(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management of metastatic castration resistant prostate cancer (mCRPC) session and a presentation by Dr. Himisha Beltran discussing treatment options in 2026 for neuroendocrine prostate cancer. Neuroendocrine prostate cancer has a tumor morphology similar to small cell carcinoma, large cell carcinoma, and mixed adenocarcinoma. The IHC markers associated with this entity include:
- Classical: INSM1, SYP, chromogranin A, CD57, NSE
- Low AR, AR signaling (ie, PSA, NXX3.1)
- High Ki67 >60% (proliferation)
The treatment emergence of neuroendocrine prostate cancer occurs after androgen receptor therapies:
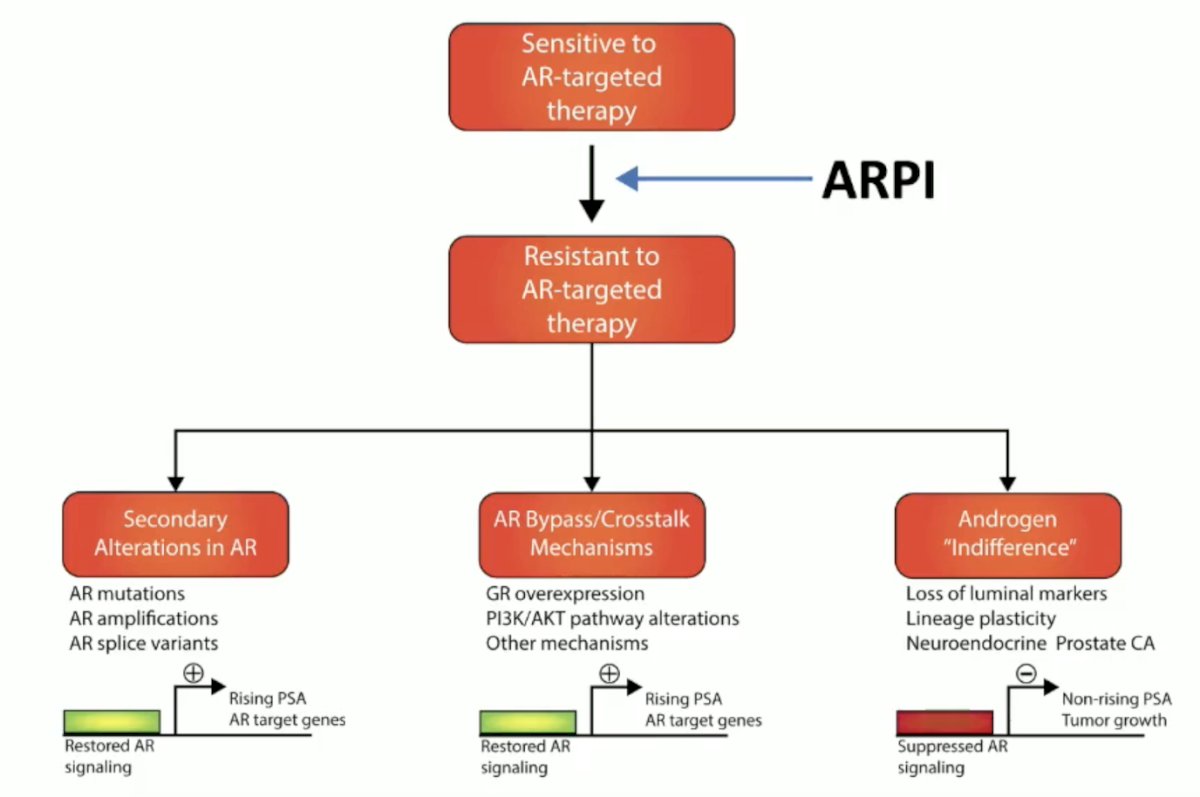
Therapeutic implications include deciding if the patient needs a next-line CRPC therapy or a small-cell directed therapy. This can be informed by pathologic features, such as pure versus mixed, percentage of positive small cell carcinoma, AR expression in tumors, and Ki67 expression. We can also be informed by clinical features, such as aggressiveness, PSA, PSMA, and visceral metastases. Dr. Beltran notes that it is important to continue ADT due to tumor heterogeneity. According to the NCCN guidelines, we should treat neuroendocrine prostate cancer like small-cell lung cancer.
