randomized trials and across multiple clinical trials.”
The two advanced tools to improve risk stratification supported by the NCCN are the 22-gene genomic classifier Decipher, and the multi-modal artificial intelligence ArteraAI Prostate test. For the remainder of his presentation, Dr. Spratt focused on the Decipher genomic classifier. He notes that the majority of tests (99.99%) fail to move past the stage of “retrospective institutional data”, which is near useless clinically. Over the last number of years, the Decipher genomic classifier has developed robust validation.
Dr. Spratt and colleagues have previously validated Decipher in the post-prostatectomy setting, demonstrating consistency in performance. In their systematic review,1 they included five studies, with 975 total patients, of which 855 patients had individual patient-level data. Of the total cohort, 60.9%, 22.6%, and 16.5% of patients were classified by Decipher as low, intermediate, and high risk, respectively. Over a median follow-up of 8 years, the 10-year cumulative incidence metastases rates were 5.5%, 15.0%, and 26.7% (p < 0.001), respectively, for the three risk classifications.
Their subsequent work with Decipher has provided integration of the biomarker with standardized risk stratification tools. In his group’s seminal work published in 2018,2 the aim of their study was to develop a novel clinical-genomic risk grouping system that can readily be incorporated into treatment guidelines for localized prostate cancer. Over a median follow-up of 8 years for patients in the training cohort, 10-year distant metastasis rates for NCCN low, favorable-intermediate, unfavorable-intermediate, and high-risk were 7.3%, 9.2%, 38.0%, and 39.5%, respectively. In contrast, the three-tier clinical-genomic risk groups had 10-year distant metastasis rates of 3.5%, 29.4%, and 54.6%, for low-, intermediate-, and high-risk, respectively, which were consistent in the validation cohort. C-indices for the clinical-genomic risk grouping system (0.84; 95% CI, 0.61 to 0.93) were improved over NCCN (0.73; 95% CI, 0.60 to 0.86) and CAPRA (0.74; 95% CI, 0.65 to 0.84). The following figure shows reclassification of NCCN risk groups to clinical-genomic risk groups in the prospective cohort: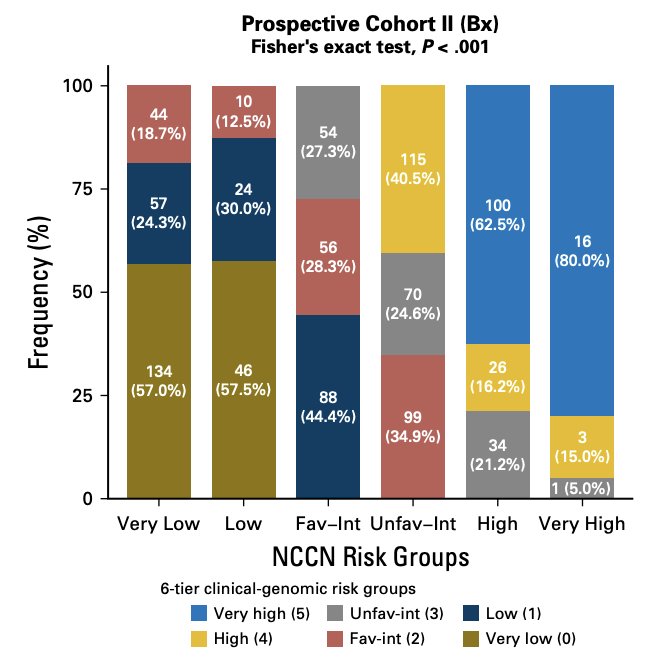
Subsequently, Decipher has been validated in 12 randomized phase III trials, and as of 2022, it has been validated in 42 studies in 30,407 patients. Moreover, as of 2023, there has been linkage with SEER and real world validation with >50,000 patients:
The following table from the NCCN 2025 guidelines summarizes the treatment implications for the Decipher genomic classifier: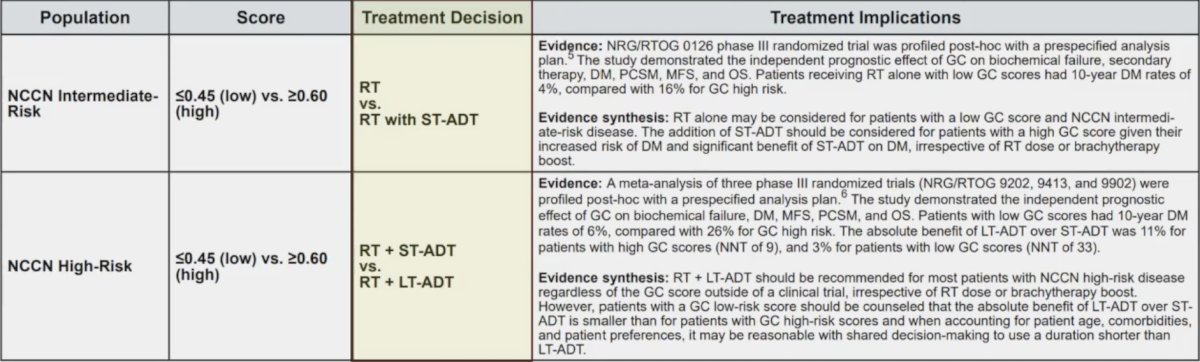
Dr. Spratt also highlighted the studies providing validation of Decipher in intermediate risk prostate cancer with radiotherapy alone, first in a Princess Margaret Hospital registry, and also in the NRG/RTOG 0126 randomized trial:
In 2023, Nguyen et al.3 validated Decipher in high risk patients, stratifying which patients benefit from short term versus long term androgen deprivation therapy (ADT). They found that based on the 10 year difference in distant metastasis, among Decipher high patients, the number needed to treat for short term ADT versus long term ADT is 9, and for Decipher low patients is 33: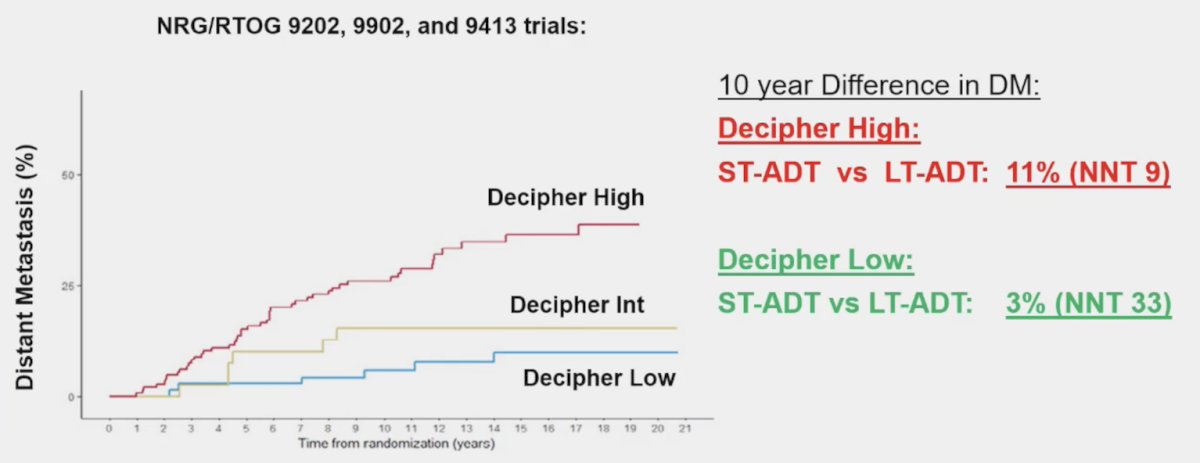
Finally, Dr. Attard and colleagues have recently validated Decipher in very high risk patients using the STAMPEDE dataset to determine who benefits from the addition of abiraterone. Notably, among those with localized high risk disease, patients with a Decipher genomic classifier score below the median had minimal benefit from the addition of abiraterone: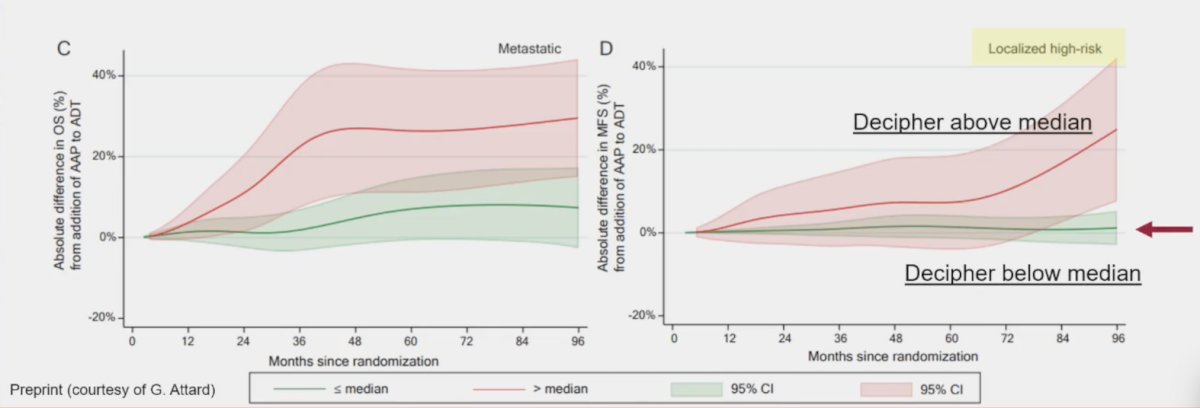
