(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management of metastatic castration-resistant prostate cancer (mCRPC) session and a presentation by Dr. Thomas Zilli discussing oligometastatic CRPC and the evidence for stereotactic body radiotherapy.
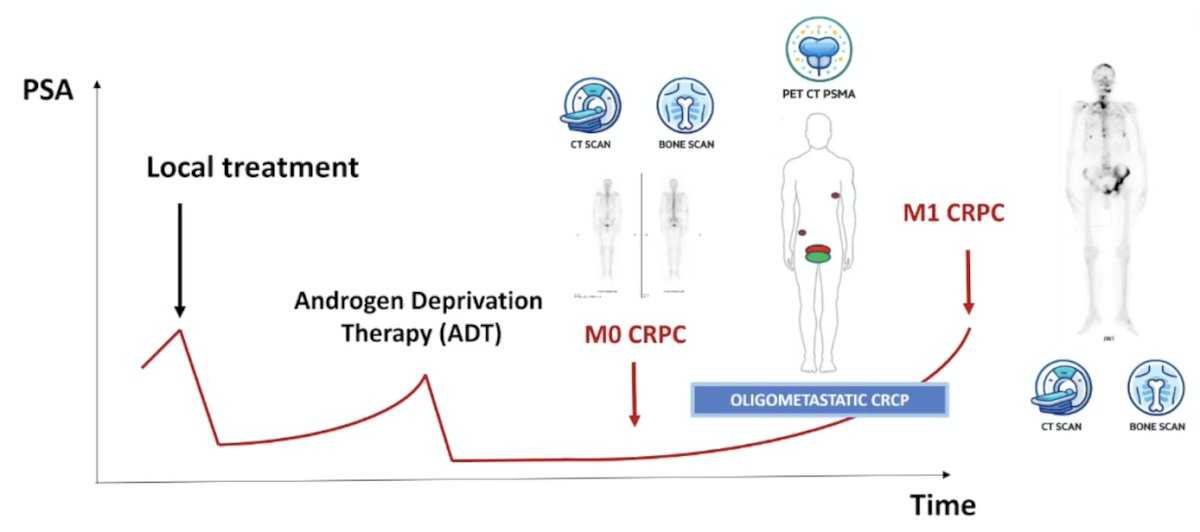
Dr. Zilli started his presentation by highlighting the evolving spectrum of CRPC disease:
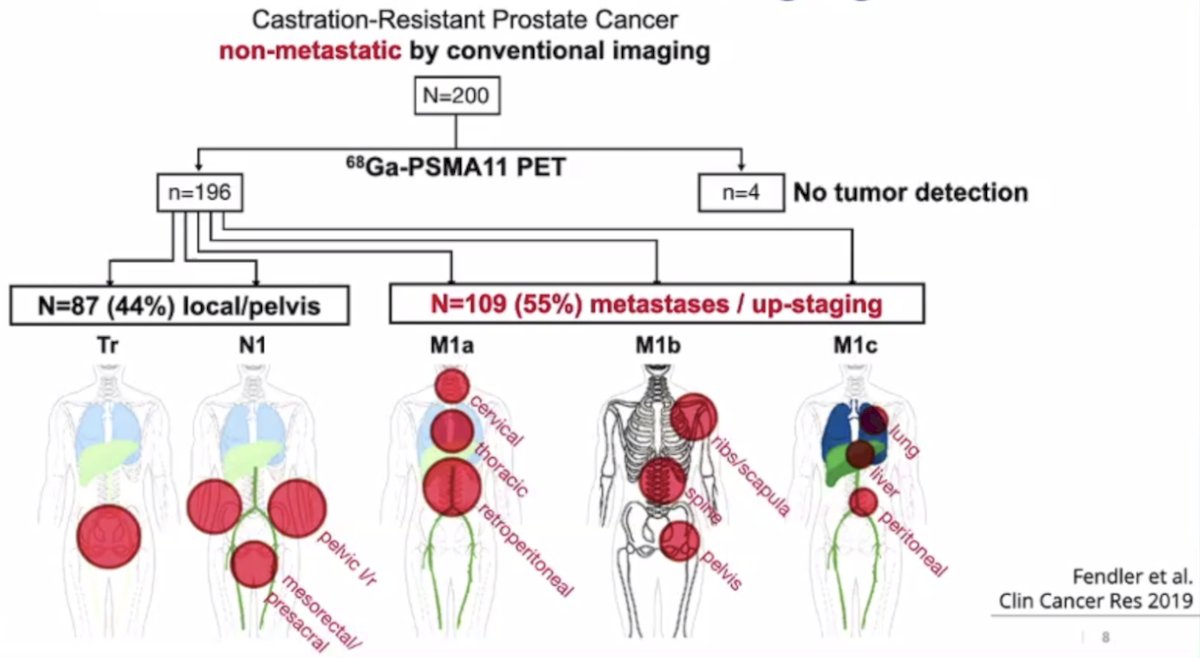
In a study from Fendler et al.,1 they conducted a retrospective analysis from six centers of 200 patients with nmCRPC, PSA >2 ng/ml, and high risk for metastatic disease (PSA doubling time ≤ 10 months and/or Gleason Score ≥8). PSMA PET/CTs were centrally reviewed to assess the PSMA-PET detection rate for pelvic disease and distant metastasis. PSMA PET/CT was positive in 196 of 200 patients. Overall, 44% had pelvic diseases, including 24% with local prostate bed recurrence, and 55% had M1 disease despite negative conventional imaging. Significant predictors of M1 disease included: PSA ≥ 5.5 ng/mL, locoregional nodal involvement determined by pathology (pN1), prior primary radiation, and prior salvage radiotherapy. The interobserver agreement was very high (κ= 0.81 – 0.91):
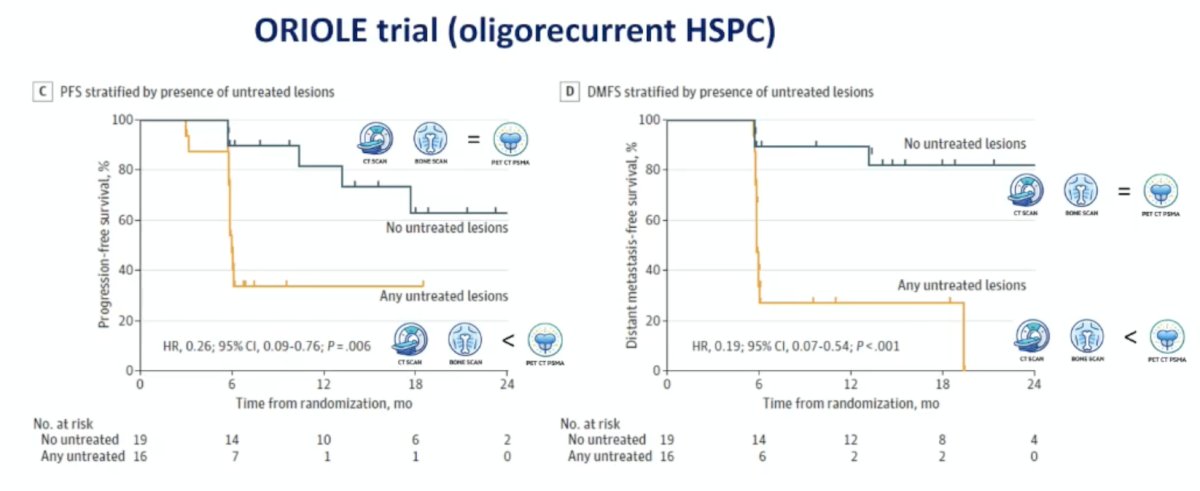
Does PSMA PET imaging make a difference? In the ORIOLE trial,2 all patients received conventional imaging, and PSMA PET/CT, and physicians were blinded to the PSMA result. In the following Kaplan-Meier curves for composite progression-free survival (HR 0.26, 95% CI 0.09-0.76) and distant metastasis-free survival (HR 0.19, 95% CI 0.07-0.54), no untreated lesions had significantly improved outcomes compared to any untreated lesions:
