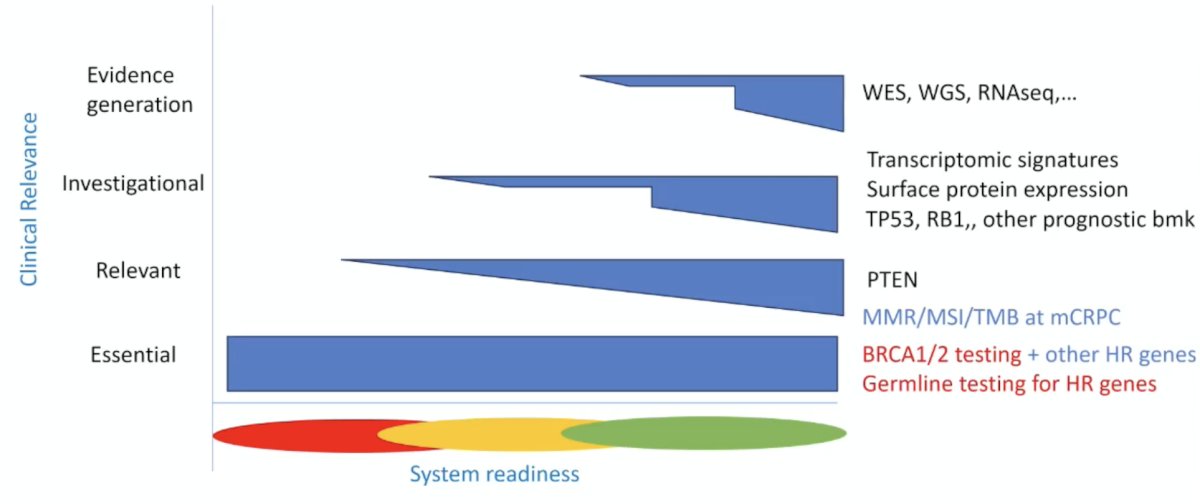
(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management of metastatic hormone sensitive prostate cancer (mHSPC) session and a presentation by Dr. Joaquin Mateo discussing how to test for relevant molecular alterations in mHSPC. When discussing molecular testing in a patient with mHSPC, it important to understand how relevant the biomarker is:
- Essential: linked to an action (drug) that improves patient outcome
- Relevant: linked to an action with moderate or no definitive benefit
- Investigational: prioritization of clinical trials
- Evidence generation: research objective, no direct actionability for individual patient
Based on the aforementioned criteria, Dr. Mateo provided the current outline based on the available molecular tests:
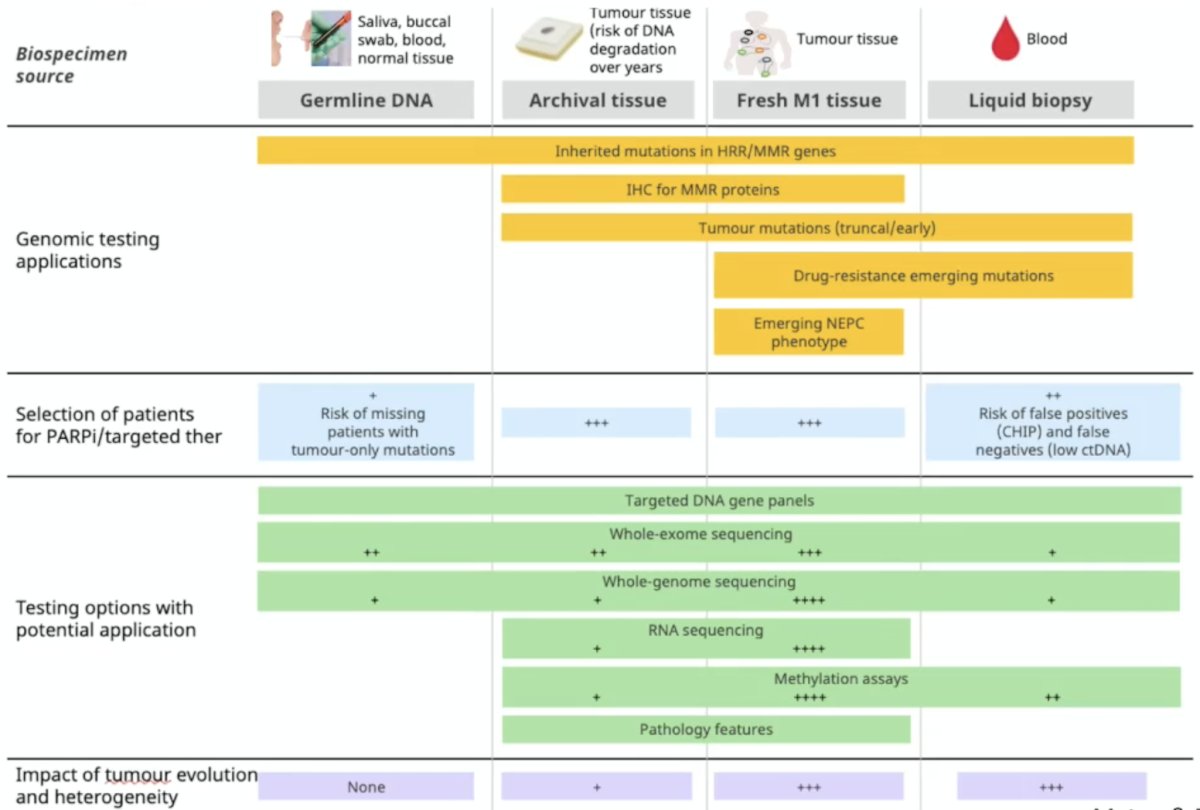
Additionally, as follows is the framework for genomic testing applications, selection of patients for PARP inhibitors, testing options with a potential application, and the impact of tumor evolution and heterogeneity:
Molecular testing in a patient with mHSPC has differences compared to implementation in mCRPC:
- Tissue acquisition and testing and closer in time for patients with de novo mHSPC
- Very old archival tissue fails more often for NGS
- Opportunity to standardize testing at diagnosis
- Opportunity to pair somatic and germline testing
- Tumor evolution is less relevant in mHSPC: no need to repeat biopsies to study biology changes
- ctDNA yield may be low in low-volume and metachronous mHSPC: higher risk of false negative liquid biopsies in cases with low tumor burden or if treatment has already been initiated
- ctDNA yield decreases rapidly upon start of ADT: ctDNA as a measure of disease burden and response biomarker that can complement established markers
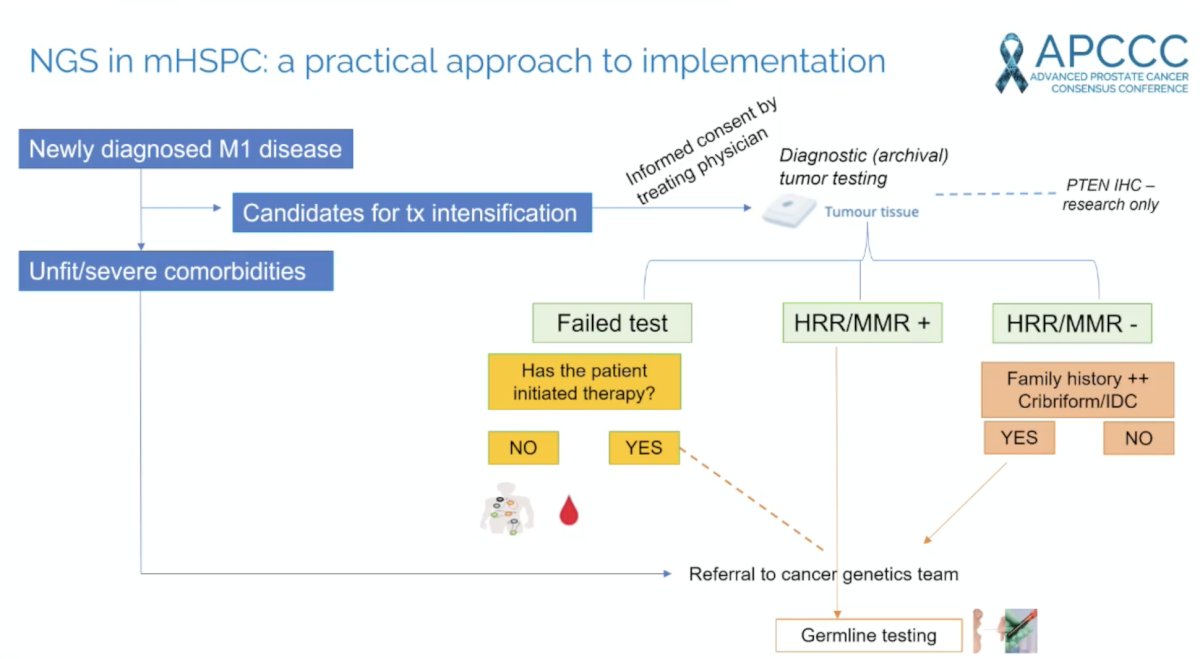
Dr. Mateo also provided a practical approach to implementation of next generation sequencing in mHSPC:
Testing for tumor suppressor genes in mHSPC should include alterations in TP53, RB1, and/or PTEN, which are prognostic in mHSPC and mCRPC. Several questions remain:
- Could this information help in treatment intensity modulation decisions for mHSPC?
- Could this information guide selection of targeted therapies in mHSPC?
