(UroToday.com) The 2025 APCCC Diagnostics annual meeting featured a session on how to stage and estimate risk for prostate cancer and a presentation by Dr. Derya Tilki discussing which patients need additional imaging for prostate cancer staging. The EAU Guideline recommendations for staging of prostate cancer include:
- Any risk group staging: use pre-biopsy MRI for local staging information (Weak)
- Low-risk localized disease: do not use additional imaging for staging purposes (Strong)
- Intermediate risk disease: for patients with ISUP grade group 3 disease, perform PSMA PET/CT if available to increase accuracy or at least cross-sectional abdominopelvic imaging and a bone scan (Weak)
- High risk localized disease/locally advanced disease: perform metastatic screening using PSMA PET/CT if available or at least cross-sectional abdominopelvic imaging and a bone scan (Strong)
Moreover, the NCCN guidelines also recommend additional staging for unfavorable intermediate, high, and very high risk prostate cancer. With regards to conventional staging with CT or MRI and bone scan, Dr. Tilki notes that abdominal CT and MRI indirectly assess nodal invasion by using lymph node diameter and morphology. Lymph nodes with a short axis > 8 mm in the pelvis and > 10 mm outside the pelvis are considered malignant. The mean bone scan positivity rate in 23 different series was 2.3% in patients with PSA levels < 10 ng/mL, 5.3% in patients with PSA levels between 10.1 and 19.9 ng/mL, and 16.2% in patients with PSA levels of 20.0-49.9 ng/mL.1
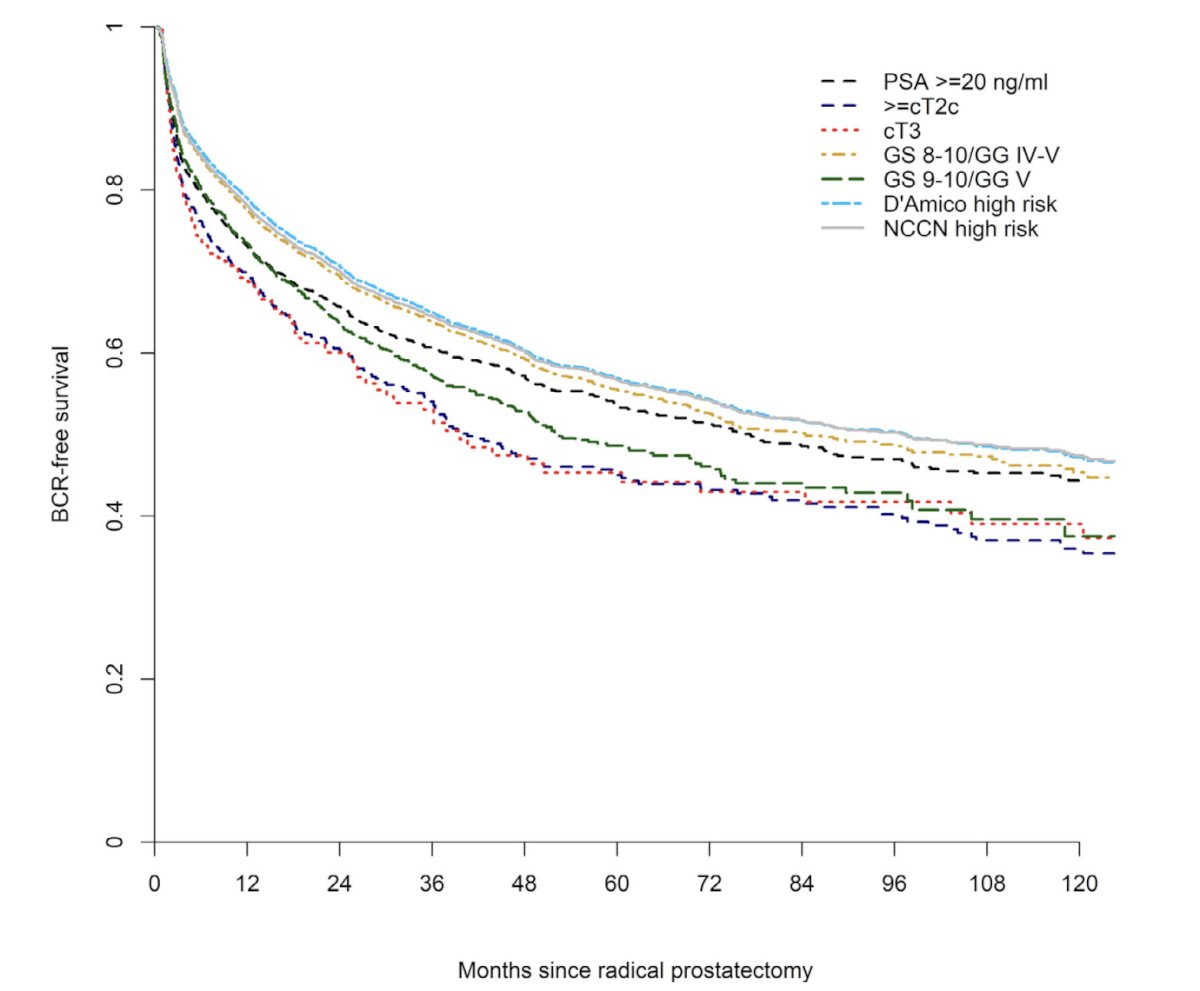
Previous work from Dr. Tilki’s group found that patients with high risk disease have a 10 year recurrence rate of 45-65% after primary therapy, and this failure rate is in great part a result of micrometastases, given negative conventional imaging at diagnosis:2