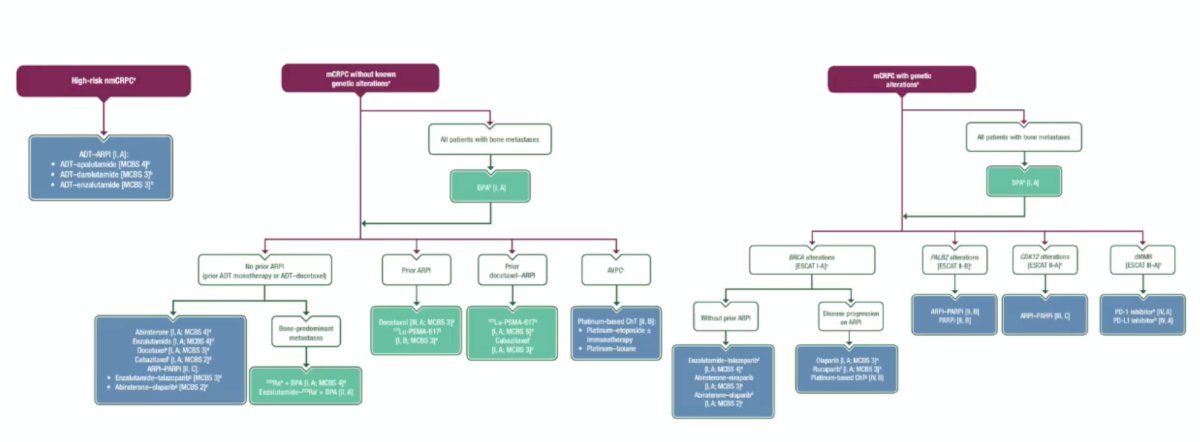
For CRPC disease, systemic therapy remains the cornerstone of treatment:
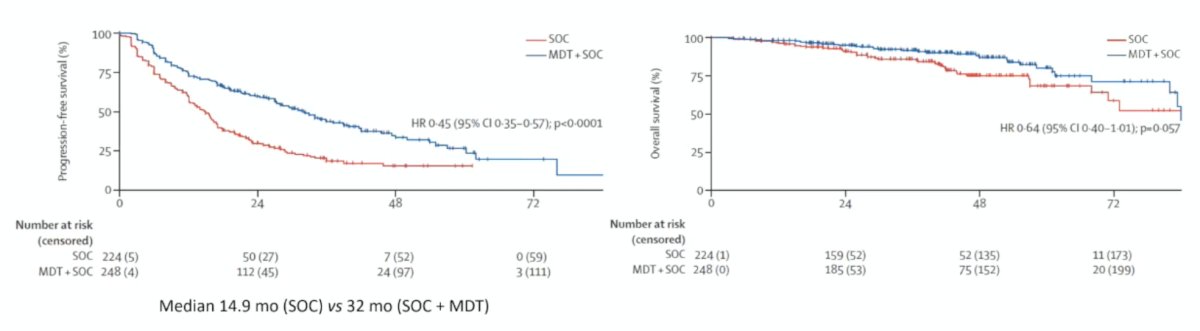
Should we believe in metastasis-directed therapy? The WOLVERINE meta-analysis was published in early 2026 [3] and amalgamated individual patient data across trials to evaluate the effectiveness of metastasis-directed therapy for oligometastatic prostate cancer. Overall, 7 phase 2 trials (n = 574) were included in the analysis. There were 6 trials randomly assigning 472 patients to metastasis-directed therapy + standard of care (n = 248) versus standard of care (n = 224) used to evaluate metastasis-directed therapy, and had a median follow-up time of 40.7 months (IQR 25.6-53.7). Metastasis directed therapy was associated with improved progression free survival (trial level HR 0.44, 95% CI 0.35-0.56, p < 0.0001; patient level HR 0.45, 95% CI 0.35-0.57, p < 0.0001), radiographic progression free survival (trial level HR 0.60, 95% CI 0.42-0.85, p = 0.0039; patient level HR 0.59, 95% CI 0.46-0.76, p < 0.0001), and castration resistance free survival (trial level HR 0.58, 95% CI 0.37-0.92, p = 0.019; patient level HR 0.58, 95% CI 0.37-0.91, p = 0.017). The association between metastasis-directed therapy and overall survival showed an HR of 0.63 (95% CI 0.39-1.00, p = 0.051) in trial-level analyses and 0.64 (95% CI 0.40-1.01, p = 0.057) in patient-level analyses:
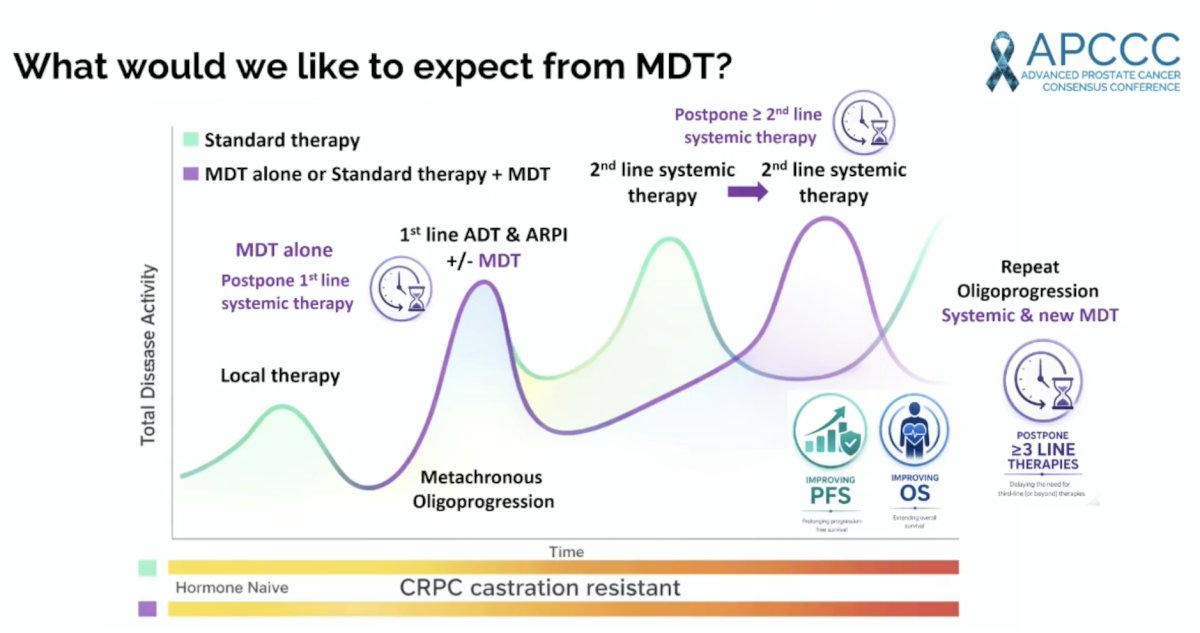
Dr. Zilli also highlighted what he would like to expect from metastasis-directed therapy:
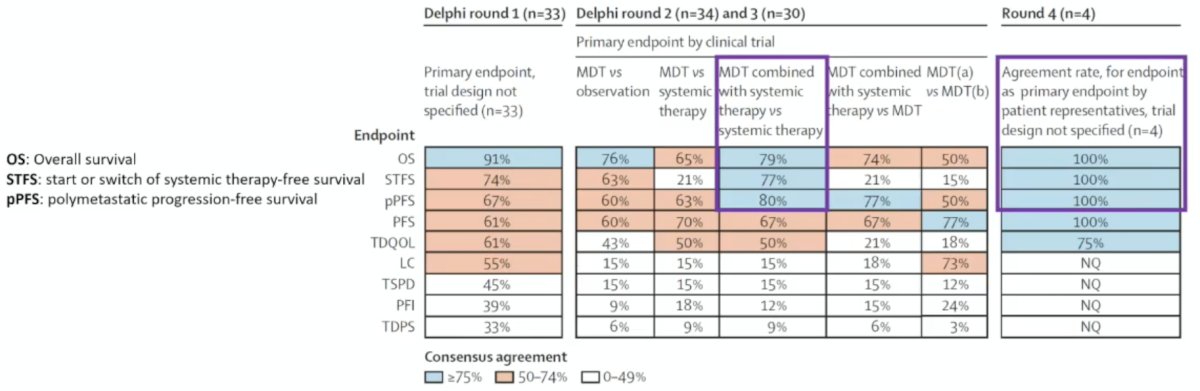
The EORTC-ESTRO OligoCare consortium recently published a report highlighting the results of a Delphi consensus addressing clinical trial endpoints for metastasis-directed therapy in oligometastatic cancer.4 This consensus supported overall survival as a primary endpoint and, in addition to progression-free survival, recommends polymetastatic progression-free survival and systemic therapy-free survival, especially in combination with systemic therapies:
Next, Dr. Zilli noted the different disease settings of oligometastatic CRPC:
- Metachronous oligoprogression: CRPC 1st line
- Induced oligoprogression: CRPC 1st line or >= 2nd line
- Repeat oligoprogression: CRPC >= 2nd line

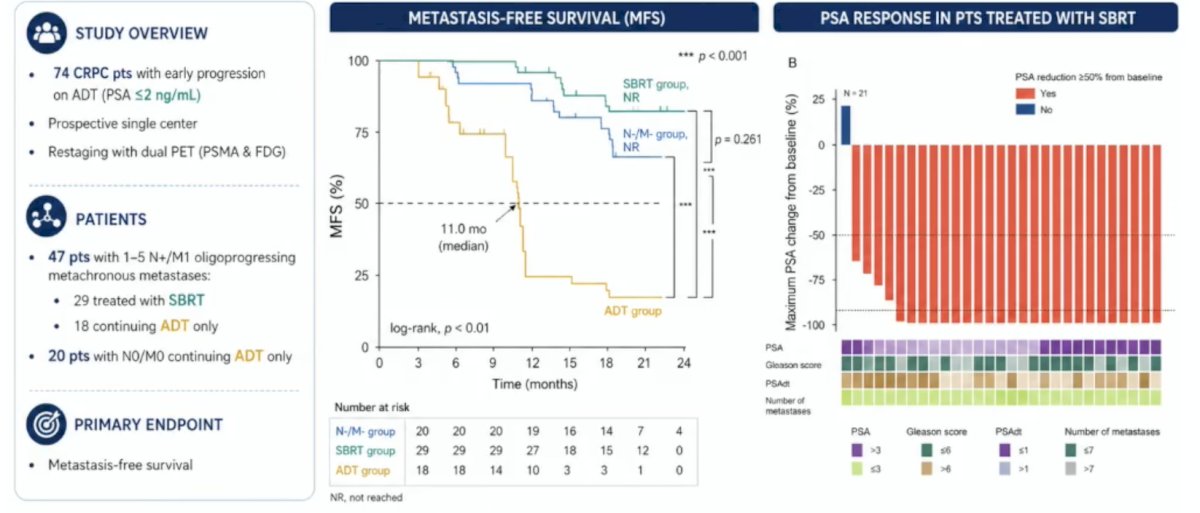
Dr. Zilli then discussed the current available literature in the three aforementioned disease states. A 2022 non-randomized, comparative phase II trial prospectively enrolled patients with nmCRPC on conventional imaging and early PSA progression on ADT (PSA ≤ 2 ng/ml).5 Patients were prospectively screened using a dual-tracer PET/CT (68Ga-PSMA and 18F-FDG). Stereotactic body radiotherapy to all PET-visible lesions, with continuation of ADT, was recommended for patients with ≤5 non-visceral metastases. The median PSA and PSA doubling time were 0.6 ng/ml and 4.6 months, respectively. Overall, 54 patients had metastases, and 17/54 (32%) had PET-discordant PSMA-/FDG+ disease. With the use of dual tracers for staging, PSA response >90% was achieved by 86% of the patients receiving stereotactic body radiotherapy. Notably, patients receiving stereotactic body radiotherapy had superior metastasis-free survival, compared to patients continuing ADT (11 versus 4.7 months, p < 0.001):
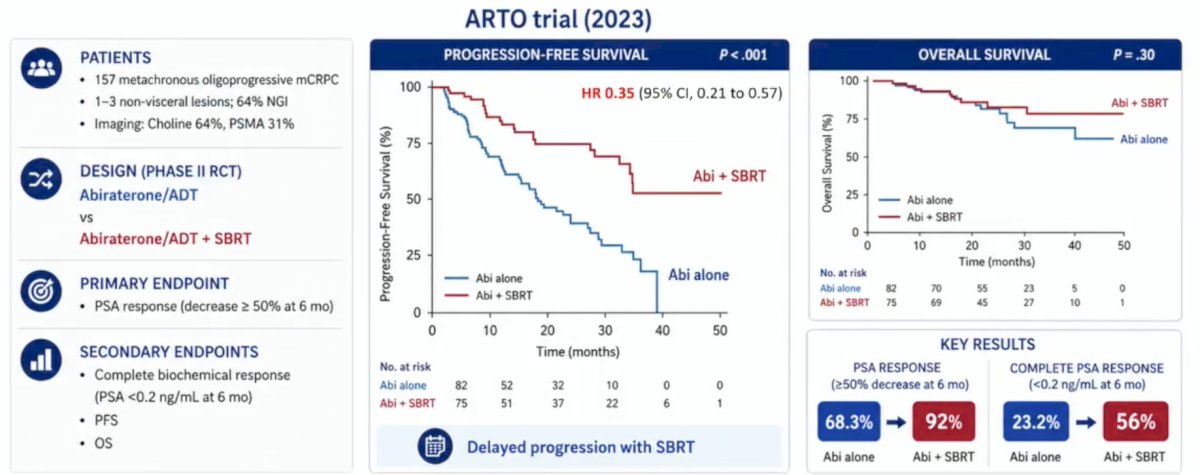
The ARTO trial was a multicenter phase II trial that randomized 157 men with oligometastatic CRPC receiving abiraterone acetate with prednisone in the first-line setting to either abiraterone acetate with prednisone alone or abiraterone acetate with prednisone + concomitant stereotactic body radiotherapy to all sites of disease. Oligometastasis was defined as ≤3 bone or nodal lesions, as per conventional imaging or PET-CT with choline, fluciclovine, or PSMA staging, per the treating physician's discretion. The primary study endpoint was the 6-month rate of biochemical response, defined as a PSA decrease of ≥50% from baseline. The addition of stereotactic body radiotherapy to abiraterone acetate with prednisone resulted in a significantly improved 6-month biochemical response rate (92% versus 68%; OR: 5.34, 95% CI: 2.1–13.9, p = 0.001). Similarly, patients in the abiraterone acetate with prednisone + stereotactic body radiotherapy arm had superior 6-month complete biochemical response rates (ie, PSA < 0.2 ng/mL): 56% versus 23% (OR: 4.22, p < 0.001). After a median follow-up of 25 months, patients in the abiraterone acetate with prednisone + stereotactic body radiotherapy arm had a superior progression-free survival rate (median: not reached versus 17 months, respectively; HR 0.35, 95% CI 0.21-0.57, p < 0.001). The median overall survival at the time of this data analysis was not yet reached in either arm (HR 0.65, 95% CI 0.28–1.49):
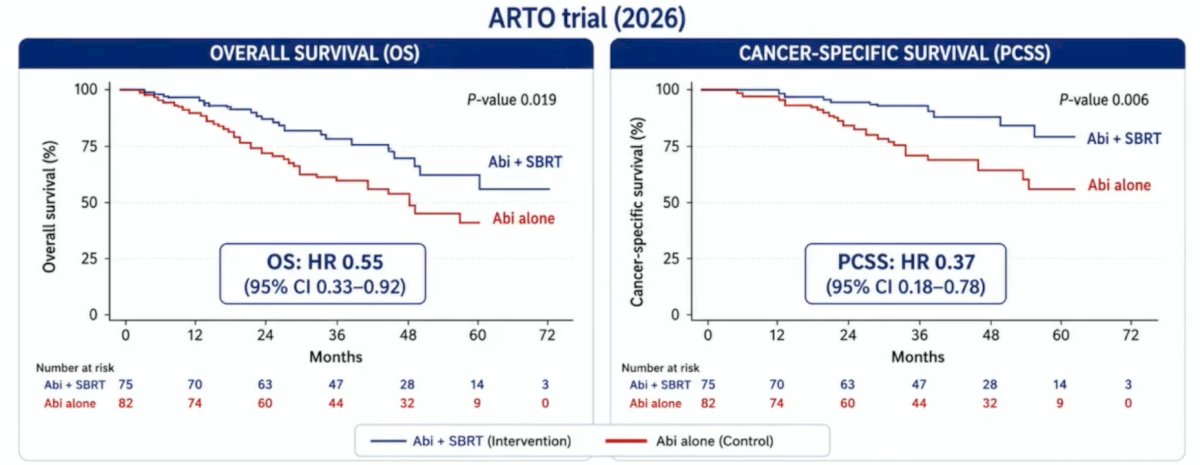
A 2026 update of the ARTO trial presented at ASCO GU 2026 confirmed that stereotactic body radiotherapy in first-line CRPC with next-generation imaging also improves overall survival. At a median follow-up of 53 months (IQR 43–60), previously reported benefits in biochemical progression-free survival and radiographic progression-free survival were confirmed in favor of the experimental arm:
- Biochemical progression-free survival: HR 0.49 (95% CI 0.33–0.73)
- Radiographic progression-free survival: HR 0.48 (95% CI 0.32–0.72)
Importantly, significant survival benefits were also observed:
- Overall survival: HR 0.55 (95% CI 0.33–0.92)
- Prostate cancer specific survival: HR 0.37 (95% CI 0.18–0.78)
These hazard ratios indicate a 45% relative reduction in risk of death overall and a 63% relative reduction in prostate cancer–specific mortality with the addition of stereotactic body radiotherapy:
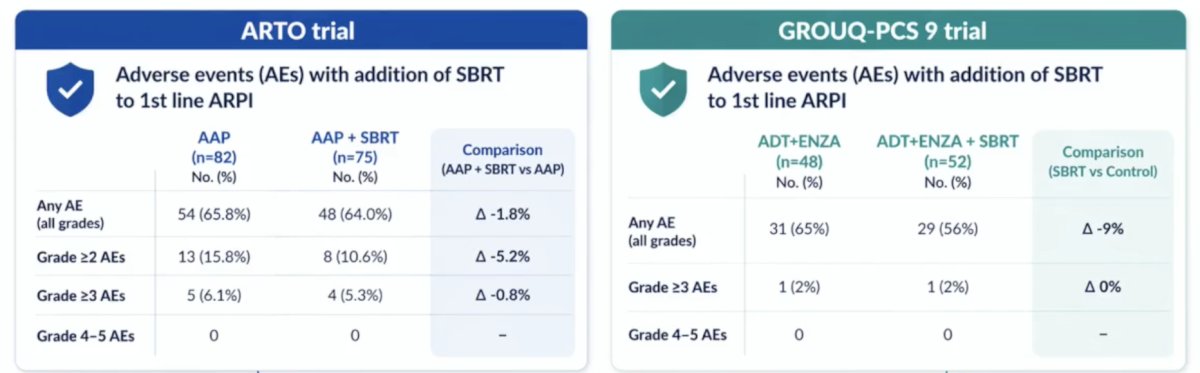
The GROUQ-PCS 9 trial7 is a phase II randomized trial of enzalutamide + stereotactic body radiotherapy versus enzalutamide alone. The median radiographic progression-free survival was 4.6 years versus 2.3 years (HR 0.48, 95% CI 0.27-0.86) for enzalutamide + stereotactic body radiotherapy. Additionally, there was a benefit in time to subsequent therapy (5.1 years versus 2.9 years; HR 0.42, 95% CI 0.22-0.80):