In 2025, Grist et al.1 reported that the Decipher RNA signature was both prognostic and predicted survival benefit from docetaxel for metastatic prostate cancer (biomarker-docetaxel interaction p = 0.039). Additionally, transcriptome-based classification of PTEN inactivation identified tumors more likely to have PTEN protein loss (p < 0.001) and metabolically perturbed metastatic prostate cancer that had shorter survival with hormone therapies (p < 0.001), but exhibited docetaxel sensitivity (biomarker-docetaxel interaction p = 0.002).
Other approaches to phenotype biomarkers on the horizon: (i) integrated clinico-biological nomograms, (ii) added value of digital pathology models beyond Gleason, (iii) integrating ctDNA quantitative measures in prognostic and response assessments, and (iv) early evaluation of tumor response to guide adaptive therapies (PSA, ctDNA, re-biospy).
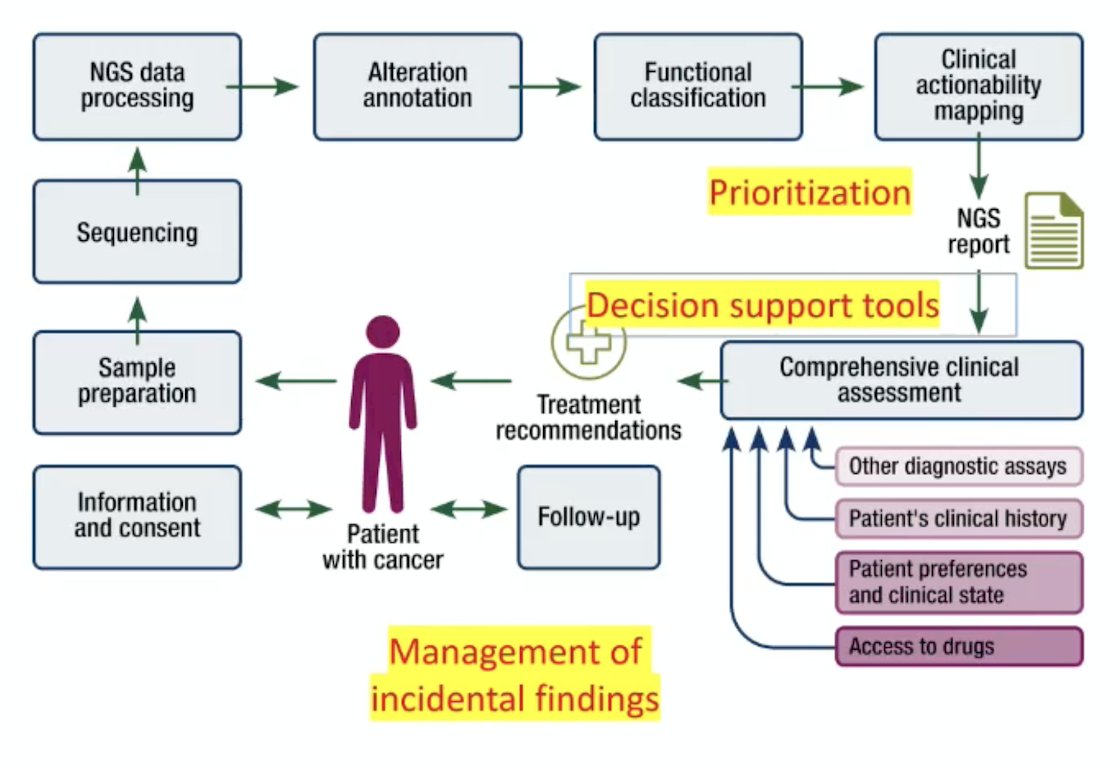
We must make the most out of molecular testing for our patients, summarizing the next generation sequencing data for clinical decision making. Data must be accurate, concise, reproducible, and clinically evidence based. Genomic reports should serve the clinical decision making process:
Dr. Mateo concluded his presentation discussing how to test for relevant molecular alterations in mHSPC with the following take-home points:
- All patients with mHSPC who are candidates for treatment intensification should be considered at least for HRR genes next generation sequencing testing – clinical actionability
- All patients with mHSPC should be considered for germline mutation testing (can be covered with tumor testing in some/many cases?) – pragmatic approach, local solutions
- Consider bringing other mCRPC tests to mHSPC (expanded HRR genes, MMR, prognostic biomarkers) if feasible based on accessibility, system readiness, and cost to benefit balance
- The proximity between diagnostic and testing in mHSPC brings an opportunity for standardizing testing procedures and patient journey (multidisciplinary work)
- A potential model: comprehensive molecular characterization as part of diagnostic evaluations, followed by ad hoc biomarkers at mCRPC with ctDNA or new biopsies as clinical data emerges
Presented by: Joaquin Mateo, MD, PhD, Vall d’Hebron Institute of Oncology, Barcelona, Spain
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References: