(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management of metastatic castration resistant prostate cancer (mCRPC) session and a presentation by Dr. Emmanuel Antonarakis discussing whether there are patients with mCRPC who may benefit from immunotherapy.
In unselected patients with mCRPC, it is established that immune checkpoint inhibitors are ineffective, with a pooled objective response rate of <5% (n = 4,680):

Dr. Antonarakis notes that there are many potential molecular markers to assess immune checkpoint inhibitor response, including: dMMR/MSI-high, TMB-high (>= 10 mut/Mb), HRR mutations, CKD12 mutations, frameshift mutations, certain TP53 mutations, POLE, POLD1 mutations, AR-V7 detection, and PD-L1 protein expression. However, to date, the only two key molecular markers are dMMR/MSI-high and TMB-high (>= 10 mut/Mb). MMRd is found in many cancers, but unfortunately, it is only present in ~2.5% of prostate cancers:

In a study of 1,033 mCRPC patients,1 only 32 (3.1%) had MSI-high or MSI-intermediate scores:

In a study assessing dMMR CRPC and immune checkpoint inhibitors, frameshift mutations had a greater response to anti-PD1 therapy than missense mutations:

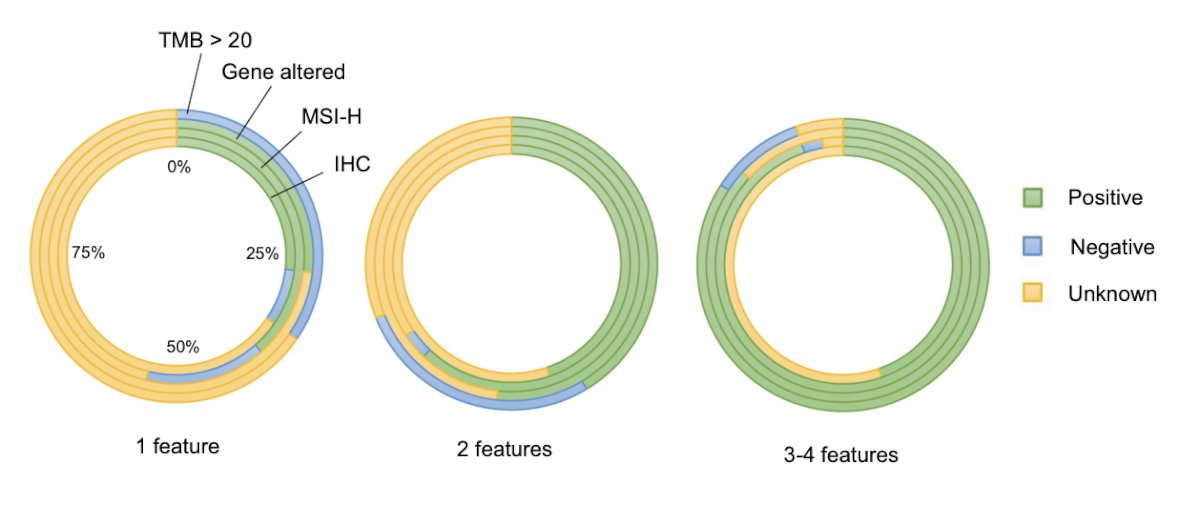
In 2025, van Wilpe et al.2 assessed the efficacy of immune checkpoint inhibitors in dMMR mCRPC among 93 patients starting anti-PD-(L)1 treatment. The cohort was split into subgroups according to the number of dMMR-associated features. These features include:
- Loss of MMR protein expression on IHC
- A somatic or germline pathogenic or likely pathogenic alteration in one of the MMR genes
- Microsatellite instability according to polymerase chain reaction analysis or next-generation sequencing (MSI-H)
- A nonsynonymous TMB >20 mutations/Mb
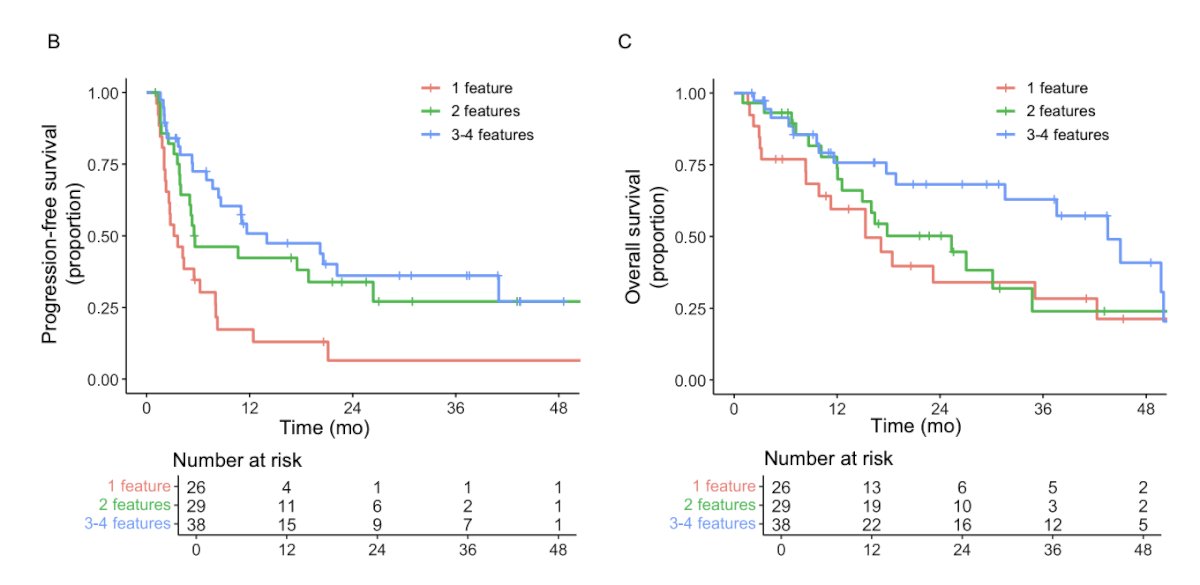
Progression-free survival was significantly longer for the group with dMMR consensus on two or more tests than for the group with only one positive test (2 tests: HR 0.47, 95% CI 0.25–0.86; p = 0.015; 3 tests: HR 0.36, 95% CI 0.20–0.65; p < 0.001). In addition, overall survival was longer for the group with dMMR consensus on three or more tests than for the group with only one positive test (HR 0.50, 95% CI 0.28–0.89; p = 0.019):
Objective response rates and PSA responses also appeared to be favorable in patients with a higher number of positive tests:

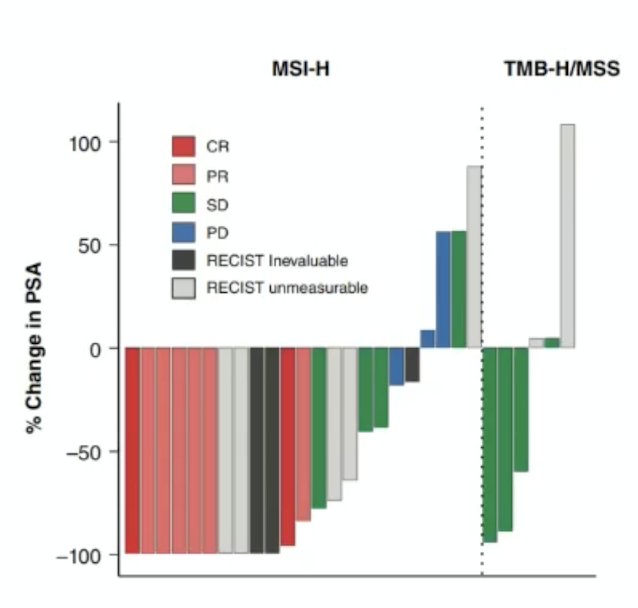
