(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a treatment of PSA recurrence or persistence session and a presentation by Dr. Pierre Blanchard discussing how to react to PSA recurrence after radiotherapy.
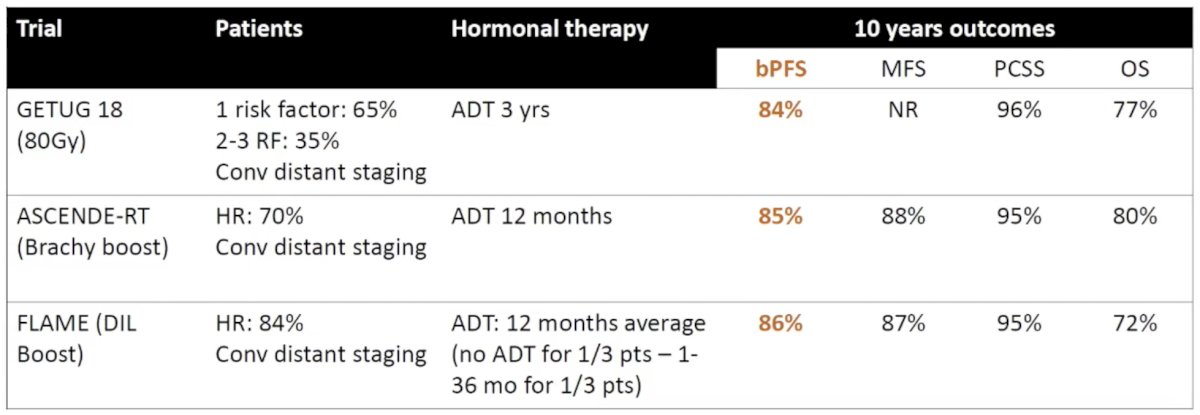
Dr. Blanchard started his presentation by highlighting the frequency of PSA recurrence after radiotherapy and the case of high-risk localized disease (relapse according to the Phoenix criteria):
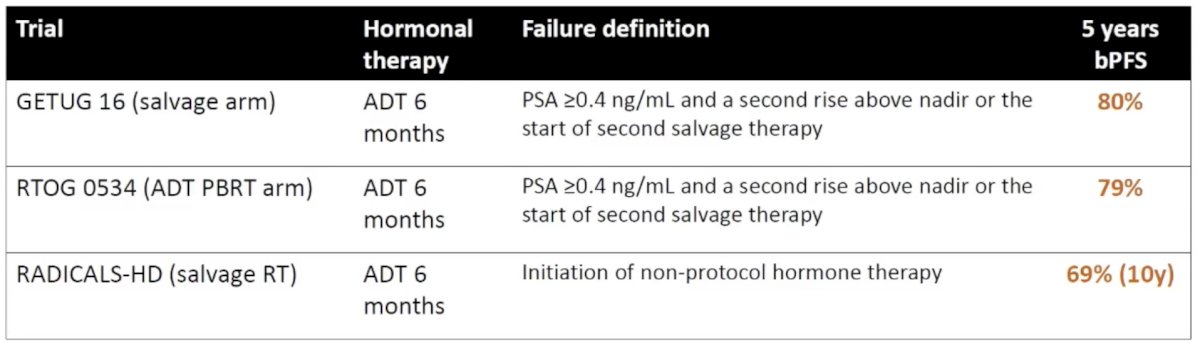
Additionally, the frequency of PSA recurrence after radiotherapy and the case of salvage radiotherapy in the pre-PSMA PET era:
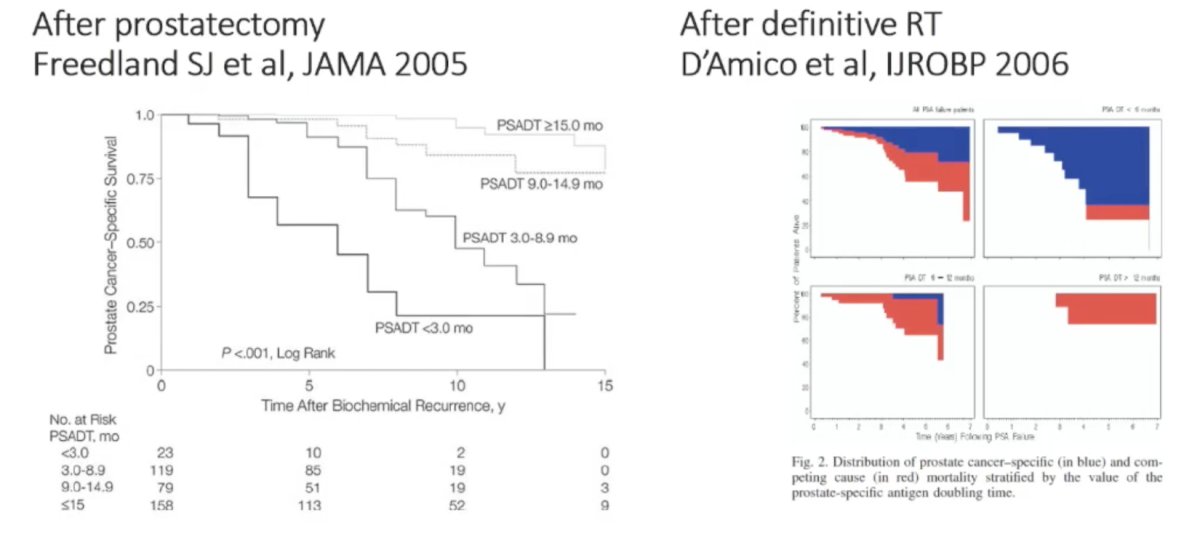
PSA doubling time is a strong prognostic factor of prostate cancer death after local therapy, whether the patient received a radical prostatectomy or definitive radiotherapy:
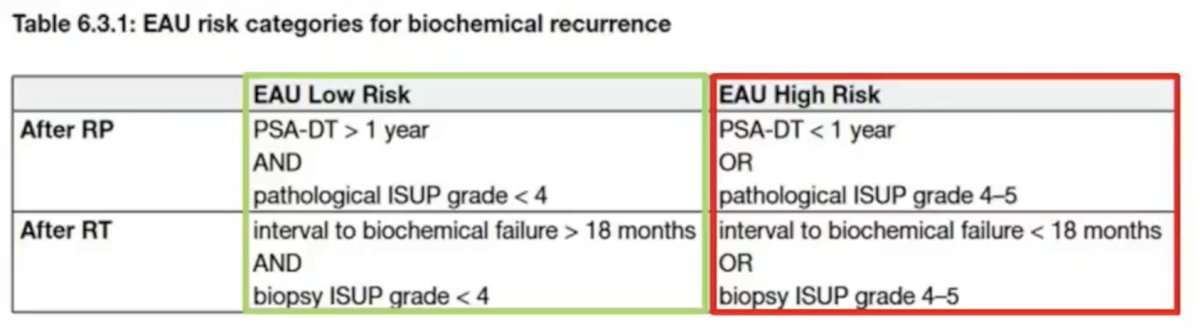
As such, the EAU risk categories for biochemical recurrence provide risk stratification and guidance for treatment of patients, whether they underwent a radical prostatectomy or definitive radiotherapy:
In 2025, van Altena et al.1 investigated the detection rate and extent of prostate cancer recurrences using PSMA PET/CT after curative radiotherapy among patients with a PSA rise of ≥2.0 ng/ml above the nadir (Phoenix positive) and patients not reaching this threshold (Phoenix negative) and to compare therapeutic management and clinical outcomes in terms of time to ADT and CRPC, as well as overall survival. There were 222 patients (39.1%) classified as Phoenix negative and 346 (60.9%) classified as Phoenix positive. PSMA-avid lesions were detected in 170 Phoenix-negative patients (76.6%) and 322 (93.1%) Phoenix-positive patients. In these groups, 75.9% of Phoenix negative patients and 45.0% of Phoenix positive patients were eligible for local salvage therapy (OR 3.84; p < 0.001). Distant metastases were less frequent in the Phoenix negative group (n = 37, 21.8%) than in the Phoenix positive group (n = 157, 48.8%; OR 0.29; p < 0.001). Survival analyses revealed longer times to ADT (re)initiation and progression to CRPC, as well as lower overall mortality, in the Phoenix negative group (log-rank p < 0.001). Thus, for patients with prostate cancer recurrence, PSMA PET/CT can detect this recurrence in the majority of cases not meeting the Phoenix criteria for biochemical recurrence. Early imaging detects recurrences at a less advanced disease stage, allowing potential salvage treatments.
Dr. Blanchard notes that when to react after PSA recurrence after radiotherapy is unclear. There are multiple factors at play, including:
- Patient age, life expectancy, and comorbidities
- Risk of further disease progression:
- EAU risk group
- Absolute PSA (depending on local therapy – EMBARK thresholds?)
- PSA doubling time
- The earlier we react, the more we’ll find oligorecurrent disease, which may lead to overtreatment in some patients, but also long-term cure in others
- Workup is only justified if treatment will be decided based on its results
When biochemical recurrence after radiotherapy occurs, PSMA is the tracer of choice. PSMA is better than conventional imaging based on the proPSMA study,2 and PSMA is better than choline PET/CT based on the PYTHON trial:
![When biochemical recurrence after radiotherapy occurs, PSMA is the tracer of choice. PSMA is better than conventional imaging based on the proPSMA study [2] and PSMA is better than choline PET/CT based on the PYTHON trial:](/images/com-doc-importer/262-apccc-2026/apccc-2026-psa-recurrence-after-radiotherapy---when-and-how-to-react/image-4.jpg)
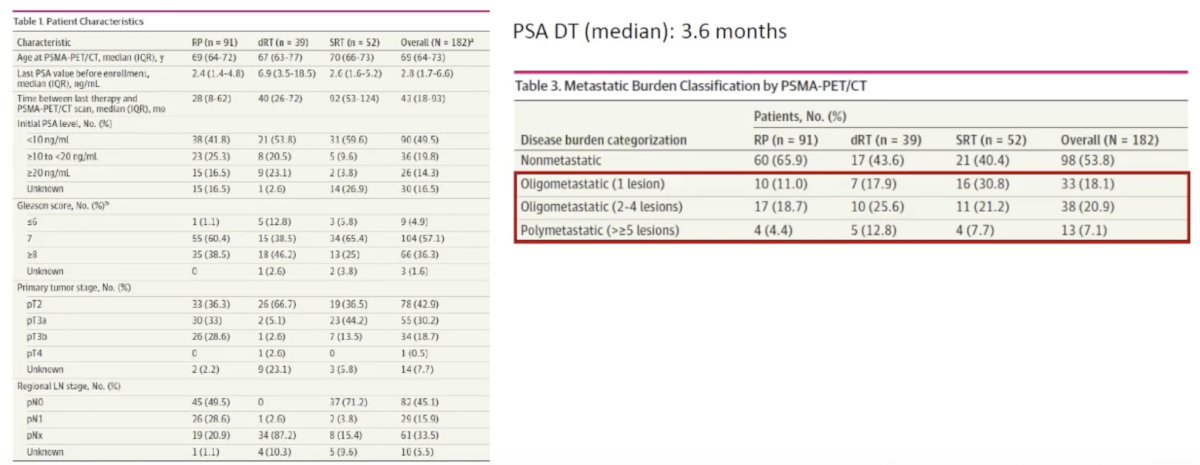
In 2025, Holzgreve et al.3 described the staging information obtained by PSMA PET/CT in a patient cohort eligible for the EMBARK trial. Among 182 included patients, the median pre-scan PSA levels were 2.4 ng/mL (IQR, 1.4-4.8 ng/mL) after radical prostatectomy (n = 91), 6.9 ng/mL (IQR, 3.5-18.5 ng/mL) after definitive radiotherapy (n = 39), 2.6 ng/mL (IQR, 1.6-5.2 ng/mL) after radical prostatectomy and salvage radiotherapy (n = 52), and 2.8 ng/mL (IQR, 1.7-6.6 ng/mL) overall. Results of PSMA-PET were positive in 80% of patients (73 of 91) after radical prostatectomy, 92% of patients (36 of 39) after definitive radiotherapy, 85% of patients (44 of 52) after radical prostatectomy and salvage radiotherapy, and 84% of patients (153 of 182) overall:
Local relapse after definitive radiotherapy is clinically important since it predicts overall survival, prostate cancer-specific survival, and distant metastasis-free survival among high-risk patients, and predicts distant metastasis-free survival for those with intermediate-risk disease.
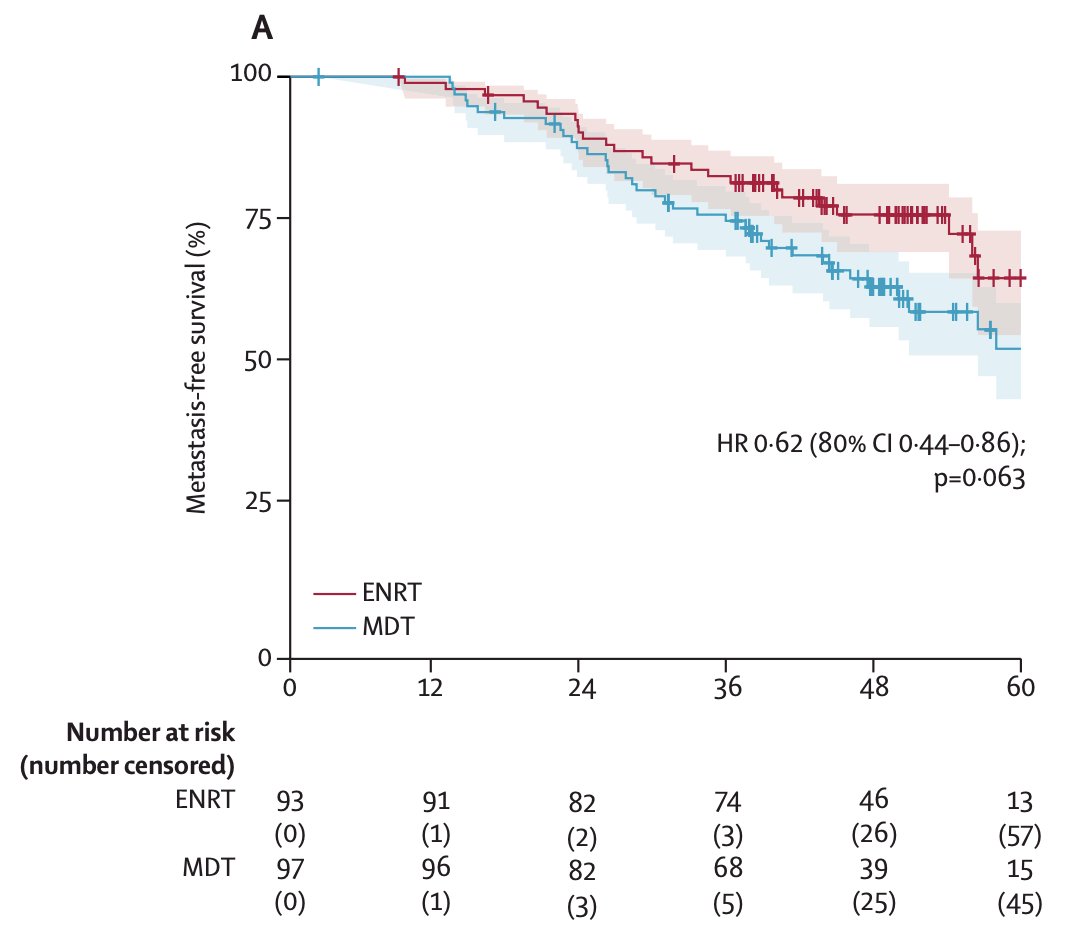
Regarding regional recurrences, the PEACE-V/STORM trial4 aimed to assess whether elective nodal radiotherapy to the pelvis would be superior to metastasis-directed therapy. Among 190 evaluable patients (metastasis directed therapy n = 97; elective nodal radiotherapy n = 93), over a median follow up of 50 months (IQR 42-58), the 4-year metastasis free survival was 63% (80% CI 56-69) in the metastasis directed therapy group and 76% (80% CI 69-81) in the elective nodal radiotherapy group (HR 0.62, 80% CI 0.44-0.86; p = 0.063):
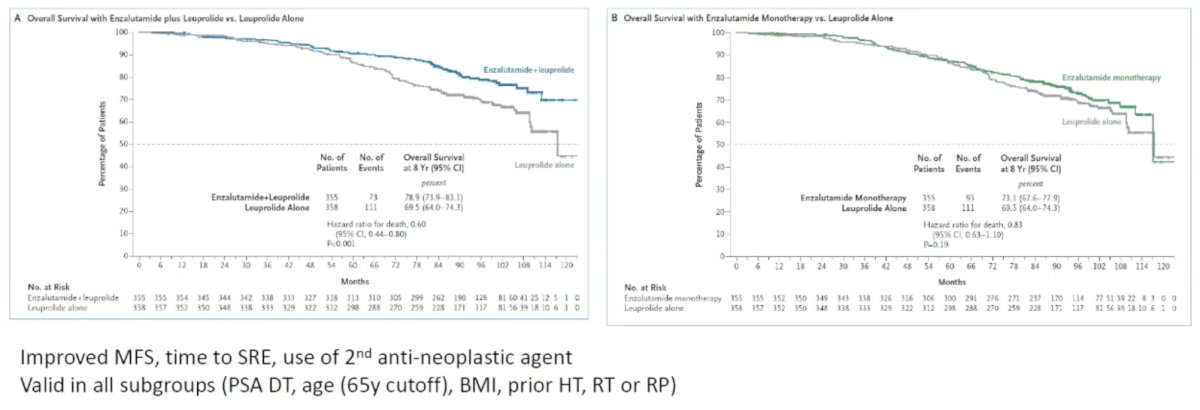
For high-risk patients, Dr. Blanchard states that patients should be treated with EMBARK5 therapy options, given the improved metastasis-free survival for enzalutamide + leuprolide versus leuprolide and enzalutamide versus leuprolide:
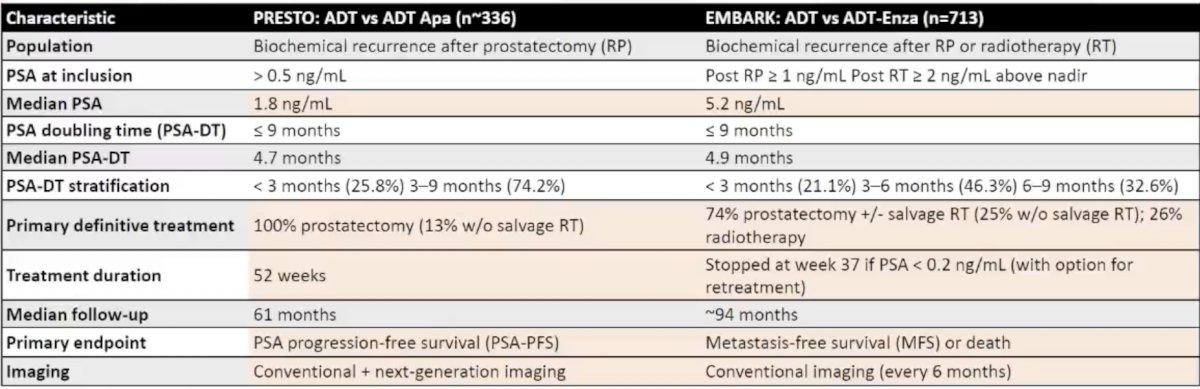
Whereas EMBARK was an overwhelmingly positive trial, PRESTO6 did not show a benefit of LHRH + apalutamide in high-risk biochemical recurrence after radical prostatectomy. How do we explain the differences between EMBARK and