The development landscape for neuroendocrine prostate cancer is robust and has many targets and modalities:
- IO combinations:
- KEYNOTE-365 – Randomized phase 1b of carboplatin and etoposide with or without pembrolizumab (NCT02861573)
- CHAMP – Phase 2 trial of nivolumab, ipilimumab, cabazitaxel, and carboplatin for aggressive variant or neuroendocrine prostate cancer (NCT04709276)
- Phase 2 trial of nivolumab + ipilimumab + cabozantinib for rare genitourinary tumors, including neuroendocrine prostate cancer (NCT03866382)
- BsAbs/T-cell engager ± immunotherapy:
- SKYBRIDGE – Phase 1 trial of peluntamig (PT217) bispecific antibody against DLL3/CD47, including neuroendocrine prostate cancer (NCT05652686)
- DeLLight – Tarlatamab for advanced extra-pulmonary small cell, including neuroendocrine prostate cancer (NCT06893783)
- Phase 2 trial of ZG006, a trispecific T-cell engager targeting DLL3/CD3, for metastatic neuroendocrine prostate cancer (NCT07024277)
- Phase 1/2 trial of HPN328, a trispecific T-cell engager targeting DLL3/CD3, monotherapy, and with atezolizumab in patients with neuroendocrine lung, prostate, and other neuroendocrine carcinomas (NCT04471727)
- Radioligand therapy:
- Phase 1 trial of 177Lu-DTPA-SC16.56 targeting DLL3 for neuroendocrine prostate cancer and neuroendocrine carcinoma of lung (NCT06941480)
- Phase 2 trial of 177Lu-DOTA-TATE for neuroendocrine prostate cancer (NCT05691465)
- Phase 1 trial of 177Lu-PSMA-617, 177Lu-DOTA-TATE, or 177Lu-NeoB to target PSMA, SSTR2, or GRPR, respectively, for metastatic neuroendocrine prostate cancer (NCT06379217)
- Antibody drug conjugates:
- ZL-1310 (DLL3) in participants with selected solid tumors (NCT06885281)
- Sacituzumab tirumotecan + tagitanlimab: Trial for neuroendocrine prostate cancer and Aggressive Variant Prostate Cancer (NCT07179783)
- TKI/Epigenetic:
- Phase 2 trial of ESK981, a multi-kinase and PIKfyve inhibitor, for select solid tumors, including neuroendocrine prostate cancer (NCT05988918)
- Phase 1/2 trial of JBI-802, an LSD1/HDAC inhibitor in advanced solid tumors, including neuroendocrine prostate cancer (NCT05268666)
- Phase 2 trial of MLN8237 (Alisertib), an AURKA inhibitor in mCRPC and neuroendocrine prostate cancer (NCT01799278)
Tarlatamab is an anti-DLL3 HLE BiTE that was previously established in the treatment of small-cell lung cancer. Tarlatamab has been assessed in the DELLpro-300 phase 1b study in neuroendocrine prostate cancer/molecularly-defined advanced variant prostate cancer led by Dr. Aggarwal and colleagues:1
