(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management and prevention of frequent side effects and modifying the metabolism session, and a presentation by Dr. Anthony Joshua discussing the evidence for using metformin in advanced prostate cancer.
It is important to note that 25% of deaths that occur after a diagnosis of mHSPC are non-cancer related and are most commonly secondary to cardiovascular disease. Because of the metabolic effects of ADT, there has been interest in the potential role of metformin for advanced prostate cancer patients. Metformin has both direct and indirect mechanisms of action, as highlighted in the following figure:

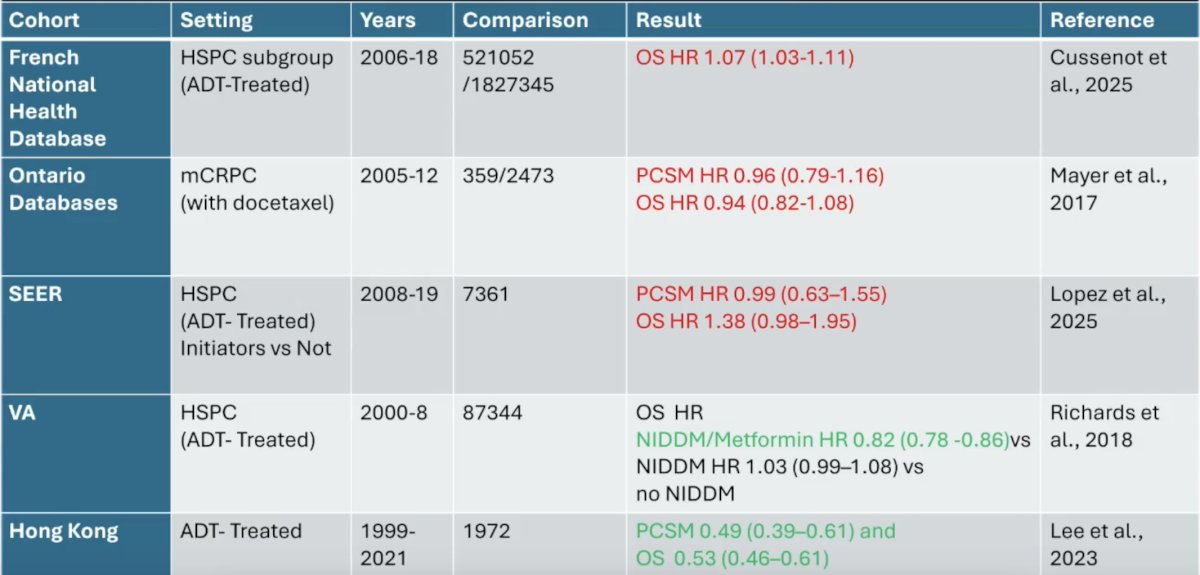