PRESTO? Dr. Blanchard notes that this is likely a class effect for androgen receptor pathway inhibitors. Additionally, EMBARK was a large trial with more power, and there were higher-risk patients in PRESTO (higher PSA), with a significant proportion having suboptimal local therapy. EMBARK also included a break based on PSA, and a retreatment period:
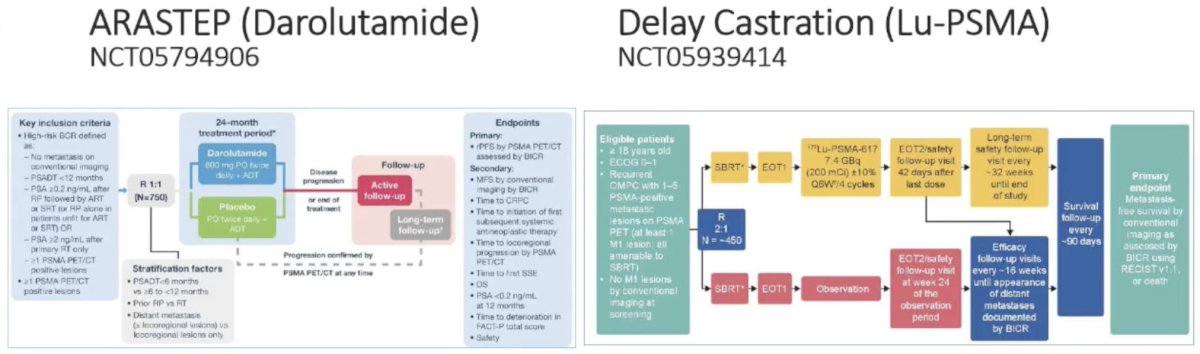
Ongoing trials in patients with PSMA-positive high-risk biochemical recurrence include ARASTEP and PSMA-DC:
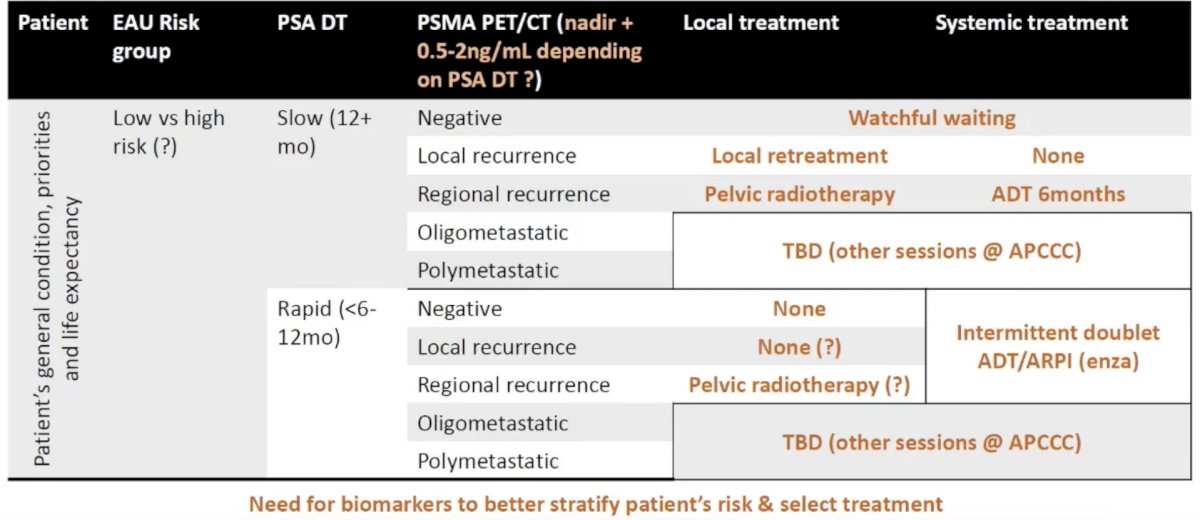
Dr. Blanchard concluded his presentation discussing how to react to PSA recurrence after radiotherapy by providing his working proposal for how to manage these patients:
Presented by: Pierre Blanchard, MD, PhD, Professor of Radiation Oncology, Institut de Cancérologie, Gustave Roussy Cancer Center, Villejuif, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:- Van Altena EJE, Jansen BHE, Korbee ML, et al. Prostate-specific membrane antigen positron emission tomography before reaching the Phoenix criteria for biochemical recurrence of prostate cancer after radiotherapy: Earlier detection of recurrences. Eur Urol Oncol. 2025 Apr;8(2):417-424.
- Hofman MS, Lawrentschuk N, Francis, RJ, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomized, multicentre study. Lancet 2020 Apr 11;395(10231):1208-1216.
- Holzgreve A, Armstrong WR, Clark KJ, et al. PSMA-PET/CT findings in patients with high-risk biochemically recurrent prostate cancer with no metastatic disease by conventional imaging. JAMA Netw Open. 2025 Jan 2;8(1):e2452971.
- Ost P, Siva S, Brabrand S, et al. Salvage metastasis-directed therapy versus elective nodal radiotherapy for oligorecurrent nodal prostate cancer metastases (PEACE V-STORM): A phase 2, open-label, randomized controlled trial. Lancet Oncol. 2025 Jun;26(6):695-706.
- Freedland SJ, de Almeida Luz M, De Giorgi U, et al. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med 2023 Oct 19;389(16):1453-1465.
- Aggarwal R, Heller G, Hillman DW, et al. PRESTO: A Phase III, Open-Label Study of Intensification of Androgen Blockade in Patients with High-Risk Biochemically Relapsed Castration-Sensitive Prostate Cancer (AFT-19). J Clin Oncol. 2024 Apr 1;42(10):1114-1123.