Importantly, stereotactic body radiotherapy is well tolerated in first-line CRPC and is not associated with an increase in adverse events. The following data highlights adverse events in the ARTO and GROUQ-PCS 9 trials:
In second-line or later CRPC, stereotactic body radiotherapy may improve progression-free survival. The TRAP trial8 is a phase II prospective trial of stereotactic body radiotherapy to progressing sites on ADT + androgen receptor pathway inhibitor. The median progression-free survival was 6.4 months, which was also associated with a delayed time to next line of therapy (median 27 months, 95% CI 14.9-24.6) and was accompanied by an acceptable safety profile:
![In second-line or later CRPC, stereotactic body radiotherapy may improve progression-free survival. The TRAP trial [8] is a phase II prospective trial of stereotactic body radiotherapy to progressing sites on ADT + androgen receptor pathway inhibitor. The median progression-free survival was 6.4 months, which was also associated with a delayed time to next line of therapy (median 27 months, 95% CI 14.9-24.6) and was accompanied by an acceptable safety profile:](/images/com-doc-importer/262-apccc-2026/apccc-2026-oligometastatic-crpc---what-is-the-evidence-for-sbrt/image-13.jpg)
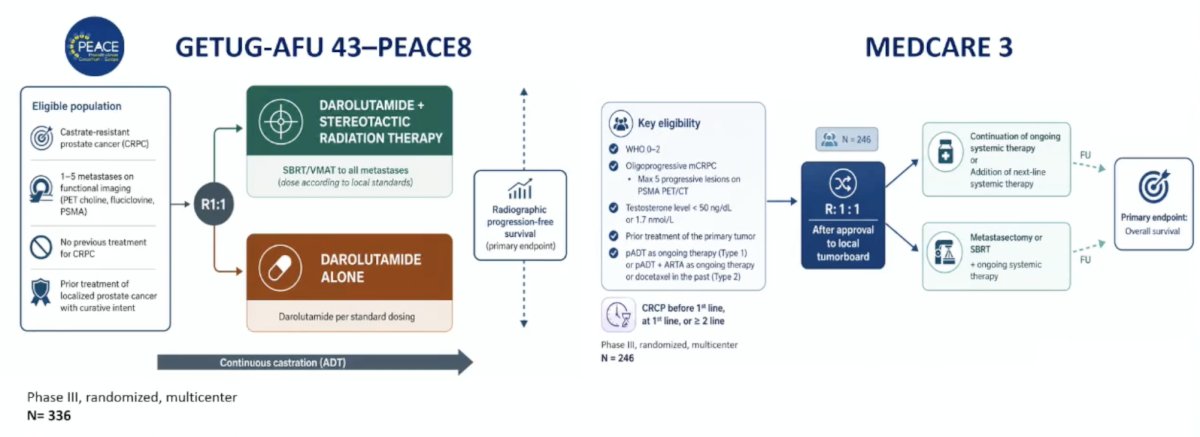
To finish his presentation, Dr. Zilli highlighted several ongoing trials testing metastasis-directed therapy in the CRPC setting. The GETUC-AFU 43-PEACE 8 phase 3 trial is testing darolutamide + stereotactic body radiotherapy versus darolutamide alone, with a primary endpoint of radiographic progression-free survival, and the MEDCARE 3 phase 3 trial is assessing continuation of ongoing systemic therapy versus metastasectomy or stereotactic body radiotherapy + continuation of ongoing systemic therapy with a primary endpoint of overall survival:
Additional ongoing trials testing metastasis-directed therapy in the CRPC setting are noted in the following table:

Dr. Zilli concluded his presentation discussing oligometastatic CRPC and the evidence for stereotactic body radiotherapy with the following take-home points:
- In metachronous oligoprogressive CRPC, stereotactic body radiotherapy + standard of care systemic therapy may improve progression-free survival, overall survival, and delay further systemic therapy (phase III validation pending)
- Metastasis-directed therapy can be used in first-line CRPC and in further lines for repeat oligoprogression
- Modern imaging and new biomarkers will improve patient selection
- Multidisciplinary discussion is key, as well as prioritizing inclusion in trials and prospective cohorts
Presented by: Thomas Zilli, MD, PD, Radiation Oncologist, Oncology Institute of Southern Switzerland, Bellinzona, Switzerland
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:
- Fendler WP, Weber M, Iravani A, et al. Prostate-Specific Membrane Antigen Ligand Positron Emission Tomography in Men with Nonmetastatic Castration-Resistant Prostate Cancer. Clin Cancer Res. 2019 Dec 15;25(24):7448-7454.
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol 2020 Mar 26;6(5):650-659.
- Tang C, Sherry AD, Hwang H, et al. Metastasis-directed therapy and standard of care versus standard of care for oligometastatic prostate cancer (WOLVERINE): A systematic review and individual patient data meta-analysis from the X-MET collaboration. Lancet Oncol. 2026 Feb;27(2):181-190.
- Widder J, Bol GM, Simek IM, et al. Clinical trial endpoints for metastasis-directed therapy in oligometastatic cancer: A review and Delphi consensus on behalf of the EORTC-ESTRO OligoCare consortium. Lancet Oncol. 2026 May;27(5):e238-247.
- Pan J, Wei Y, Zhang T, et al. Stereotactic radiotherapy for lesions detected via 68Ga-prostate-specific membrane antigen and 18F-fluorodeoxyglucose positron emission tomography/computed tomography in patients with nonmetastatic prostate cancer with early prostate-specific antigen progression on androgen deprivation therapy: a prospective single-center study. Eur Urol Oncol. 2022; 5:420–427.
- Francolini G, Allegra AG, Detti B, et al. Stereotactic body radiation therapy and abiraterone acetate for patients affected by oligometastatic castrate-resistant prostate cancer: A randomized phase II trial (ARTO). J Clin Oncol. 2023 Dec 20;41(36):5561-5568.
- Niazi T, Saad F, Tisseverasinghe S, et al. Metastasis-directed therapy in addition to standard systemic therapy in oligometastatic castration-resistant prostate cancer in Canada (GROUQ-PCS 9): A multicentre, open-label, randomized, phase 2 trial. Lancet Oncol. 2025 Sep;26(9):1158-1167.
- Patel P, Dreibe S, Attard G, et al. Stereotactic body radiation therapy for oligoprogressive disease in androgen-suppressed prostate cancer: Primary endpoint analysis of the TRAP trial. Int J Radiat Oncol Biol Phys. 2026 May 1;125(1):285-294.