From an epidemiological perspective, metformin primarily has an effect on decreasing the risk of non-insulin-dependent diabetes mellitus, with little/no effect on prostate cancer and overall mortality:
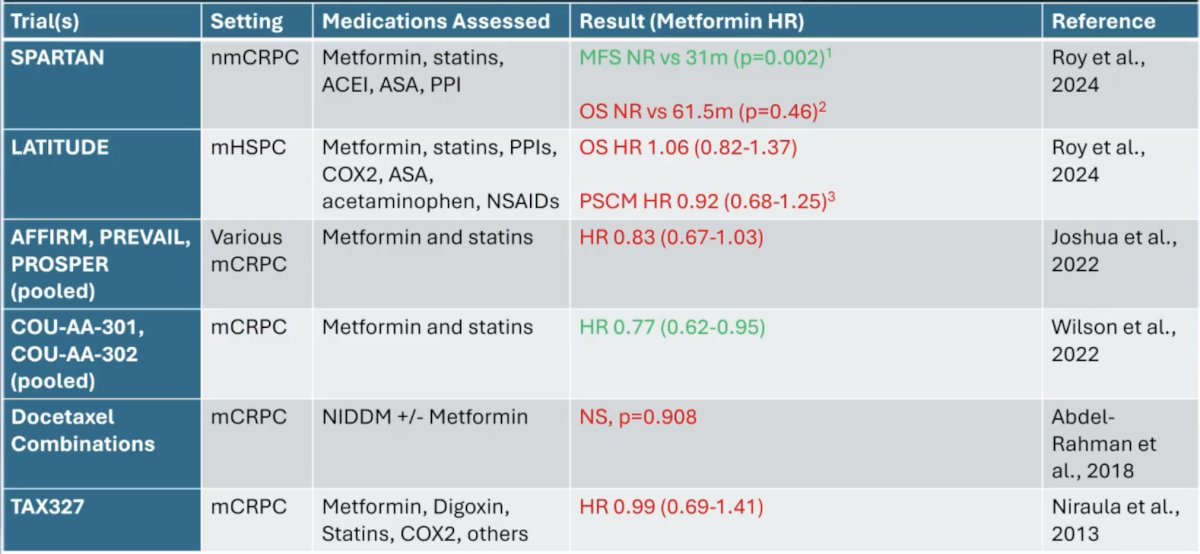
Generally, similar findings have been reported in retrospective analyses of phase 3 advanced prostate cancer trials:
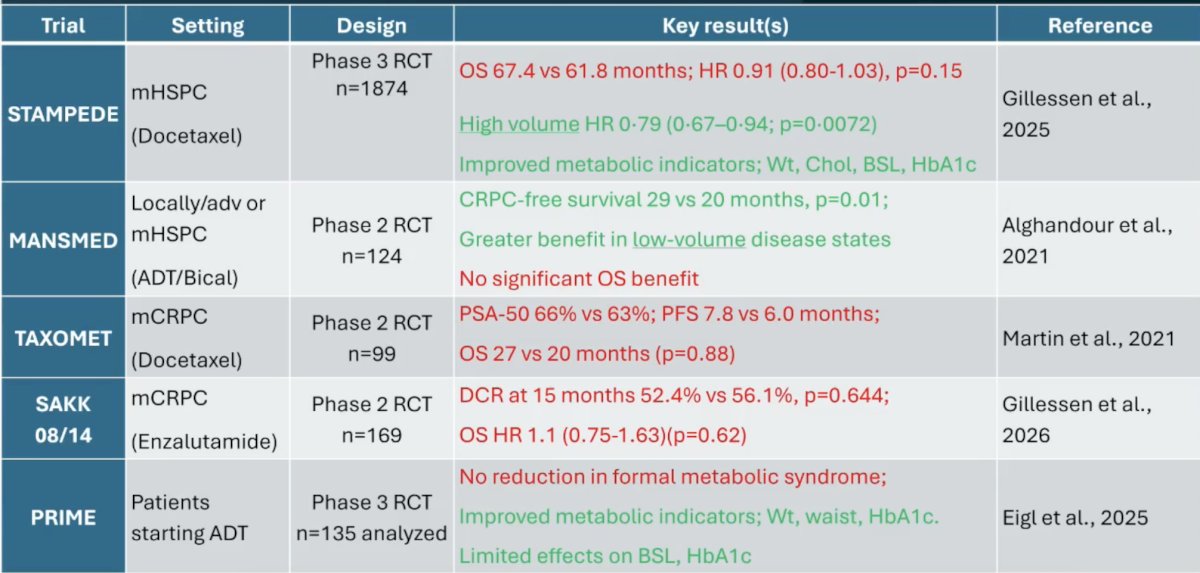
There have been 5 prospective randomized trials assessing the effect of metformin on various clinical outcomes, with varying degrees of effect:
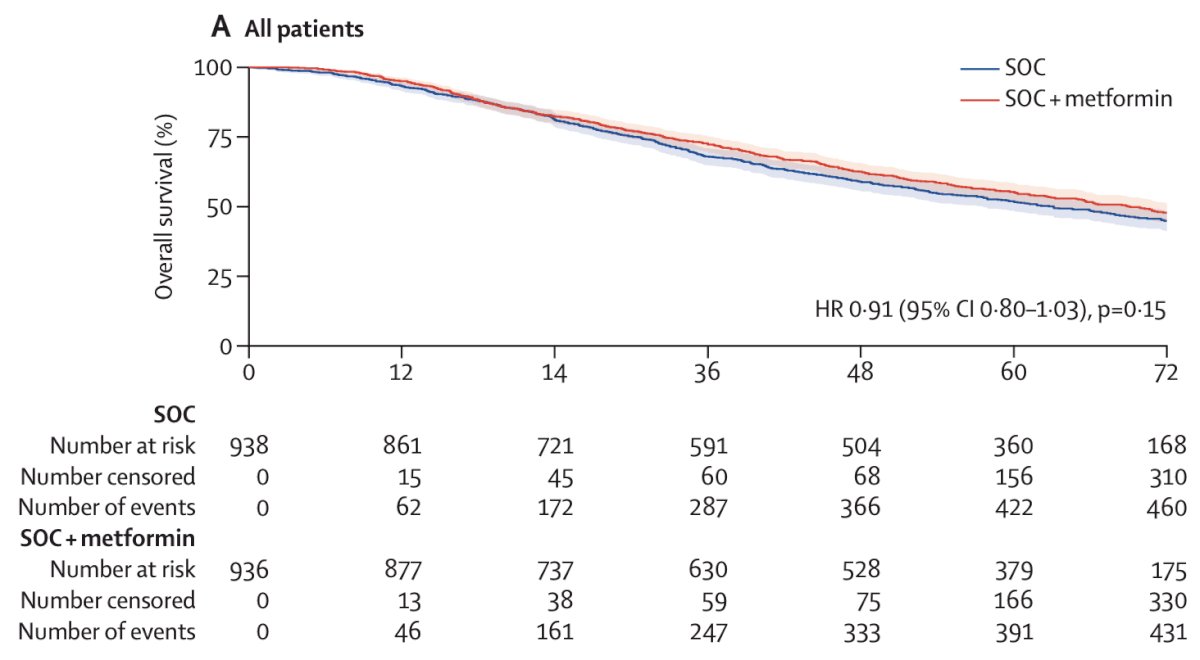
Dr. Joshua discussed the STAMPEDE platform trial in more detail, which hypothesized that metformin might improve survival in patients with mHSPC and reduce metabolic complications associated with ADT.1 Patients were randomly allocated (1:1) to standard of care or standard of care plus metformin 850 mg twice daily. Patients were stratified for randomizing hospital, age (<70 years versus ≥70 years), WHO performance status (0 versus 1 or 2), type of ADT, regular long-term use of aspirin or non-steroidal anti-inflammatory drugs (NSAIDs; yes versus no), pelvic nodal status (positive versus negative), planned radiotherapy (yes versus no), and planned docetaxel or androgen receptor pathway inhibitor use (docetaxel versus abiraterone, enzalutamide, or apalutamide versus none). The primary outcome measure was overall survival, defined as the time to death from any cause, assessed in the intention-to-treat population.
There were 1,874 patients with metastatic disease randomly allocated to standard of care (n = 938) or standard of care plus metformin (n = 936). Overall, 1,543 (82%) of 1,874 patients received ADT + docetaxel, and 52 (3%) received abiraterone, enzalutamide, or apalutamide. There were 473 deaths reported in the standard of care group, with a median overall survival of 61.8 months (IQR 29.7 to not reached), and 453 deaths in the metformin group with a median survival of 67.4 months (IQR 32.5 to not reached; HR 0.91, 95% CI 0.80-1.03; p = 0.15):
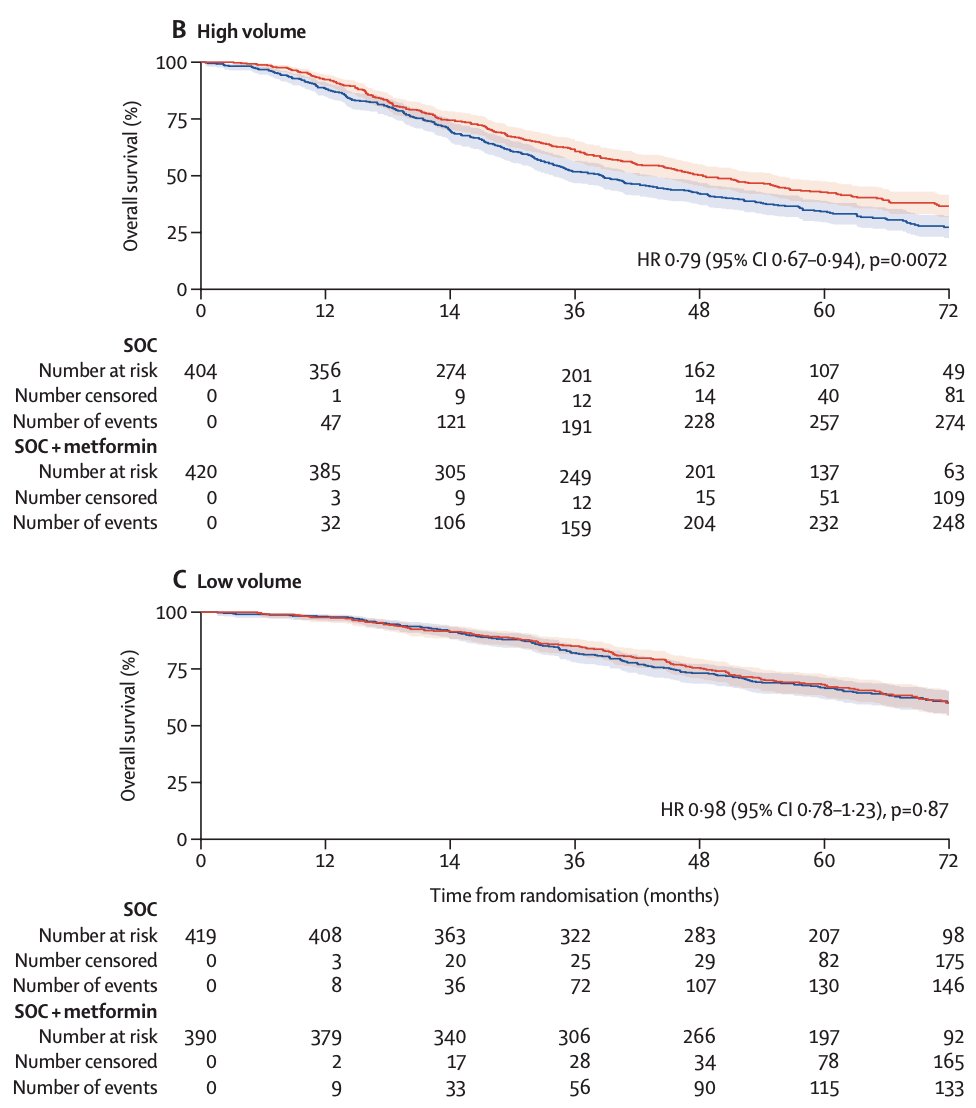
