(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a treatment of PSA recurrence or persistence session and a presentation by Dr. Piet Ost discussing that early salvage radiotherapy is equivalent to adjuvant radiotherapy in patients with high-risk localized or locally advanced disease.
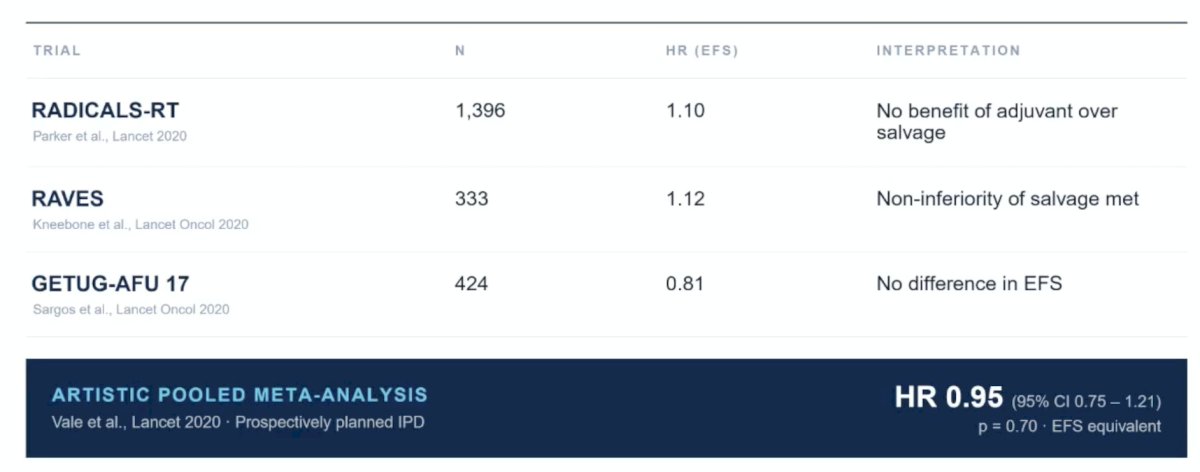
Dr. Ost started by emphasizing that for us to consider adjuvant radiotherapy in favor of early salvage radiotherapy, it should be superior, not equivalent. There have been three randomized trials (RADICALS-RT,1 RAVES,2 and GETUG-AFU 173) and the ARTISTIC pooled meta-analysis4 (HR 0.95, 95% CI 0.75-1.21) that have shown that early salvage radiotherapy is non-inferior to adjuvant radiotherapy:
In 2024, Parker et al.5 reported 10-year outcomes of the RADICALS-RT trial. With 80 distant metastasis events, 10-year freedom from distant metastasis was 93% for adjuvant radiotherapy and 90% for salvage radiotherapy: HR 0.68 (95% CI 0.43-1.07, p = 0.095). Dr. Ost notes that the 3% gap is not significant. An underpowered, secondary endpoint, with a confidence interval crossing 1, does not justify irradiating the 70% who never needed it.
Additionally, the side effects of adjuvant radiotherapy are real, as highlighted in the long-term RADICALS-RT follow-up. For five late RTOG side effect metrics (grade 1-2), all were significantly higher in the adjuvant versus the early salvage group. Additionally, the patient-reported outcomes adjusted for baseline all favored salvage radiotherapy:

Dr. Ost notes that the cost of a universal adjuvant policy would be that we would irradiate 100 patients in order to benefit 30 patients. Approximately 30% of pT3/R1 patients develop biochemical recurrence at 10 years, which means that 70% of patients irradiated under a universal policy gain nothing. Adjuvant radiotherapy is not personalized medicine; it is defensive oncology applied at scale.
An argument may be that the trials do not apply “to my high-risk population,” but Dr. Ost emphasized that the trials did enroll the high-risk population: 68-71% of RADICALS-RT patients had pT3 disease, positive margins, or Gleason 7-10 prostate cancer. RADICALS-RT required at least one adverse feature after radical prostatectomy, and ARTISTIC pooled three populations built on the same inclusion criteria. Furthermore, the HR for the Gleason 8-10 subgroup was 1.14 (95% CI 0.63-2.04), with no signal suggesting these patients should get adjuvant radiotherapy.