The proPSMA study3 found that PSMA PET-CT had a 27% greater accuracy than that of conventional imaging (92% versus 65%), with subgroup analyses also showing the superiority of PSMA PET/CT for patients with pelvic nodal metastasis (AUC 91% versus 59%) and for patients with distant metastases (AUC 95% versus 74%). In a head to head comparison of PSMA PET and conventional imaging, Chow et al.4 found that among 6 studies (687 patients), PSMA PET was also significantly more sensitive and specific than CT by a larger absolute difference of 34.7 percentage points and 14.1 percentage points, respectively.
Do bone scans over stage disease compared with PSMA PET at initial staging? In 2023, Dr. Hope and colleagues performed a multicenter retrospective diagnostic study of 167 patients with prostate cancer who were imaged with bone scans and PSMA PET performed within 100 days. In patients at initial staging, the PPV, NPV, and specificity for bone scans were 0.43 (95% CI, 0.26-0.63), 0.94 (95% CI, 0.85-0.98), and 0.80 (95% CI, 0.68-0.88), respectively, suggesting that the PPV of bone scans was low in patients at initial staging, with 57% of positive bone scans being falsely positive:5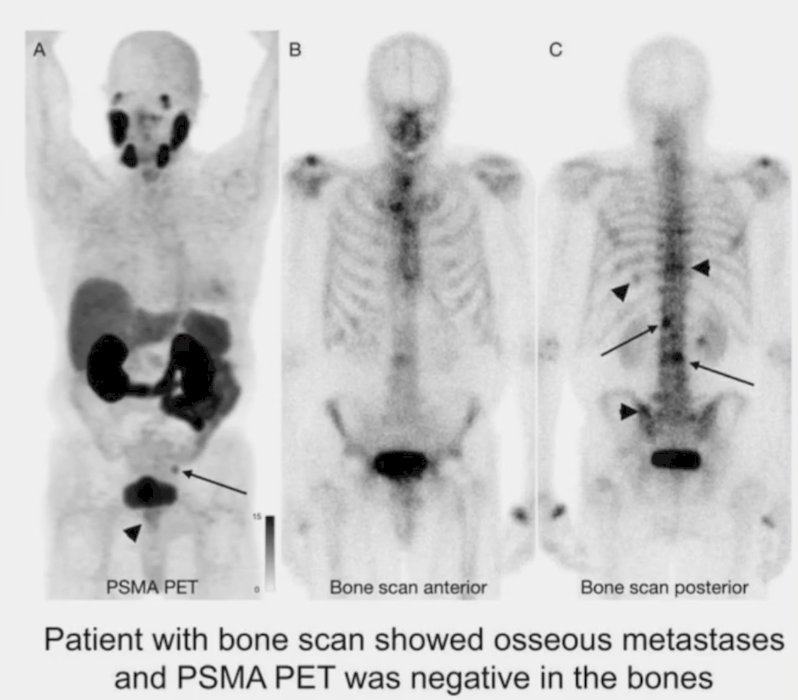
Recently, Luining et al.6 performed a comparison of globally applied prognostic risk groups and assessed the prevalence of metastatic disease on PSMA PET in 2,630 newly diagnosed prostate cancer patients. They found that metastatic disease was observed in 35% of patients, and according to NCCN stratification, metastatic disease was noted in 5.8%, 13%, 22%, and 62% of favorable intermediate, unfavorable intermediate, high, and very high risk prostate cancer patients, respectively.