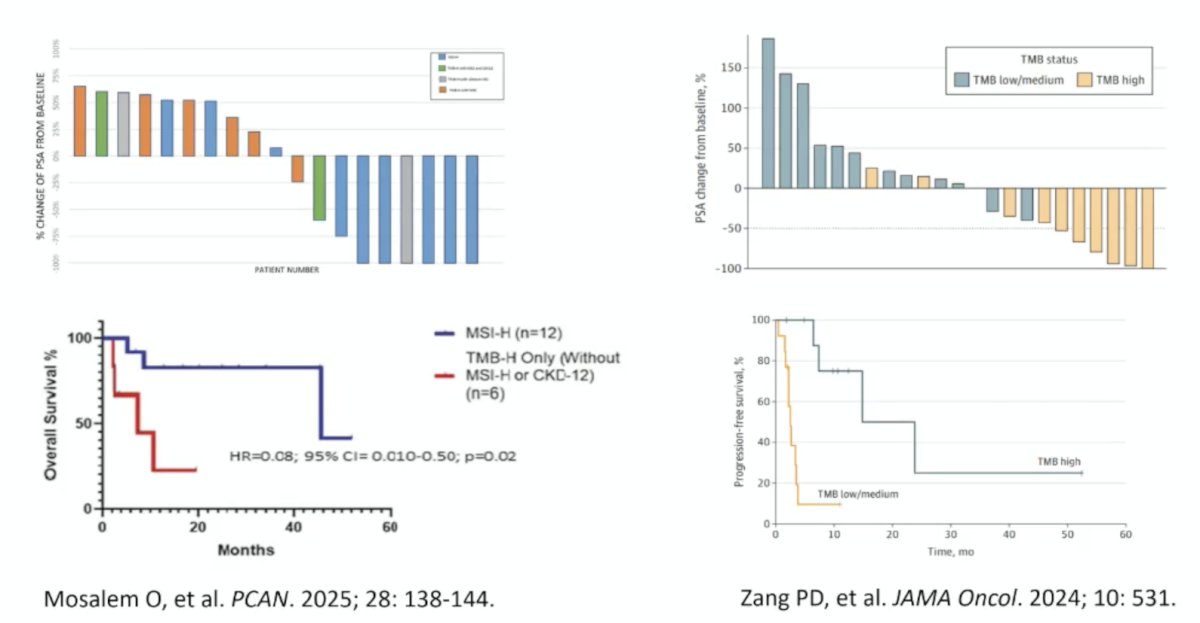
Is MSI-high or TMB-high more important for selecting mCRPC patients? To address this question, Lenis et al.3 assessed 66 men who had MSI-H/dMMR, and 33 who had TMB-H/MSS prostate cancers. Overall, 27 patients with MSI-H/dMMR and 8 patients with TMB-H/MSS tumors received immune checkpoint blockade, of which 45% of patients with MSI-H/dMMR had a RECIST response, and 65% had a PSA50 response. No patient with TMB-H/MSS had a RECIST response, and 50% had a PSA50 response:
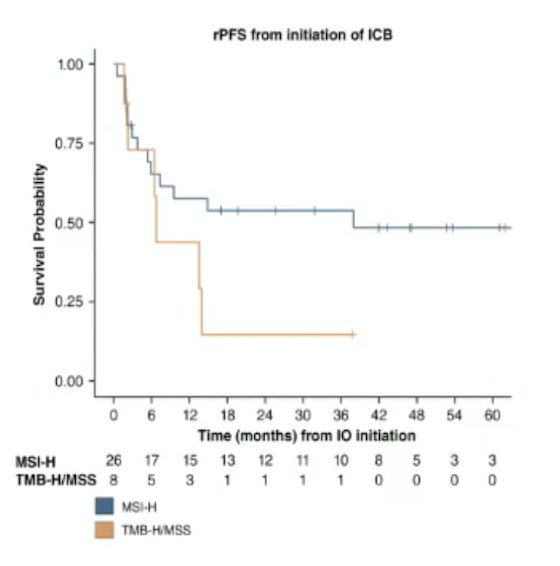
Radiographic progression-free survival tended to be longer in patients with MSI-H/dMMR than in patients with TMB-H/MSS who received immunotherapy:
The results confirming improved outcomes with MSI-H/dMMR versus patients with TMB-H/MSS who received immunotherapy have been noted in several other studies:
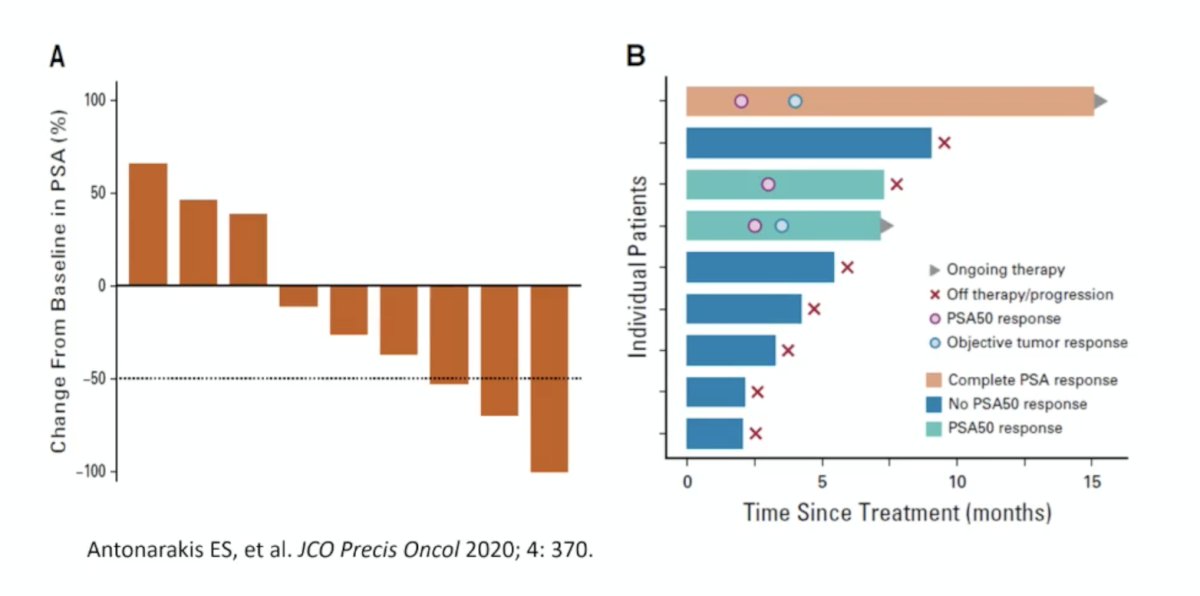
Next, Dr. Antonarakis discussed CDK12 mutations in mCRPC. Early studies suggested there was perhaps an anti-PD1 sensitivity for CDK12 mutations, based on early work from Dr. Antonarakis’ group:
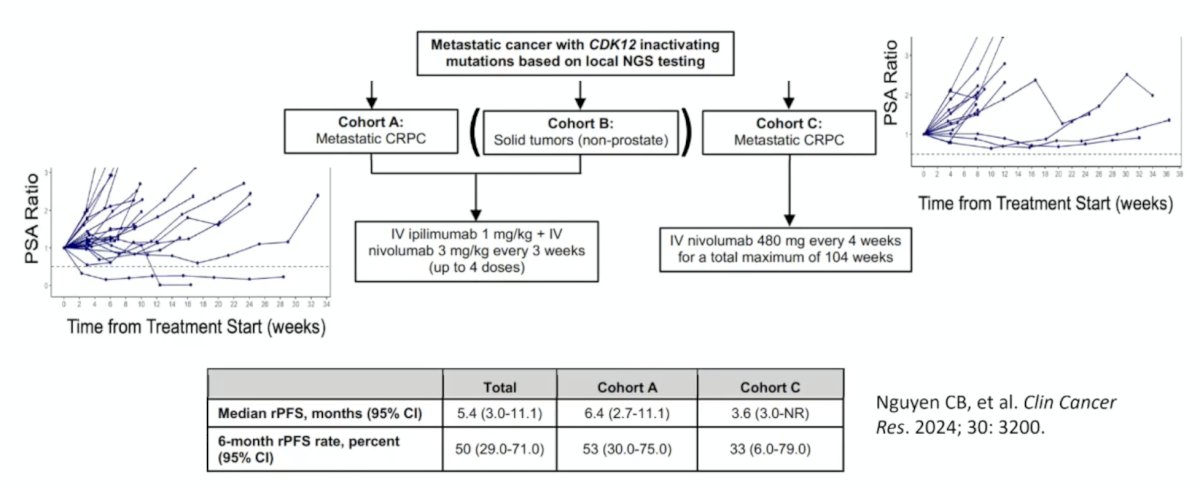