Patients with high volume disease had an improved overall survival with metformin (HR 0.79, 95% CI 0.67-0.94), whereas those with low volume disease had no survival benefit (HR 0.98, 95% CI 0.78-1.23):
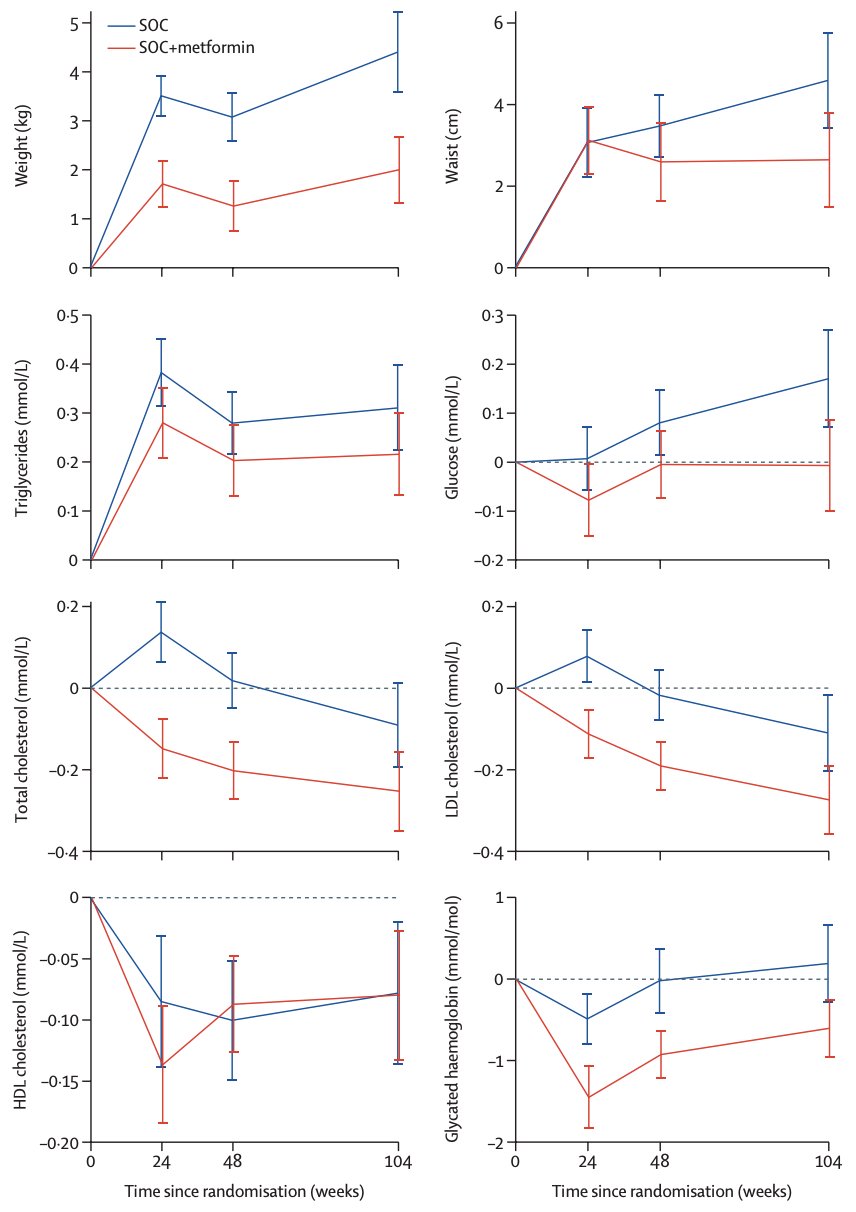
Grade 3 or worse adverse events were reported in 487 (52%) of 938 patients in the standard of care group and 523 (57%) of 921 patients in the standard of care + metformin group. 61 (7%) patients in the standard of care group and 84 (9%) patients in the standard of care + metformin group reported at least one grade 3 or worse gastrointestinal adverse event. The following figures report the morphological (weight) and metabolic (triglycerides, total cholesterol, and HDL cholesterol) outcomes by treatment group, generally favoring the metformin group:
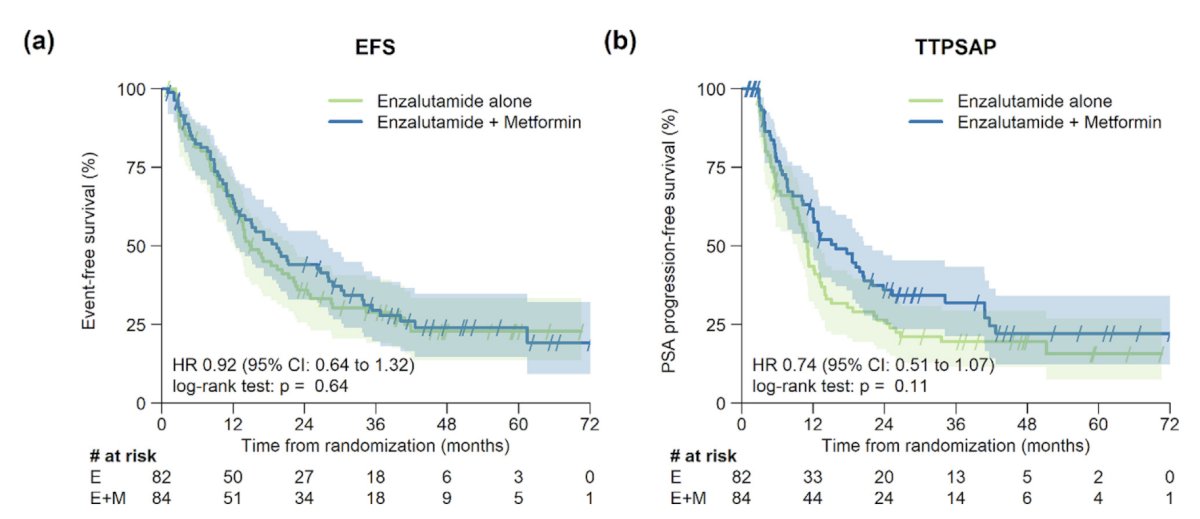
Earlier in 2026, Gillessen et al.2 published results from the SAKK 08/14 phase 2 trial of enzalutamide plus metformin versus enzalutamide alone in mCRPC. The primary endpoint for this trial was the disease control rate at 15 months. Enzalutamide + metformin (n = 84) did not increase disease control compared with enzalutamide alone (n = 82; disease control rate 52% versus 56%, p = 0.64). Additionally, there was no difference in event-free survival (HR 0.92, 95% CI 0.64-1.32) or time to PSA progression (HR 0.74, 95% CI 0.51-1.07):