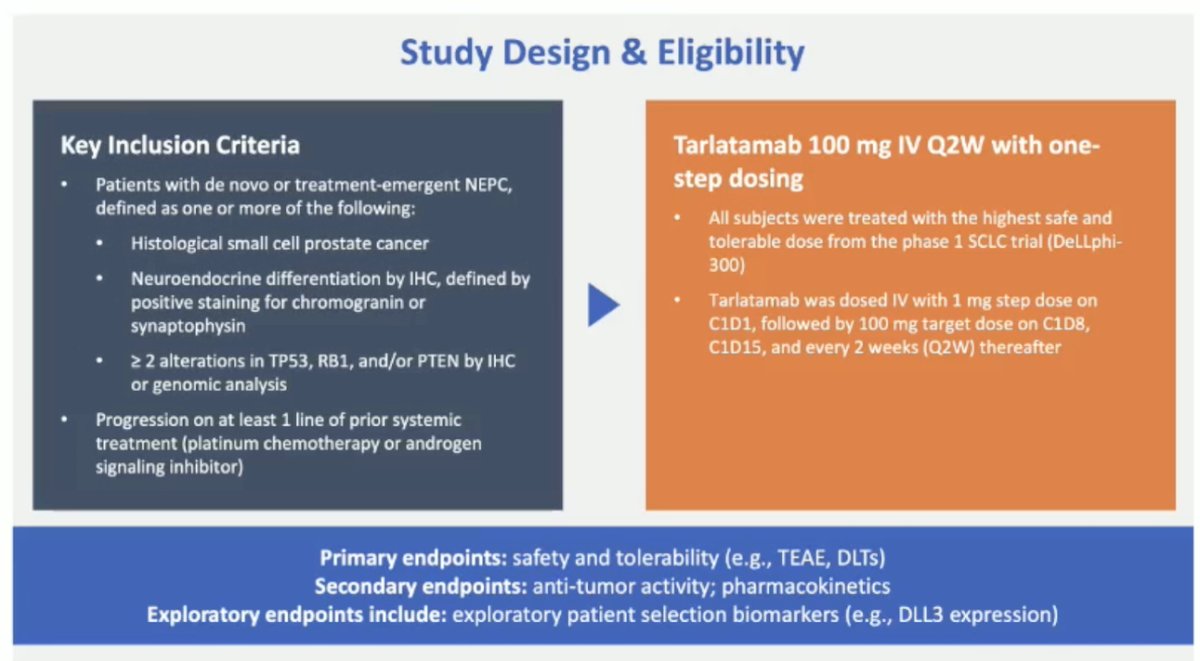
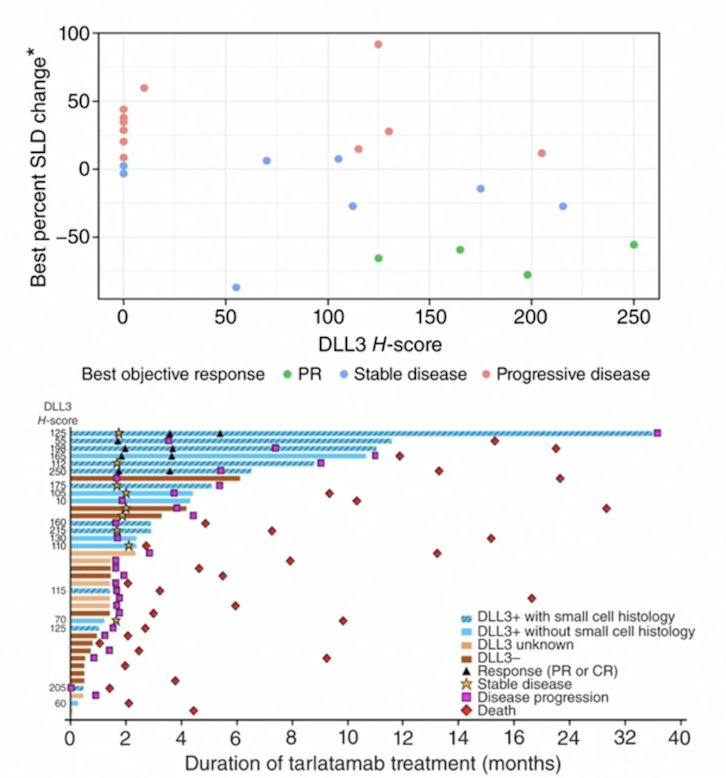
In DELLpro-300, a change in tumor size from baseline correlated with baseline DLL3 H-score, and the objective response rate was 22% in DLL3-positive tumors. Durable responses were observed in a subset of DLL3-positive tumors with small cell histology:
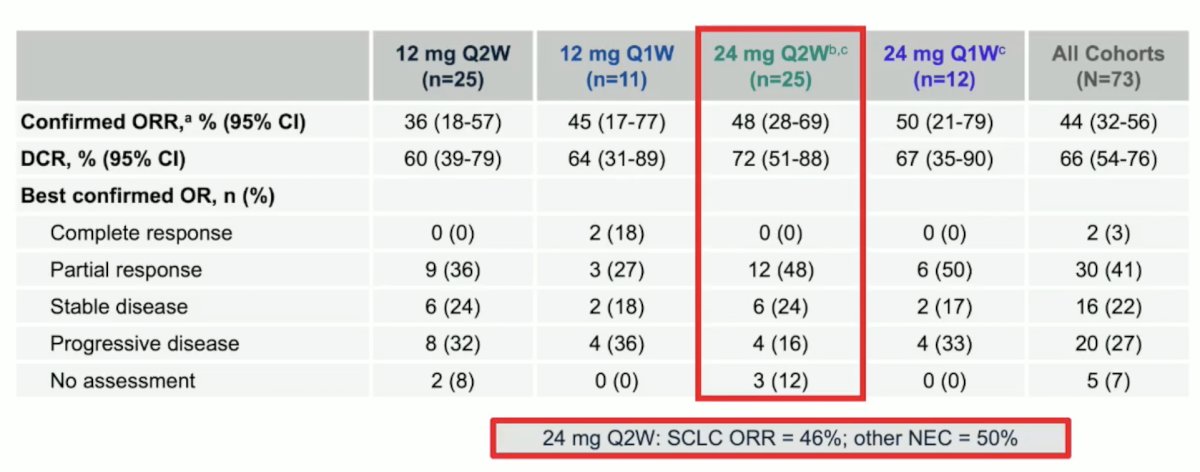
At ESMO 2025, Dr. Beltran presented phase 1/2 data from a trial of MK6070 (gocatamig), a DLL3 T-cell engager. At a dose of 24 mg every 2 weeks (n = 25), the confirmed objective response rate of 48%, the disease control rate was 72%, and 48% of responses were partial responses:
Should we treat neuroendocrine prostate cancer with tarlatamab? Dr. Beltran notes that we should make sure there is confirmed neuroendocrine prostate cancer with morphology and IHC. To do so, we must test for DLL3. Dr. Beltran also highlighted keys to administering DLL3-targeted T-cell engagers:
- 10 mg IV every 2 weeks (approved dose tarlatamab) – with dexamethasone pre-medication
- Day 1 (priming dose)– 1 mg IV: hospital admission x 48 hours
- Day 8 (target dose)– 10 mg IV: hospital admission x 48 hours
- Cytokine release syndrome is the most common adverse event (50-60%)
- Highest risk during the first doses (priming, target), usually grade 1-2 and reversible in 24-48 hours
- Associated with fever, hypotension, hypoxia, and tachycardia
- Treatment includes: steroids, tocilizumab (anti-IL-6) (for ≥grade 2)
- Neurotoxicity (ICANS) – is less common (DELLphi-301 trial- 5-10%, grade ≥3 was 1-2%)
- ICE score + neuro checks
- Can be later after cycle 2
- Treatment steroids (for ≥grade 2)
What are the other options to consider if there is no clinical trial? We can consider CRPC therapy, but we must consider the clinical context. Re-treatment with platinum chemotherapy is also an option, but we must consider how long ago the prior therapy was. Other therapies include lurbinectedin and topotecan.
Lurbinectedin is a synthetic alkaloid and DNA alkylating chemotherapy approved for small-cell lung cancer. In 2024, Meyer and colleagues2 retrospectively reported their use of lurbinectedin for the treatment of neuroendocrine prostate cancer. Among 18 patients, the median number of prior systemic therapies was 4 (range: 2-7), and the median number of lurbinectedin cycles completed was 5 (range: 1-10). The clinical benefit rate was 56%, with the most common treatment-related adverse events being fatigue and anemia. The median overall survival was 6.01 months (95% CI 0.23-16.69), and median progression-free survival was 3.35 months (95% CI 0.16-7.79).