One of the important questions with PSMA PET is how it affects decision making for treatment. In 2020, Ferraro et al.7 assessed the performance of 68Ga-PSMA-11 PET for staging of 116 intermediate and high-risk prostate cancer patients and its potential impact on disease management. Compared with conventional imaging, PSMA PET resulted in new information in 36% of the patients. In 27% of patients, this information would have changed management to a different therapy modality (13%) or adjusted treatment details (ie. modification of radiotherapy field or lymph node dissection template; 14%):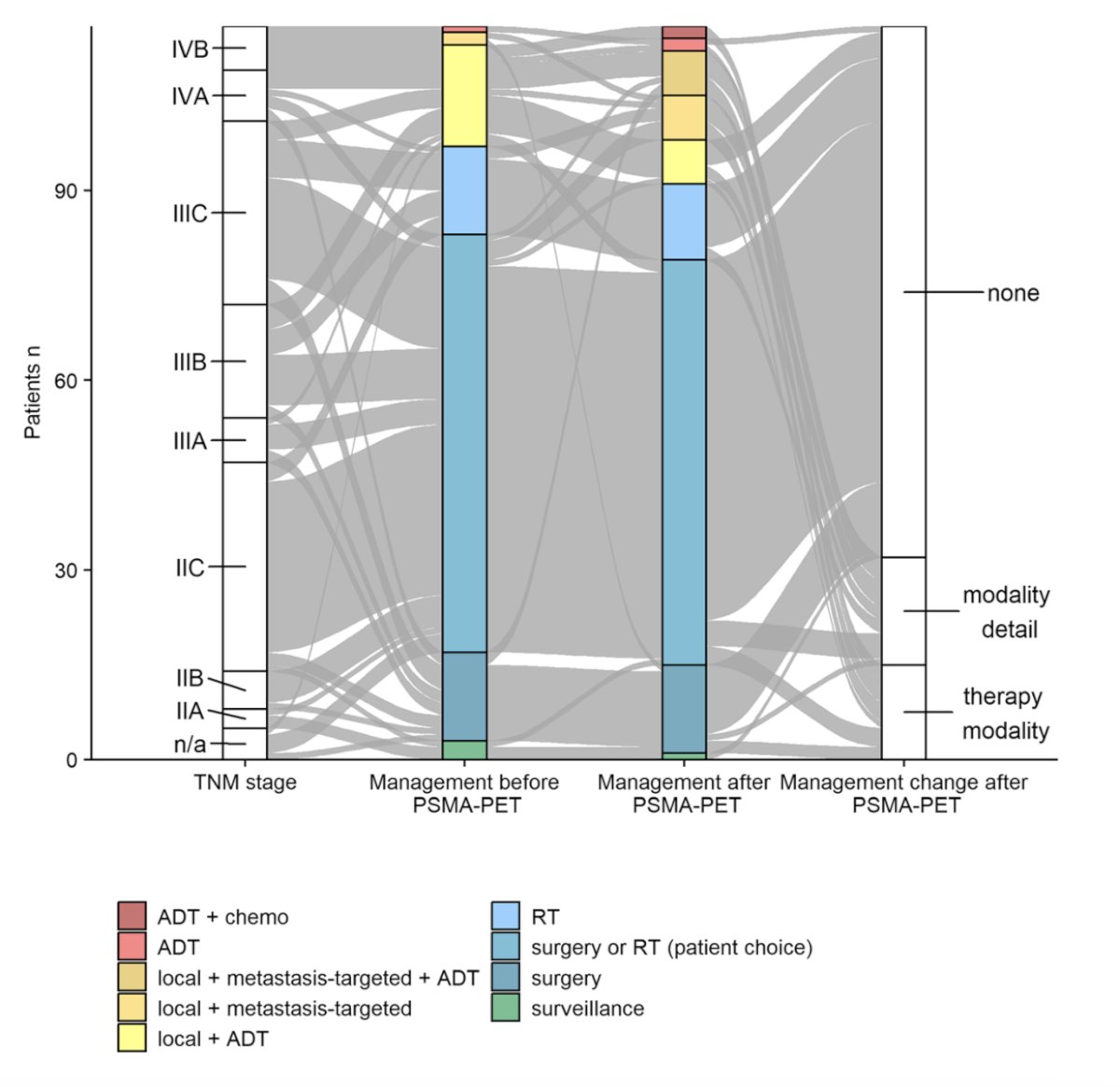
Dr. Tilki then highlighted several of the APCCC Diagnostics 2025 consensus questions and their respective answers:
Q24: If biopsy was done without prostate MRI, do you recommend a prostate MRI prior to radical prostatectomy for surgical planning (ie. nerve-sparing)?