Dr. Spratt notes that Decipher has been incorporated into numerous ongoing multi-national phase III trials, including the NRG GU010 GUIDANCE trial assessing the use and intensity of ADT, and the NRG GU009 PREDICT RT trial assessing the duration and intensity of ADT. Moreover, Decipher has been used prospectively in FORMULA-509, NRG GU002, and NRG GU006, all of which are completed trials.
Dr. Spratt concluded his presentation discussing the added value of risk stratification using a genomic classifier for localized prostate cancer by emphasizing that currently, most patients receive imprecise medicine and inaccurate medicine. Our goal is that genomics can help improve both accuracy and precision: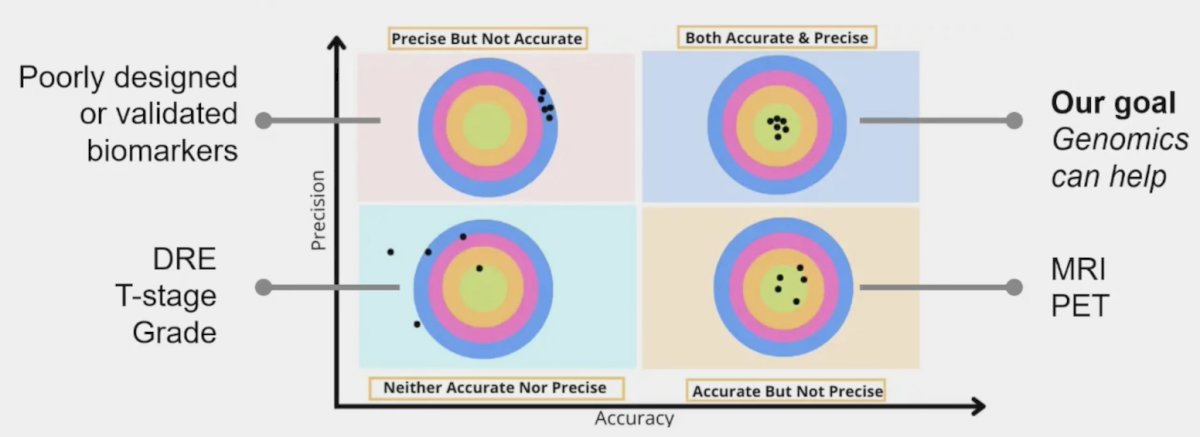
Presented by: Daniel E. Spratt, MD, University Hospitals Seidman Cancer Center, Case Western Reserve University, Cleveland, OH
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.
References:
- Spratt DE, Yousefi K, Deheshi S, et al. Individual Patient-Level Meta-Analysis of the Performance of the Decipher Genomic Classifier in High-Risk men after prostatectomy to predict development of metastatic disease. J Clin Oncol. 2017 Jun 20;35(18):1991-1998.
- Spratt DE, Zhang J, Santiago-Jimenez M, et al. Development and validation of a novel integrated clinical-genomic risk group classification for localized prostate cancer. J Clin Oncol 2018 Feb 20;36(6):581-590.
- Nguyen PL, Huang HR, Spratt DE, et al. Analysis of a biopsy-based genomic classifier in high-risk prostate cancer: Meta-analysis of the NRG Oncology/Radiation Therapy Oncology Group 9202, 9413, and 9902 phase 3 randomized trials. Int J Radiat Oncol Biol Phys. 2023 Jul 1;116(3):521-529.