Other potential targets and trials include B7-H3 expressed CRPC and neuroendocrine prostate cancer, SEZ6, co-targeting adenocarcinoma + neuroendocrine lineage, and epigenetic therapies to target lineage plasticity.
Finally, Dr. Beltran highlighted de novo versus treatment-emergent neuroendocrine prostate cancer:
- “De novo” small cell/neuroendocrine prostate cancer has similar pathologic and molecular features to treatment-emergent neuroendocrine prostate cancer and can be heterogeneous
- Pure small cell carcinoma versus “mixed” adenocarcinoma/neuroendocrine features
- Similar prostate genomic aberrations (including T2-ERG)
- Some patients with mHSPC present with “neuroendocrine features,” but are AR positive, PSA is high, and PSMA is positive
- Currently managed like HSPC
- Should we monitor more closely with scans? Should we repeat the biopsy at the progression of the disease?
- Treatment considerations?
- Triplet or quadruplet therapy? ADT, androgen receptor pathway inhibitor, docetaxel, carboplatin
- The CaBRA trial (PEACE-6) (PI: Dr. Alice Bernard-Tessier)
Dr. Beltran concluded her presentation discussing treatment options in 2026 for neuroendocrine prostate cancer with the following take-home points:
- Neuroendocrine prostate cancer is a heterogeneous disease – treatment should be tailored to clinical and pathologic features
- Platinum chemotherapy and small-cell lung cancer regimens could be considered based on guidelines
- DLL3 is very specific to neuroendocrine carcinomas – careful patient selection for tarlatamab and other emerging DLL3-therapies is critical (not enough to have TP53/RB1/PTEN)
- Other potential targets in clinical trials: cell surface (eg, SEZ6, B7H3), epigenetic (ie, EZH2), rational combination strategies
Presented by: Himisha Beltran, MD, Medical Oncologist, Dana Farber Cancer Institute, Associate Professor of Medicine, Harvard Medical School, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
- Aggarwal R, Rottey S, Bernard-Tessier A, et al. Safety and efficacy of tarlatamab in patients with neuroendocrine prostate cancer: Results from the phase 1b DeLLpro-300 study. Clin Cancer Res. 2025 Sep 15;31(18):3854-3863.
- Meyer H, Sunakra R, Rothmann E, et al. The use of lurbinectedin for the treatment of small-cell and neuroendocrine carcinoma of the prostate. Clin Genitourin Cancer. 2024 Oct;22(5):102172.