This resulted in the design of the IMPACT trial,4 which assessed immunotherapy among patients with CDK12-mutated mCRPC. In IMPACT, Cohort A received ipilimumab (1 mg/kg) with nivolumab (3 mg/kg) every 3 weeks for up to four cycles, followed by nivolumab 480 mg every 4 weeks. Cohort C received nivolumab alone at 480 mg every 4 weeks. The primary endpoint was a PSA50 response. The PSA50 rate was 9% in cohort A with two responders, and there were no PSA50 responses in cohort C. The median PSA progression-free survival was 7.0 months (95% CI, 3.6-11.4) in cohort A and 4.5 months (95% CI, 3.4-13.8) in cohort C. The median overall survival was 9.0 months (95% CI, 6.2-12.3) in cohort A and 13.8 months (95% CI, 3.6-not reached) in cohort C:
Because cabozantinib has been shown to induce favorable changes in the tumor microenvironment and regression of prostate tumors in vivo, it was subsequently combined with atezolizumab in the phase 3 CONTACT-02 trial.5 In this trial, patients were randomized 1:1 to cabozantinib + atezolizumab (cabozantinib [40 mg PO daily] + atezolizumab [1200 mg IV every 3 weeks]) or control (abiraterone [1000 mg PO daily] + prednisone [5 mg PO twice daily] or enzalutamide [160 mg PO daily]) and were stratified by liver metastasis (yes/no), prior docetaxel for mHSPC (yes/no), and prior novel hormonal therapy for mHSPC, M0CRPC, or mCRPC. The trial design for CONTACT-02 is as follows:
![Because cabozantinib has been shown to induce favorable changes in the tumor microenvironment and regression of prostate tumors in vivo, it was subsequently combined with atezolizumab in the phase 3 CONTACT-02 trial.5 In this trial, patients were randomized 1:1 to cabozantinib + atezolizumab (cabozantinib [40 mg PO daily] + atezolizumab [1200 mg IV every 3 weeks]) or control (abiraterone [1000 mg PO daily] + prednisone [5 mg PO twice daily] or enzalutamide [160 mg PO daily]) and were stratified by liver metastasis (yes/no), prior docetaxel for mHSPC (yes/no), and prior novel hormonal therapy for mHSPC, M0CRPC, or mCRPC. The trial design for CONTACT-02 is as follows:](/images/com-doc-importer/262-apccc-2026/apccc-2026-are-there-patients-with-mcrpc-who-may-benefit-from-immunotherapy/image-12.jpg)
The median follow-up was 12.0 months for all randomized patients and 14.3 months for the first 400 patients. The median radiographic progression-free survival was significantly longer with cabozantinib + atezolizumab versus control (6.3 versus 4.2 months; HR 0.65, 95% CI 0.50-0.84):

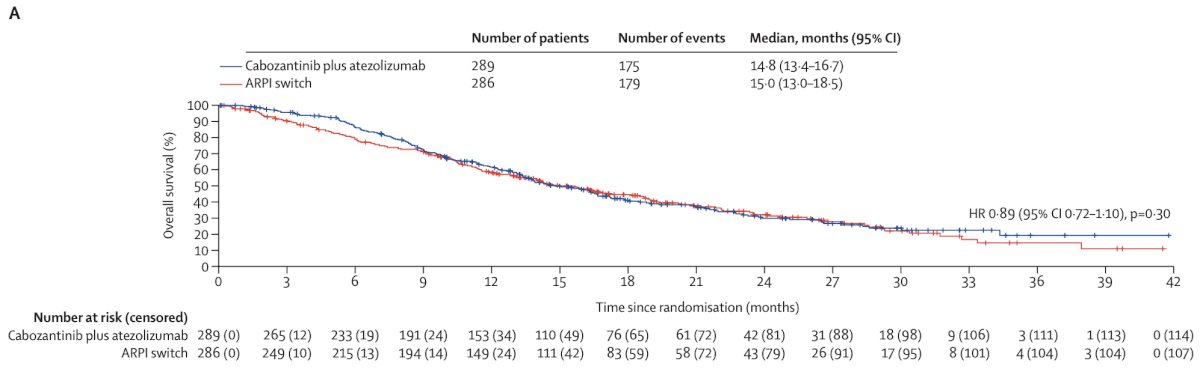
After a median follow-up of 23.1 months (IQR 17.4-30.5), overall survival was not significantly different between the cabozantinib + atezolizumab and androgen receptor pathway inhibitor switch groups (median 14.8 months versus 15.0 months; HR 0.89, 95% CI 0.72-1.10, p = 0.30):
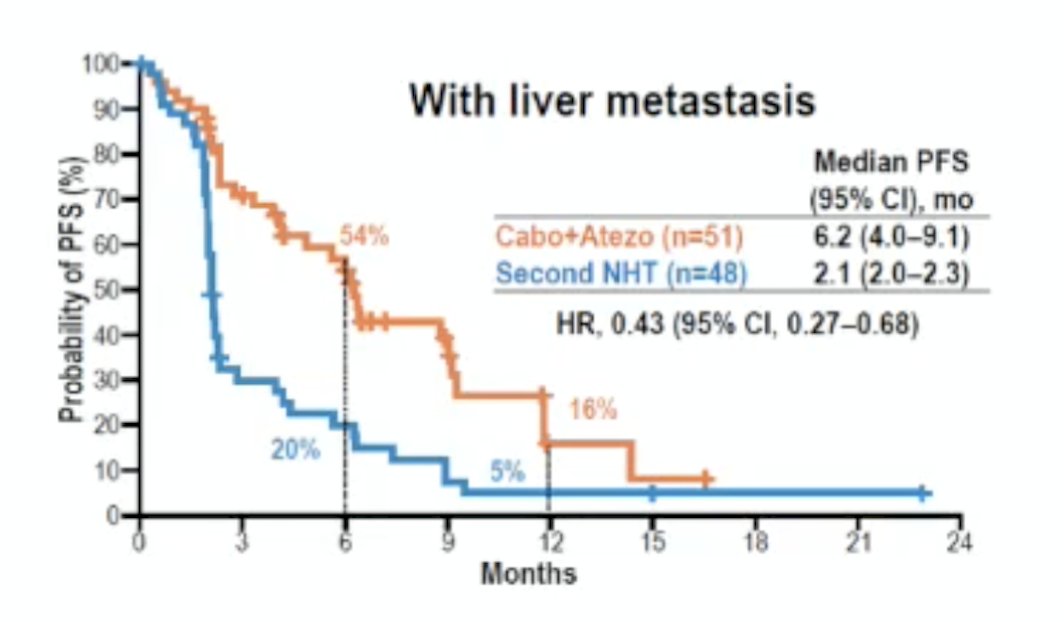
Patients with liver metastasis may have a radiographic progression-free survival benefit from cabozantinib + atezolizumab (HR 0.43, 95% CI 0.27-0.68). Dr. Antonarakis is skeptical whether this combination will get FDA approval for this indication:
Dr. Antonarakis provided the following conclusions regarding the CONTACT-02 trial:
- Contact-02 met its progression-free survival co-primary endpoint (HR 0.65, P<0.01), but not its overall survival co-primary endpoint (HR 0.89, p = 0.30)
- Progression-free survival and overall survival trends were greatest in liver metastasis subsets
- Neither cabozantinib nor atezolizumab is currently FDA/EMA approved
- Regulatory approval may(?) be sought for the liver metastasis subset
- Open question: Does the atezolizumab add anything?
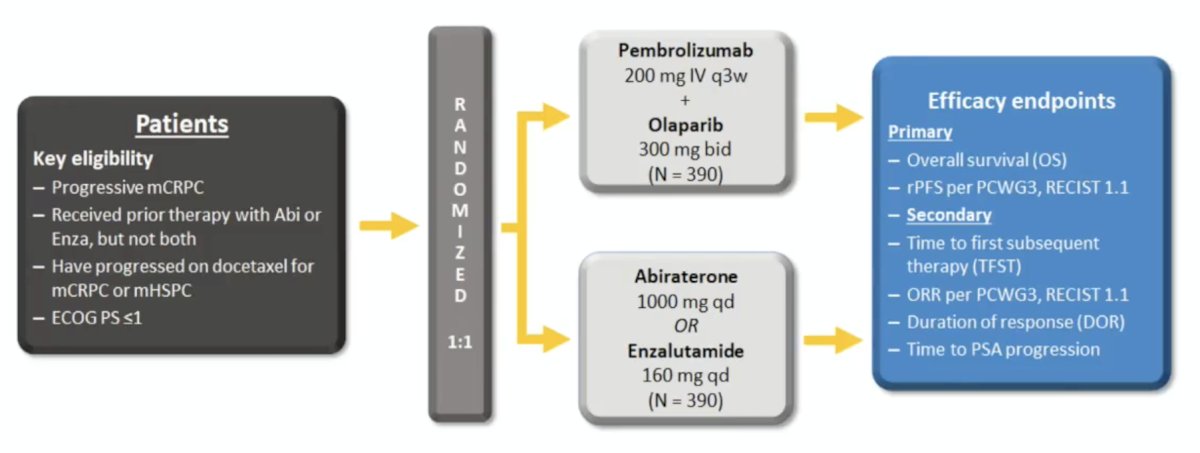
Finally, Dr. Antonarakis discussed the KeyLynk-010 trial assessing pembrolizumab + olaparib versus an androgen receptor pathway inhibitor. This phase 3 open-label trial evaluated pembrolizumab + olaparib versus a next-generation hormonal agent for biomarker-unselected, previously treated mCRPC. Eligible patients, aged ≥18 years, had mCRPC that progressed after abiraterone or enzalutamide (but not both), as well as docetaxel, and had an ECOG performance status ≤1. Patients were randomized 2:1 to receive either 200 mg pembrolizumab IV Q3W for ≤35 cycles + 300 mg olaparib orally BID, or a next-generation hormonal agent: 1000 mg abiraterone orally QD (if previously treated with enzalutamide) or 160 mg enzalutamide orally QD (if previously treated with abiraterone). The study design is depicted below:
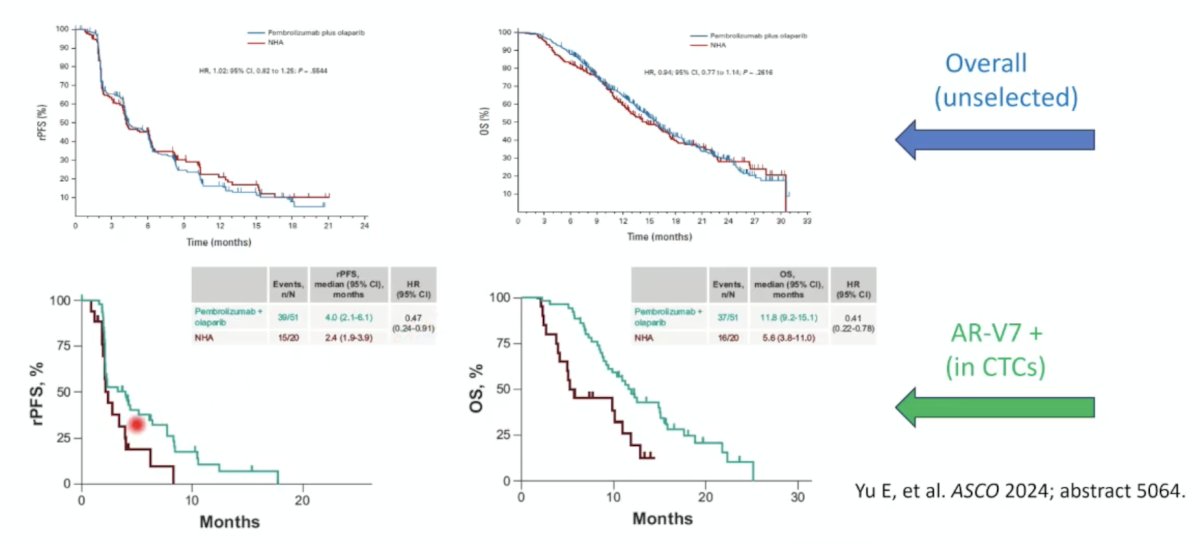
In the unselected cohort, there was no benefit to pembrolizumab + olaparib with regard to radiographic progression-free survival and overall survival, however among patients with AR-V7 positivity, there was a potential benefit in radiographic progression-free survival (HR 0.47, 95% CI 0.24-0.91) and overall survival (HR 0.41, 95% CI 0.22-0.78):
Dr. Antonarakis concluded his presentation discussing whether there are patients with mCRPC that may benefit from immunotherapy with the following take-home points:
- No immune checkpoint inhibitor is approved (by the FDA or EMA) for molecularly-unselected prostate cancer patients
- Pembrolizumab is approved for MMR-deficient (and TMB ≥10) cancers
- Multiple immune checkpoint inhibitor-based combinations have failed in phase 3 trials
- Better biomarkers of immune checkpoint inhibitor sensitivity are needed for mCRPC patients
- New immunotherapies (e.g., T cell engagers) will change the mCRPC landscape
Presented by: Emmanuel Antonarakis, MD, Clark Endowed Professor of Medicine, Division of Hematology, Oncology and Transplantation, Associate Director of Translational Research, Masonic Cancer Center, University of Minnesota, Minneapolis, MN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
- Abida W, Cheng ML, Armenia J, et al. Analysis of the prevalence of microsatellite instability in prostate cancer and response to immune checkpoint blockade. JAMA Oncol. 2019 Apr 1;5(4):471-478.
- van Wilpe S, Taha T, Rothmann EC, et al. Efficacy of anti-PD-(L)1 immunotherapy in patients with DNA mismatch repair-deficient metastatic castration-resistant prostate cancer. Eur Urol Oncol. 2025 Aug;8(4):1020-1029.
- Lenis AT Ravichandran V, Brown S, et al. Microsatellite instability, tumor mutational burden, and response to immune checkpoint blockade in patients with prostate cancer. Clin Cancer Res. 2024 Sep 3;30(17):3894-3903.
- Nguyen CB, Reimers MA, Perera C, et al. Evaluating immune checkpoint blockade in metastatic castration-resistant prostate cancers with deleterious CDK12 alterations in the phase 2 IMPACT trial. Clin Cancer Res. 2024 Aug 1;30(15):3200-3210.
- Agarwal N, Azad AA, Carles J, et al. Cabozantinib plus atezolizumab in metastatic prostate cancer (CONTACT-02): Final analyses from a phase 3, open-label, randomized trial. Lancet Oncol. 2025 Jul;26(7):860-876.