Additionally, the cost of a selective adjuvant policy would be to irradiate 100 patients in order to benefit 80 patients. This would be the case given that ~80% patients were ISUP Grade Group 4-5 + pT3 or pN1, thus 20% of patients radiated under this plan would gain nothing.
Another argument is that in the PSMA ear, salvage is not early anymore. Dr. Ost notes that PSMA guides the field, not the decision. The EAU guidance is explicit: a negative PSMA PET should not delay salvage radiotherapy if otherwise indicated. The “PSMA drift” argument is a workflow problem, not an indictment of salvage radiotherapy.
Dr. Ost emphasized that the guidelines support his stance for early salvage radiotherapy:
- EAU guidelines 2026
- Offer early salvage intensity-modulated radiotherapy to men with two consecutive PSA rises (strong). Do not wait for a PSA threshold
- Offer monitoring to EAU low-risk biochemical recurrence (weak)
- Offer adjuvant radiotherapy for ISUP Grade Group 4-5 and pT3 (weak)
- NCCN 2026
- Salvage radiotherapy is graded Category 1
- Adjuvant radiation may be reasonable for patients with multiple adverse features
- ESMO guidelines 2026
- Early salvage radiotherapy for patients with biochemical recurrence if there is a risk of metastatic progression (Category III, B)
- Surveillance for biochemical recurrence and low risk of metastatic progression (Category III, B)
The answer to a public health problem is not systematic overtreatment. What early salvage radiotherapy does not cover is (i) waiting for a PSA > 0.5 ng/mL, (ii) pN+, (iii) waiting for a positive PSMA PET/CT, and (iv) PSA persistence. A prerequisite is adequate PSA monitoring and early referral to radiation oncology.
Dr. Ost concluded his presentation discussing that early salvage radiotherapy is equivalent to adjuvant radiotherapy in patients with high-risk localized or locally advanced disease, with the following take-home points:
- We have three trials and one meta-analysis that are equivalent
- HR 0.95, 95% CI 0.75-1.21; p = 0.70 across 2,153 randomized patients
- 70% of adjuvant patients are irradiated for no personal benefit and carry the side effects for a decade
- PSA triggered early salvage radiotherapy is now an international guideline standard of care
- Primum Non Nocere
Presented by: Piet Ost, MD, PhD, Associate Professor (Faculty of Medicine and Health Sciences, UGent), Radiation Oncologist at the Iridium Network, GZA Ziekenhuizen, Antwerp, Chair of the EORTC Radiation Oncology Science Council, Ghent University, Ghent, Belgium
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:- Parker CC, Clarke NW, Cook AD, et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): A randomized, controlled phase 3 trial. Lancet 2020;396(10260):1413-1421.
- Kneebone A, Fraser-Browne C, Duchesne GM, et al. Adjuvant radiotherapy versus early salvage radiotherapy following radical prostatectomy (TROG 08.03/ANZUP RAVES): A randomized, controlled, phase 3, non-inferiority trial. Lancet Oncol. 2020;21(10):1331-1340
- Sargos P, Chabaud S, Latorzeff I, et al. Adjuvant radiotherapy versus early salvage radiotherapy plus short-term androgen deprivation therapy in men with localized prostate cancer after radical prostatectomy (GETUG-AFU 17): A randomized, phase 3 trial. Lancet Oncol 2020;21(10):1341-1352.
- Vale CL, Fisher D, Kneebone A, et al. Adjuvant or early salvage radiotherapy for the treatment of localized and locally advanced prostate cancer: A prospectively planned systematic review and meta-analysis of aggregate data. Lancet 2020 Oct 31;396(10260):1422-1431.
- Parker CC, Peterson PM, Cook AD, et al. Timing of radiotherapy (RT) after radical prostatectomy (RP): Long-term outcomes in the RADICALS-RT trial (NCT00541047). Ann Oncol. 2024 Jul;35(7):656-666.