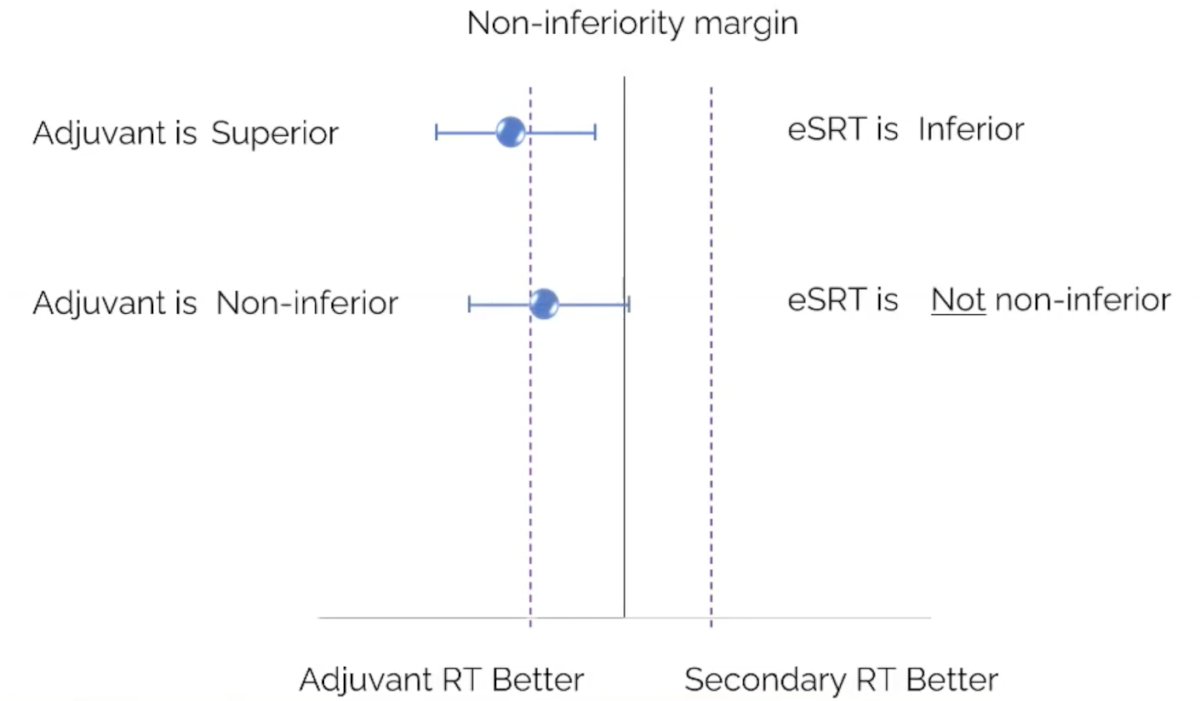
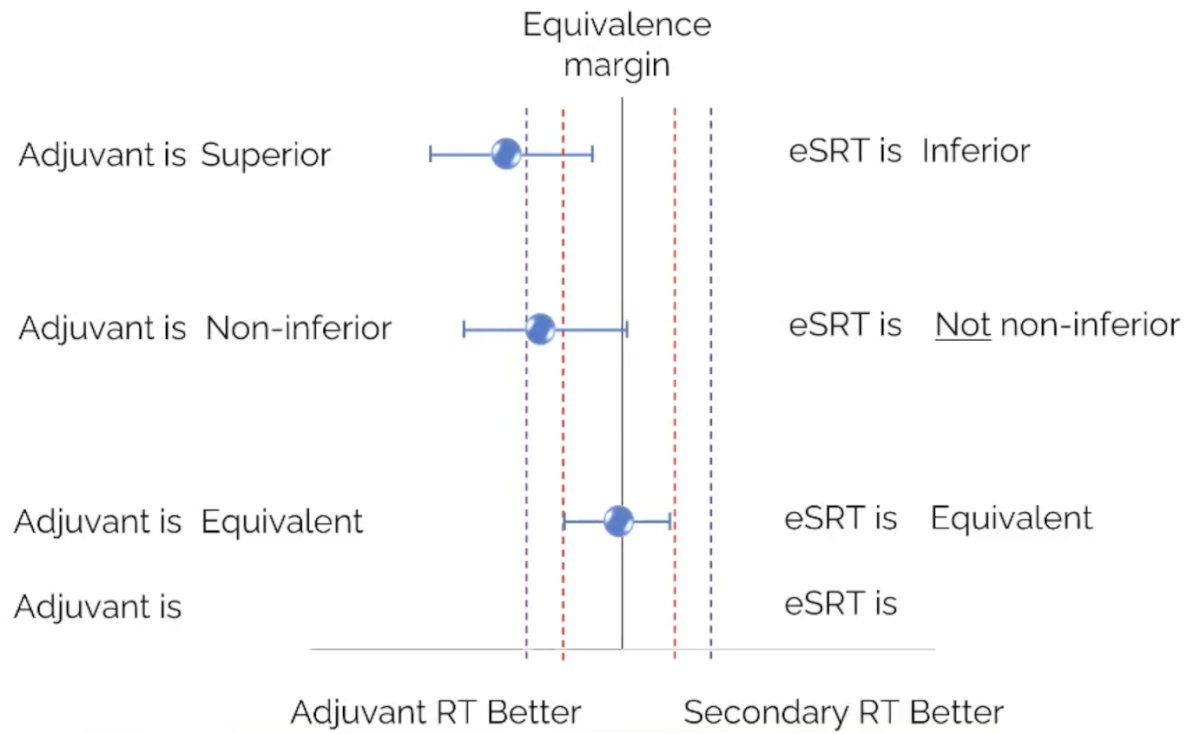
(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a treatment of PSA recurrence or persistence session and a presentation by Dr. Daniel Spratt discussing that early salvage radiotherapy is not equivalent to adjuvant radiotherapy in patients with high-risk localized or locally advanced disease. Dr. Spratt notes that, given that early salvage radiotherapy is not equivalent to adjuvant radiotherapy, the person making the claim has the burden to provide proof for that claim, not the one dismissing it. Dr. Spratt provided a biostatistics crash course explaining superiority and non-inferiority margins:
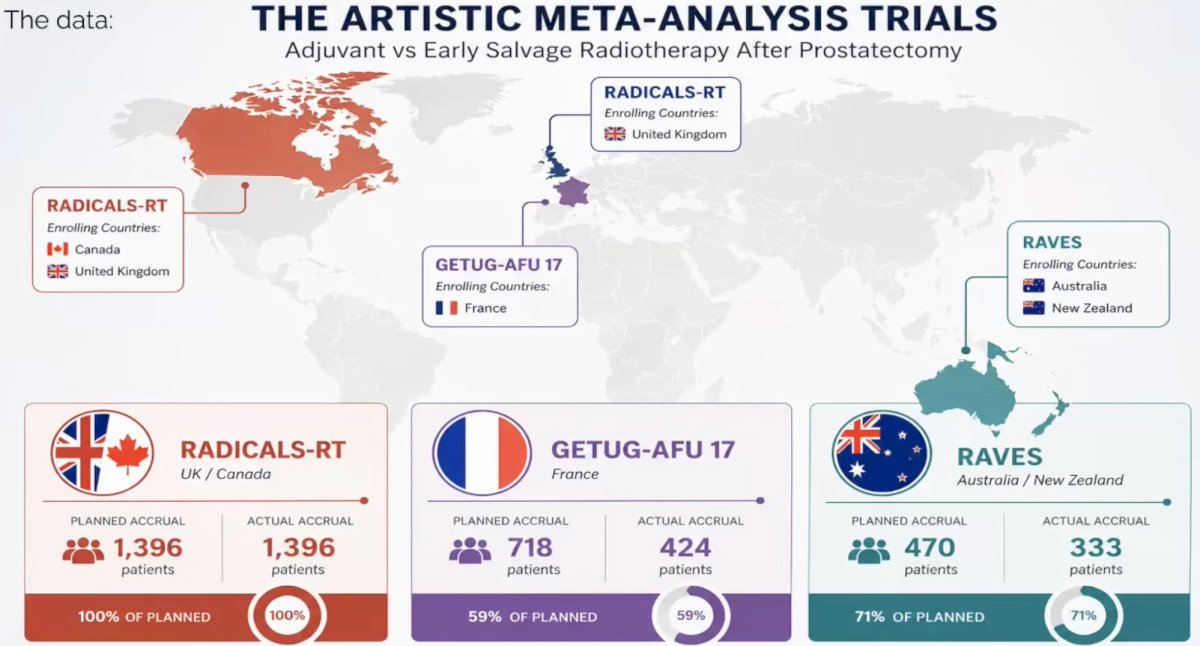
Dr. Spratt then discussed the ARTISTIC meta-analysis1 assessing adjuvant versus early salvage radiotherapy after prostatectomy:
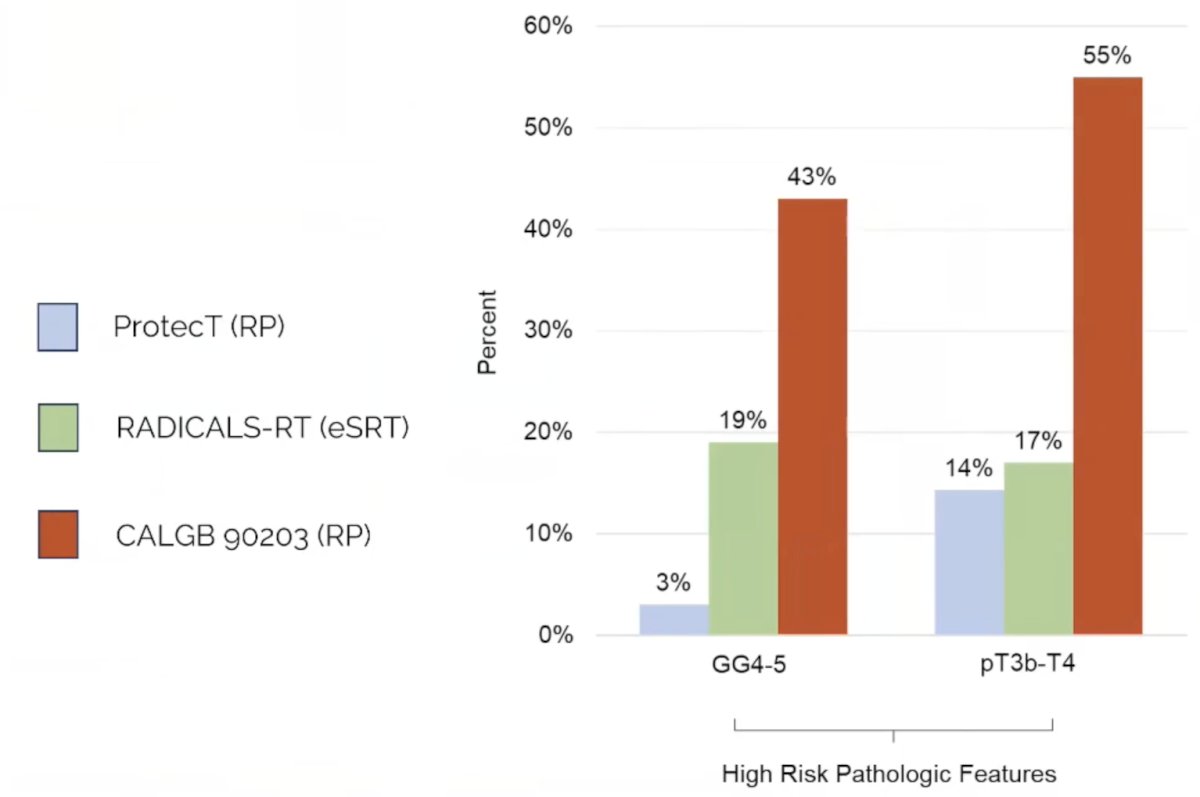
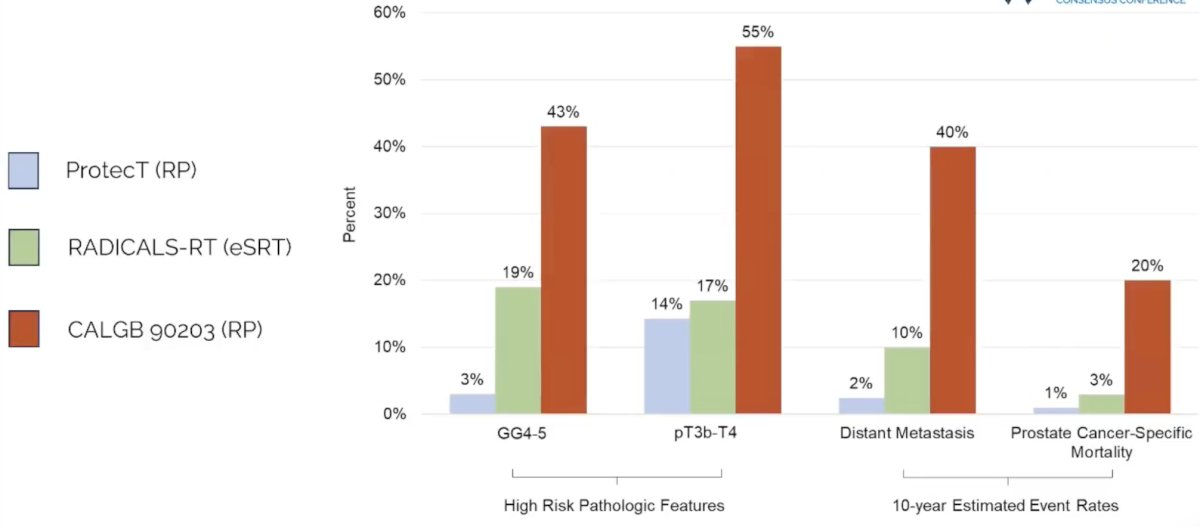
Looking at the ProtecT (radical prostatectomy),2 RADICALS-RT (early salvage radiotherapy),3 and CALGB 90203 (high risk radical prostatectomy),4 he notes that patients enrolled in RADICALS-RT were higher risk than ProtecT, but lower risk than CALGB 90203:
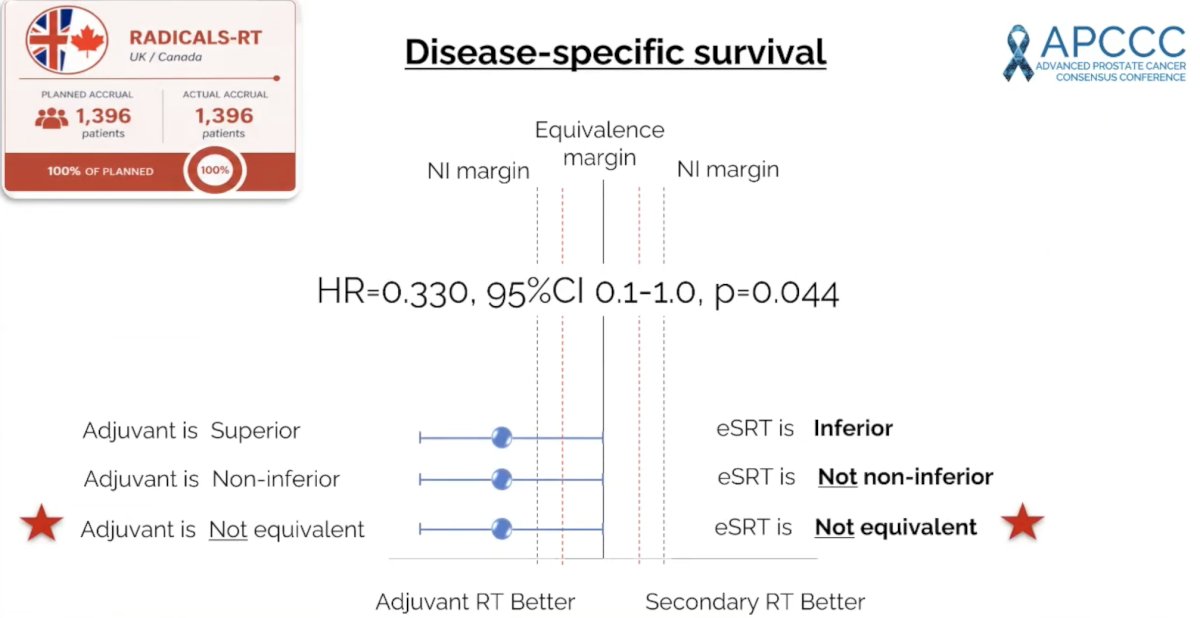
Dr. Spratt also notes that the original primary endpoint in RADICALS-RT was disease specific survival (HR 0.330, 95% CI 0.1-1.0; p = 0.044), favoring adjuvant radiotherapy:
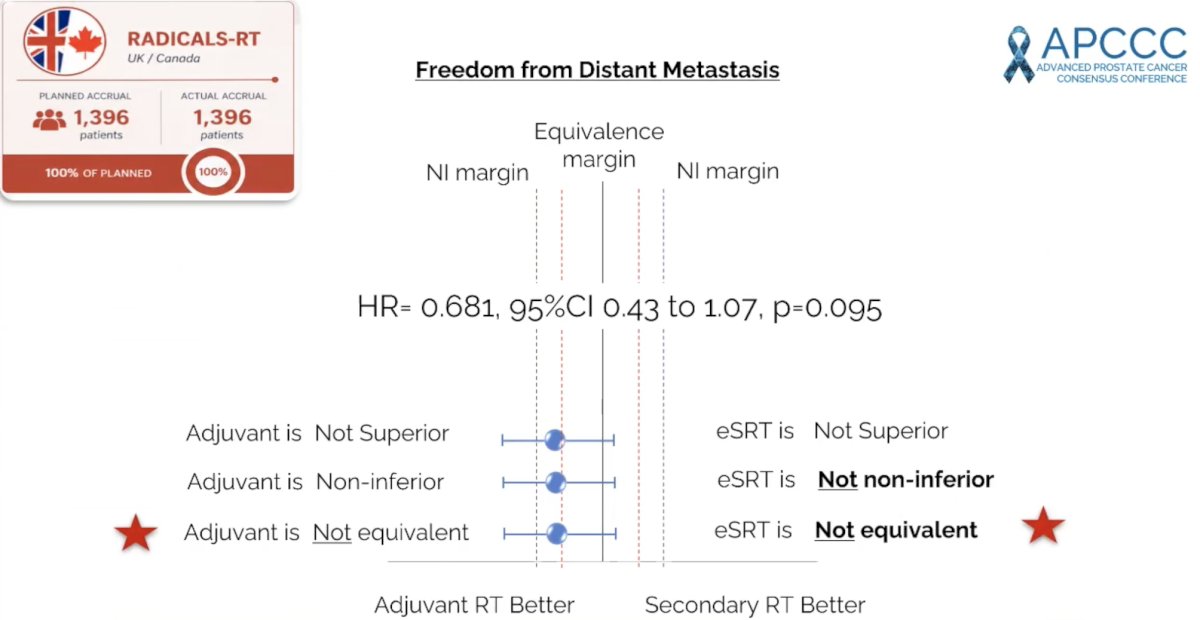
The new primary endpoint was freedom from distant metastasis (HR 0.681, 95% CI 0.43-1.07; p = 0.095), which also favored adjuvant radiotherapy:
Dr. Spratt emphasized that the debate really is for “high risk or locally advanced disease”:
Next, Dr. Spratt provided his second biostatistics crash course explaining the implications for disease specific survival favoring adjuvant radiotherapy (HR 0.330, 95% CI 0.1-1.0; p = 0.044). With a baseline risk of 20% for early salvage radiotherapy, and a new risk of 7.1% with adjuvant radiotherapy, there is no longer a 2% disease specific survival benefit (number needed to treat of 50), but rather a 12.9% benefit and number needed to treat of 7.8. Similarly, Dr. Spratt explained the clinical implications for freedom from distant metastasis, favoring adjuvant radiotherapy (HR 0.681, 95% CI 0.43-1.07; p = 0.095). With a baseline risk of 40% for early salvage radiotherapy, and a new risk of 29.3% with adjuvant radiotherapy, there is no longer a 3% disease specific survival benefit (number needed to treat of 33), but rather a 10.7% benefit and number needed to treat of 9.3.
Dr. Spratt concluded his presentation discussing that early salvage radiotherapy is not equivalent to adjuvant radiotherapy in patients with high-risk localized or locally advanced disease, with the following take-home points:
- For low and intermediate risk prostate cancer, many patients did not need a radical prostatectomy in the first place, and early salvage radiotherapy is not non-inferior and not equivalent to adjuvant radiotherapy
- For high risk/N+ prostate cancer, it is unclear why they had a radical prostatectomy in the first place and early salvage radiotherapy has a high probability of being inferior and not equivalent
Presented by: Daniel E. Spratt, MD, University Hospitals Seidman Cancer Center, Case Western Reserve University, Cleveland, OH
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:
- Vale CL, Fisher D, Kneebone A, et al. Adjuvant or early salvage radiotherapy for the treatment of localized and locally advanced prostate cancer: A prospectively planned systematic review and meta-analysis of aggregate data. Lancet 2020 Oct 31;396(10260):1422-1431.
- Hamdy FC, Donovan JL, Lane JA, et al. 10-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer. N Engl J Med 2016;375(15):1415-1424.
- Parker CC, Clarke NW, Cook AD, et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): A randomized, controlled phase 3 trial. Lancet 2020;396(10260):1413-1421.
- Eastham JA, Heller G, Halabi S, et al. Cancer and Leukemia Group B 90203 (Alliance): Radical Prostatectomy with or without Neoadjuvant Chemohormonal Therapy in Localized, High-Risk Prostate Cancer. J Clin Oncol. 2020 Sep 10;38(26):3042-3050.