(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management of metastatic hormone-sensitive prostate cancer (mHSPC) session and a presentation by Dr. Shahneen Sandhu discussing how to select patients with mHSPC for ADT plus an androgen receptor pathway inhibitor plus a targeted therapy.
In mHSPC, the addition of an androgen receptor pathway inhibitor to ADT consistently improves overall survival and progression-free survival across both high- and low-volume disease and is now the default approach for most patients. The role of triplet therapy (ADT + docetaxel + an androgen receptor pathway inhibitor) has demonstrated further benefit in selected fit patients with high-volume disease, at the cost of increased toxicity, making patient selection and performance status key factors in decision-making. Novel biomarker-directed approaches aim to define the roles of 177Lu-PSMA-617, AKT inhibitors, and PARP inhibitors in mHSPC. There are several prognostic molecular features/biomarkers:
- Tumor-suppressor gene loss (PTEN, TP53 and/or RB1)
- AKT and/or PIK3C alterations
- HRR deficiency (BRCA1/2, CDK12 and/or PALB2 aberrations)
- SPOP mutations
- Genomic classifier
- Microsatellite instability-high and/or deficient mismatch repair
- PSMA PET molecular tumour volume
The four molecular subgroups with prognostic implications include BRCA, HRR, PTEN, and SPOP:

Dr. Sandhu notes that the prevalence of alterations in HRR-deficient tumors is similar in low and high-volume mHSPCs and previous work has suggested that biology supersedes conventional tumor volume:

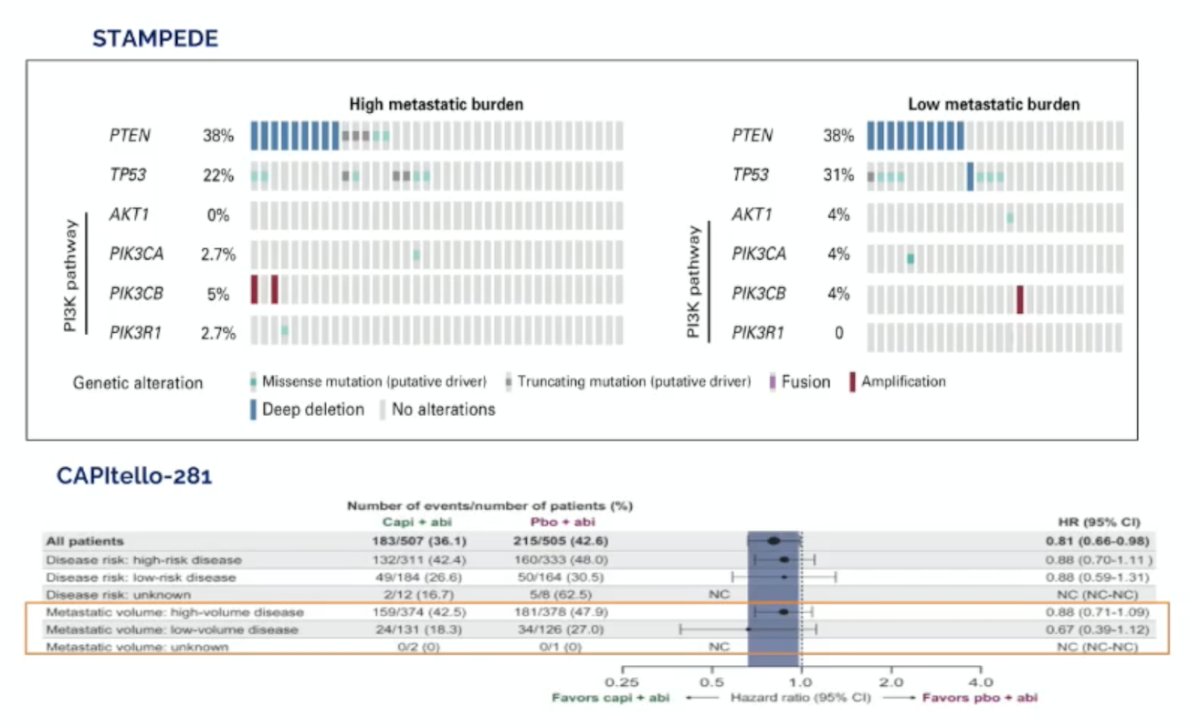
Both STAMPEDE and CAPItello-281 trials have shown that the prevalence of alterations in the PTEN PIK3CA/AKT pathway is similar in low and high-volume mHSPC:
Does molecular tumor volume matter? In a study of the ENZA-p trial,2 Emmett and colleagues found that median overall survival for PSMA total tumor volume below or above the median in the enzalutamide group was 39 months (95% CI 31-not estimable) versus 20 months (13-24; HR 0.23 [95% CI 0.13-0.42], log-rank p < 0.0001). The corresponding median overall survival for PSMA total tumor volume below or above the median in the enzalutamide + 177Lu-PSMA-617 group was 35 months (95% CI 32-37) versus 28 months (26-34; HR 0.66 [0.36-1,21], log-rank p = 0.18). The test for interaction between PSMA total tumor volume and treatment group for overall survival was p = 0.0078:
![Does molecular tumor volume matter? In a study of the ENZA-p trial [2], Emmett and colleagues found that median overall survival for PSMA total tumor volume below or above the median in the enzalutamide group was 39 months (95% CI 31-not estimable) versus 20 months (13-24; HR 0.23 [95% CI 0.13-0.42], log-rank p < 0.0001). The corresponding median overall survival for PSMA total tumor volume below or above the median in the enzalutamide + 177Lu-PSMA-617 group was 35 months (95% CI 32-37) versus 28 months (26-34; HR 0.66 [0.36-1,21], log-rank p = 0.18). The test for interaction between PSMA total tumor volume and treatment group for overall survival was p = 0.0078:](/images/com-doc-importer/262-apccc-2026/apccc-2026-how-to-select-patients-with-mhspc-for-adt-plus-an-arpi-plus-a-targeted-therapy-parp-or-akt-inhibition/image-3.jpg)
Dr. Sandhu then discussed the AMPLITUDE trial evaluating the combination of niraparib with abiraterone acetate + prednisone versus placebo and abiraterone acetate + prednisone in mHSPC with HRR gene alterations:3
![Dr. Sandhu then discussed the AMPLITUDE trial evaluating the combination of niraparib with abiraterone acetate + prednisone versus placebo and abiraterone acetate + prednisone in mHSPC with HRR gene alterations [3]:](/images/com-doc-importer/262-apccc-2026/apccc-2026-how-to-select-patients-with-mhspc-for-adt-plus-an-arpi-plus-a-targeted-therapy-parp-or-akt-inhibition/image-4.jpg)
The primary endpoint was met, with a significant improvement in radiographic progression-free survival observed in the BRCA subgroup: median not reached for niraparib and abiraterone acetate + prednisone group versus 26 months for the abiraterone acetate + prednisone group (HR 0.52, 95% CI 0.37-0.72; p < 0.0001). This was also noted in the intention to treat population (HR 0.63, 95% CI 0.49-0.80; p = 0.0001):

An FDA pooled analysis (6 trials: PROfound, PROpel, TALAPRO-2, MAGNITUDE, TRITON-2, TALAPRO-1) from 2024 assessed what the impact of PARP inhibitors are for patients with non-BRCA HRR alterations [4], noting that the benefit from PARP inhibitors appeared greatest for patients with BRCA1, BRCA2, CDK12, and PALB2 mutations:
![An FDA pooled analysis (6 trials: PROfound, PROpel, TALAPRO-2, MAGNITUDE, TRITON-2, TALAPRO-1) from 2024 assessed what the impact of PARP inhibitors are for patients with non-BRCA HRR alterations [4], noting that the benefit from PARP inhibitors appeared greatest for patients with BRCA1, BRCA2, CDK12, and PALB2 mutations:](/images/com-doc-importer/262-apccc-2026/apccc-2026-how-to-select-patients-with-mhspc-for-adt-plus-an-arpi-plus-a-targeted-therapy-parp-or-akt-inhibition/image-6.jpg)
Dr. Sandhu notes that our understanding of HRR mutations is evolving. What we know is that patients with HRR defects, namely BRCA1/2 alterations, have a poor prognosis and benefit from the biology-modulating impact of PARP inhibitor + androgen receptor pathway inhibitor. Additionally, tumor volume (conventional) is less important, and there is an increased risk of toxicity mostly in the first 3-4 months, and a long-term possibility of myelodysplastic syndrome. What we don’t know is:
- Improved molecular stratification – what is the impact of molecular tumor volume using PSMA PET scans and baseline ctDNA fraction?
- Not all BRCA1/2 mutants are the same – homozygous deletions confer benefit from single-agent PARP inhibitors, but there is no data for combinations
- Data on PARP inhibitors + androgen receptor pathway inhibitors for rarer genomic alterations – CDK12, CHEK2, PALB2, RAD51, etc. is not clear; we will likely need individual patient data meta-analysis
- The impact of co-occurring alterations – p53, Rb, PI3KCA, AKT, PTEN
- The impact on the tumor immune microenvironment is understudied – it may account for the longer-term responders and tail of the curve
- Can we de-escalate combination treatment in a subset of patients using prognostic and predictive biomarkers to inform care?
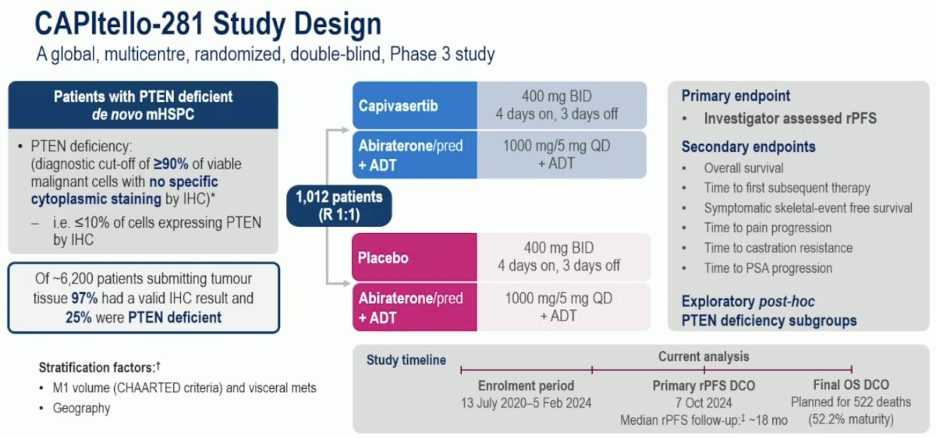
Switching to AKT inhibitors, Dr. Sandhu discussed the CAPItello-281 trial,1 which was initially presented at ESMO 2025. CAPItello-281 is a global, multicenter, randomized, double-blind, phase III trial that included patients meeting the following eligibility criteria:
- De novo mHSPC
- PTEN deficiency: ≤10% of cells expressing PTEN by immunohistochemistry (IHC)
- Of 6,200 patients submitting tumor tissue, 97% had a valid IHC result, and 25% were PTEN-deficient
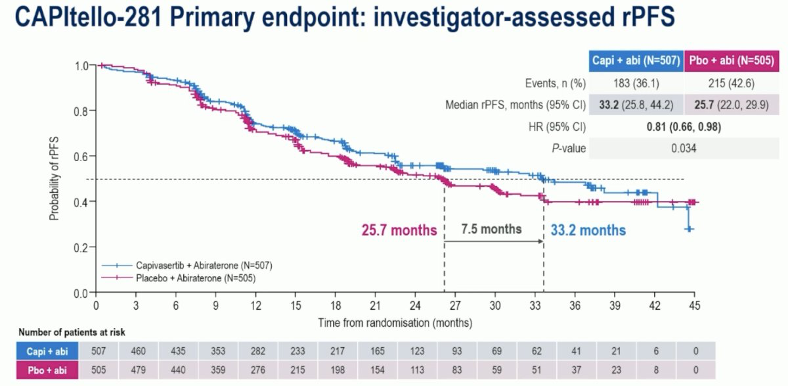
Eligible participants (n=1,012) were randomized 1:1 to capivasertib (400 mg BID, 4 days on & 3 days off) + abiraterone acetate (1,000 mg daily) + prednisone (5 mg daily) + ADT versus placebo + abiraterone acetate + prednisone + ADT. The primary endpoint was investigator-assessed radiographic progression-free survival:
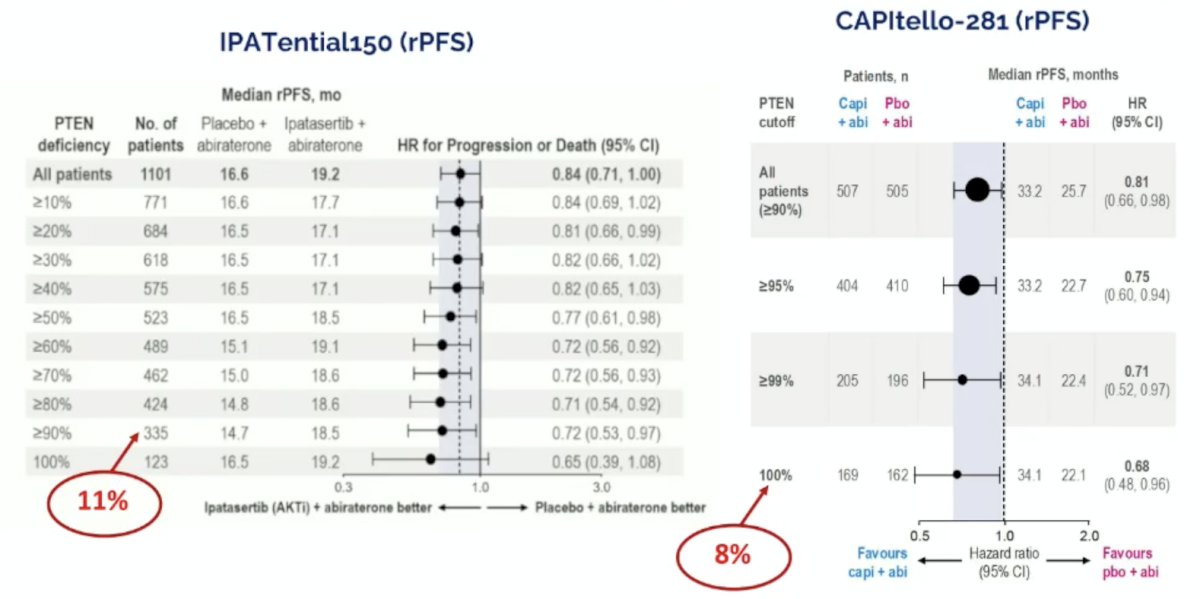
The study met its primary endpoint with capivasertib prolonging radiographic progression-free survival by 7.5 months (median: 33.2 versus 25.7 months; HR 0.81, 95% CI 0.66-0.98, p = 0.034):
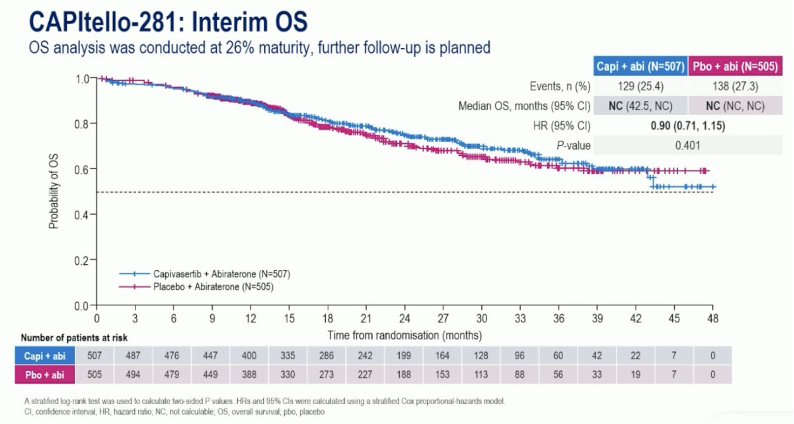
The overall survival analysis was conducted at 26% maturity (HR 0.90, 95% CI 0.71–1.15, p = 0.401):
IPATential1505 was a randomized, double-blind, phase 3 trial comparing ipatasertib + abiraterone with placebo + abiraterone in patients with previously untreated mCRPC with or without tumor PTEN loss. Patients were randomly assigned (1:1) to receive ipatasertib (400 mg once daily orally) + abiraterone (1,000 mg once daily orally) and prednisolone (5 mg twice a day orally) or placebo + abiraterone and prednisolone (with the same dosing schedule). The co-primary endpoints were investigator-assessed radiographic progression-free survival in the PTEN-loss by IHC population and in the intention-to-treat population. In the 521 (47%) patients who had tumors with PTEN loss by IHC, the median radiographic progression-free survival was 16.5 months (95% CI 13.9-17.0) in the placebo + abiraterone group and 18.5 months (16.3-22.1) in the ipatasertib + abiraterone group (HR 0.77 [95% CI 0.61-0.98]; p = 0.034). There was no overall survival benefit:
![IPATential1505 was a randomized, double-blind, phase 3 trial comparing ipatasertib + abiraterone with placebo + abiraterone in patients with previously untreated mCRPC with or without tumor PTEN loss. Patients were randomly assigned (1:1) to receive ipatasertib (400 mg once daily orally) + abiraterone (1,000 mg once daily orally) and prednisolone (5 mg twice a day orally) or placebo + abiraterone and prednisolone (with the same dosing schedule). The co-primary endpoints were investigator-assessed radiographic progression-free survival in the PTEN-loss by IHC population and in the intention-to-treat population. In the 521 (47%) patients who had tumors with PTEN loss by IHC, the median radiographic progression-free survival was 16.5 months (95% CI 13.9-17.0) in the placebo + abiraterone group and 18.5 months (16.3-22.1) in the ipatasertib + abiraterone group (HR 0.77 [95% CI 0.61-0.98]; p = 0.034). There was no overall survival benefit:](/images/com-doc-importer/262-apccc-2026/apccc-2026-how-to-select-patients-with-mhspc-for-adt-plus-an-arpi-plus-a-targeted-therapy-parp-or-akt-inhibition/image-10.jpg)
Notably, in a further assessment of the IPATential150 and CAPItello-281 trials, AKT inhibitors had an increased treatment effect with increasing PTEN deficiency:
In the final overall survival analysis report of IPATential150, De Bono and colleagues [6] found that ipatasertib did not improve overall survival for patients with PTEN loss on IHC (sHR 0.94, CI 0.76-1.17; p = 0.57) or the ITT population (sHR 0.91, 95% CI 0.79-1.07). Among the patients classified as having PTEN loss on IHC, 77% had PTEN loss on next-generation sequencing, and among the patients with PTEN loss on next-generation sequencing, 91% had PTEN loss on IHC. There was a higher concordance for next-generation sequencing with a more stringent IHC cutoff, and most PTEN loss by IHC corresponded to genomic events:
![In the final overall survival analysis report of IPATential150, De Bono and colleagues [6] found that ipatasertib did not improve overall survival for patients with PTEN loss on IHC (sHR 0.94, CI 0.76-1.17; p = 0.57) or the ITT population (sHR 0.91, 95% CI 0.79-1.07). Among the patients classified as having PTEN loss on IHC, 77% had PTEN loss on next-generation sequencing, and among the patients with PTEN loss on next-generation sequencing, 91% had PTEN loss on IHC. There was a higher concordance for next-generation sequencing with a more stringent IHC cutoff, and most PTEN loss by IHC corresponded to genomic events:](/images/com-doc-importer/262-apccc-2026/apccc-2026-how-to-select-patients-with-mhspc-for-adt-plus-an-arpi-plus-a-targeted-therapy-parp-or-akt-inhibition/image-12.jpg)
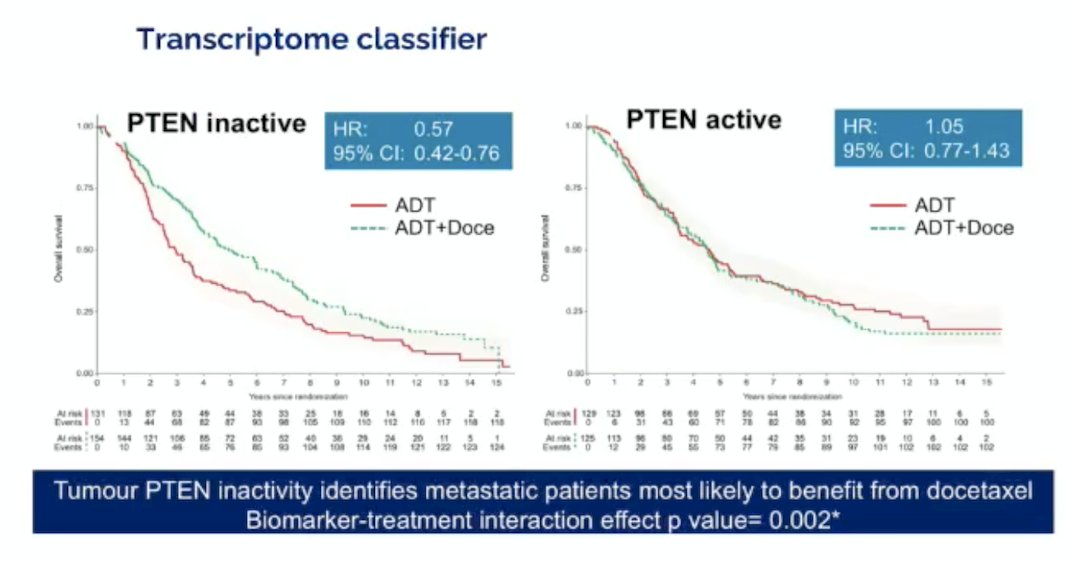
In an ancillary study of STAMPEDE presented at ASCO 2025, Dr. Emily Grist assessed transcriptomic classification of PTEN inactivation to predict benefit from docetaxel at the start of ADT. Tumors with homogeneous PTEN loss by IHC exhibited high transcriptomic PTEN inactivity scores, reflecting strong agreement between the two methods. In contrast, heterogeneous PTEN loss showed variable transcriptomic profiles, while a substantial proportion of tumors with preserved PTEN expression by IHC were still classified as PTEN-inactive at the transcriptomic level:

Among patients with PTEN-inactive tumors, the addition of docetaxel to ADT was associated with a 43% improvement in overall survival compared to ADT alone, indicating a clinically meaningful benefit. Conversely, in patients with PTEN-active tumors, there was no survival advantage with docetaxel (HR 1.05; 95% CI 0.77–1.43). These findings provide strong evidence that PTEN transcriptomic inactivity may serve as a predictive biomarker for identifying metastatic prostate cancer patients most likely to benefit from treatment intensification with docetaxel (biomarker-treatment interaction p=0.002):
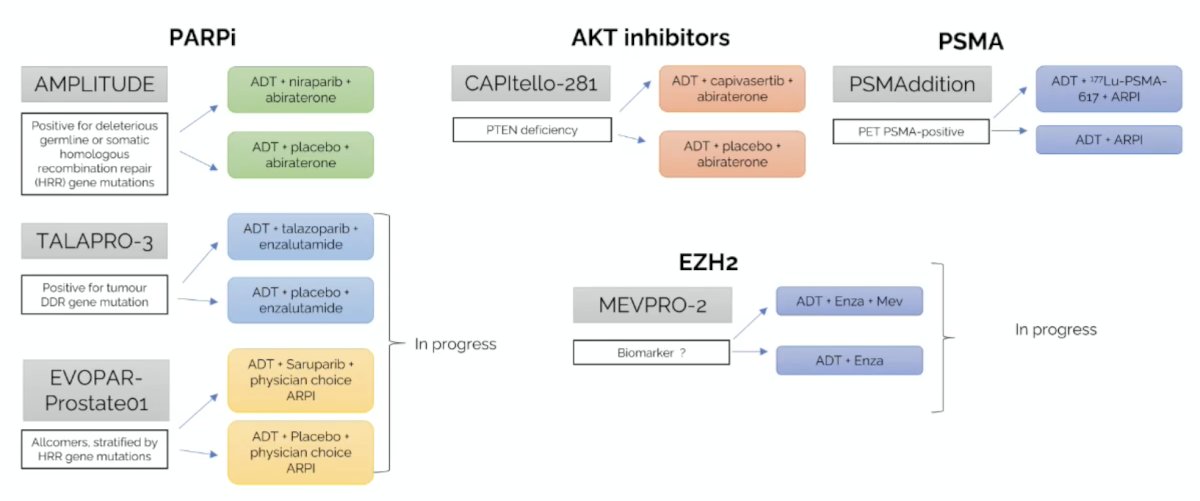
The following figure highlights patient selection for mHSPC trials:
Dr. Sandhu notes that our understanding of PTEN is evolving. What we know is that patients with PTEN loss have a worse outlook, which can be modified by abrogating AKT signaling and translates into improvement in radiographic progression-free survival. The greater the PTEN loss cut-off, the worse the prognosis and the greater the treatment effect. What we don’t know is:
- The incidence and impact of co-occurring PTEN loss (100%) and BRCA
- An optimal way to select patients – we will likely need to do next-generation sequencing for HRR in mHSPC
- AN optimal androgen receptor pathway inhibitor partner – given the >30% incidence of hyperglycemia, perhaps abiraterone is not the optimal partner
Dr. Sandhu concluded her presentation discussing how to select patients with mHSPC for ADT plus an androgen receptor pathway inhibitor plus a targeted therapy with the following take-home points:
- Treatment intensification in mHSPC carries significant morbidity, and we need to optimize patient selection
- Patients are living longer and experiencing frailty 8-10 years on from continuous ADT + androgen receptor pathway inhibitor, even without further intensification
- We need to molecularly stratify – the current framework is based on timing, and volume can be improved
- We need multimodal integration of digital pathology, genomics, transcriptomics, molecular tumor volume, baseline ctDNA, global protein expression on tissue and blood, and host factors (immune fitness)
Presented by: Shahneen Sandhu, MBBS, FRACP, Consultant Medical Oncologist, Associate Professor, Melanoma and Uro-Oncology Units, Peter MacCallum Cancer Centre, Victoria, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
- Fizazi K, Clarke NW, De Santis M, et al. Capivasertib plus abiraterone in PTEN-deficient metastatic hormone-sensitive prostate cancer: CAPItello-281 phase III study. Ann Oncol. 2026 Jan;37(1):53-68.
- Emmett L, Papa N, Subramaniam S, et al. Prognostic and predictive value of baseline PSMA-PET total tumour volume and SUVmean in metastatic castration-resistant prostate cancer in ENZA-p (ANZUP1901): A substudy from a multicentre, open-label, randomized, phase 2 trial. Lancet Oncol. 2025 Sep;26(9):1168-1177.
- Attard G, Agarwal N, Graff JN, et al. Niraparib and abiraterone acetate plus prednisone for HRR-deficient metastatic castration-sensitive prostate cancer: A randomized phase 3 trial. Nat Med. 2025 Dec;31(12):4109-4118.
- Fallah J, Xu J, Weinstock C, et al. Efficacy of Poly(ADP-ribose) Polymerase Inhibitors by Individual Genes in Homologous Recombination Repair Gene-Mutated Metastatic Castration-Resistant Prostate Cancer: A US Food and Drug Administration Pooled Analysis. J Clin Oncol. 2024 10;42(14):1687-1698.
- Sweeney C, Bracarda S, Sternberg CN, et al. Ipatasertib plus abiraterone and prednisolone in metastatic castration-resistant prostate cancer (IPATential150): A multicentre, randomized, double-blind, phase 3 trial. Lancet 2021 Jul 10;398(10295):131-142.
- De Bono JS, He M, Shi Z, et al. Final overall survival and molecular data associated with clinical outcomes in patients receiving ipatasertib and abiraterone in the phase 3 IPATential150 trial. Eur Urol. 2025 Jan 29;S0302-2838(24)02771-4.