- Yes, in the majority of patients (84%)
- Yes, but only if cT3 on DRE or other features of high risk suspicion of more advanced prostate cancer (10%)
- No (6%)
Q29: Do you recommend staging by conventional imaging (CT and bone scintigraphy) for patients with favorable intermediate risk (Gleason 3+4) and pre-biopsy MRI in the majority of patients?
- Yes, in the majority of patients (13%)
- Yes, but only if PSMA PET/CT is not available (24%)
- No, I do not stage patients with favorable intermediate risk disease (63%)
Q30: Do you recommend staging by conventional imaging (CT and bone scintigraphy) for patients with unfavorable intermediate risk (Gleason 4+3) and pre-biopsy MRI in the majority of patients?
- Yes, in the majority of patients (2%)
- Yes, but only if PSMA PET/CT is not available (91%)
- No, I do not stage patients with unfavorable intermediate risk disease (7%)
Q31: Do you recommend PSMA PET/CT as a staging tool in patients with clinically high-risk localized/locally advanced prostate cancer?
- Yes, in the majority of patients (95%)
- Yes, but only in selected patients with very high risk disease or inconclusive conventional imaging (5%)
- No, I recommend conventional imaging (0%)
Q32: Do you recommend whole-body MRI instead of PSMA PET/CT as a staging tool in the majority of patients with clinically high risk localized/locally advanced prostate cancer?
- Yes (0%)
- Both are equally accurate and can be used (15%)
- No (85%)
Dr. Tilki concluded her presentation discussing which patients need additional imaging for prostate cancer staging with the following take-home points:
- Staging is recommended in unfavorable intermediate and high risk prostate cancer
- Conventional imaging techniques are insufficient for preoperative staging in patients with high risk prostate cancer
- PSMA PET/CT has superior sensitivity and specificity, and small lymph node metastases may be missed
- The management impact of PSMA PET needs further evaluation
- Further research will be necessary to interpret the available results of randomized trials in a post-PSMA PET setting
Presented by: Derya Tilki, MD, Martini-Klinik Prostate Cancer Center, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Advanced Prostate Cancer Consensus Conference (APCCC) Diagnostics 2025 Annual Meeting, Virtual and Lugano, Switzerland, Thurs, Feb 27 – Fri, Feb 28, 2025.
References:
- Abuzallouf S, Dayes I, Lukka H. Baseline staging of newly diagnosed prostate: A summary of the literature. J Urol. 2004 Jun;171(6 Pt 1):2122-2127.
- Knipper S, Karakiewicz PI, Heinze A, et al. Definition of high-risk prostate cancer impacts oncological outcomes after radical prostatectomy. Urol Oncol. 2020 Apr;38(4)184-190.
- Hofman MS, Lawrentschuk N, Francis, RJ, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomized, multicentre study. Lancet 2020 Apr 11;395(10231):1208-1216.
- Chow KM, So WZ, Lee HJ, et al. Head-to-head comparison of the diagnostic accuracy of Prostate-specific Membrane Antigen Positron Emission Tomography and Conventional Imaging Modalities for Initial Stating of Intermediate- to High-risk Prostate Cancer: A Systematic Review and Meta-analysis. Eur Urol. 2023 Jul;84(1):36-48.
- Hope TA, Benz M, Jiang F, et al. Do bone scans overstage disease compared with PSMA PET at initial staging? An International multicenter retrospective study with masked independent readers. J Nucl Med. 2023 Nov;64(11):1744-1747.
- Luining WI, Boeve LMS, Hagens MJ, et al. A comparison of globally applied prognostic risk groups and the prevalence of metastatic disease on prostate-specific membrane antigen positron emission tomography in patients with newly diagnosed prostate cancer. Eur Urol Oncol. 2024 Apr 30: S2588-9311(24)00097.
- Ferraro DA, Schuler HIG, Muehlematter UJ, et al. Impact of 68Ga-PSMA-11 PET staging on clinical decision-making in patients with intermediate or high-risk prostate cancer. Eur J Nucl Med Mol Imaging. 2020 Mar;47(3):652-664.