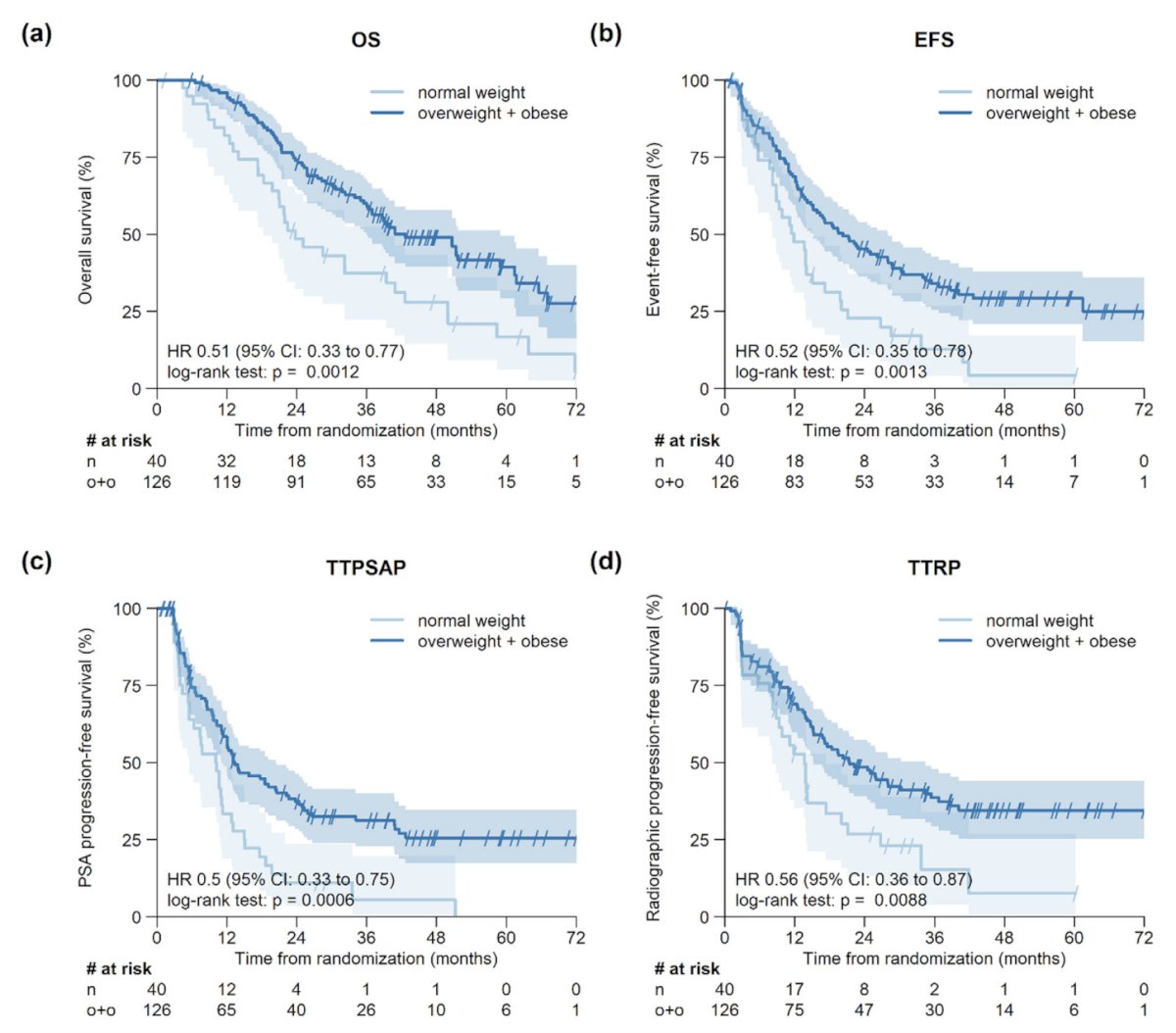
Patients who were overweight/obese at baseline (BMI ≥25 kg/m2) had better disease control rate, overall survival, event-free survival, time to PSA progression, and time to radiographic progression than patients with BMI <25 kg/m2, independent of treatment arm (p < 0.009):
Post hoc analysis suggests that the addition of metformin to enzalutamide may improve time to PSA progression (p = 0.0074) in patients with PTEN-expressing tumors (n = 64), but not in patients with PTEN-negative tumors (n = 65, p > 0.6).
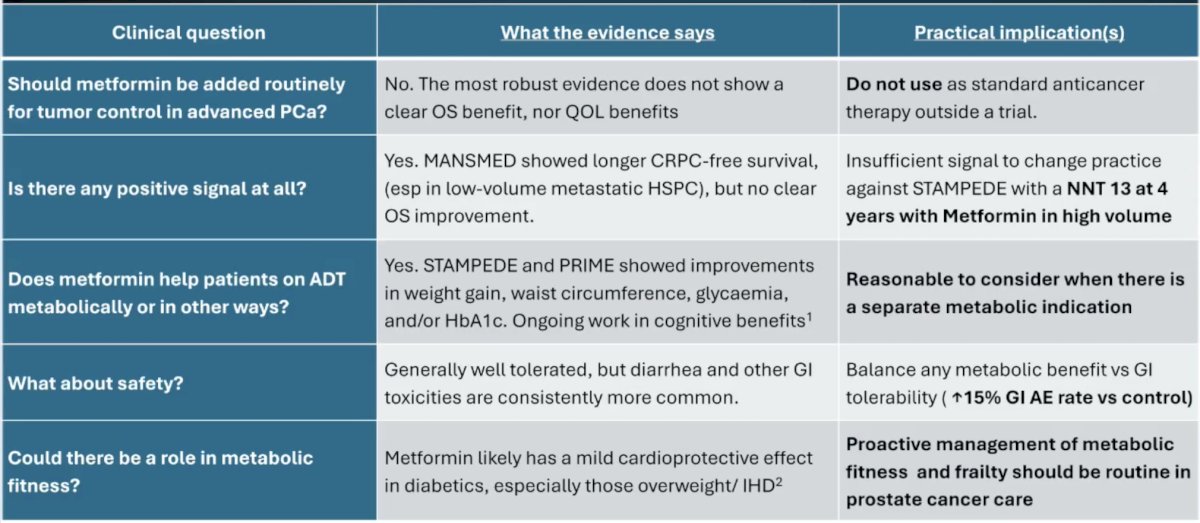
Dr. Joshua emphasized that currently, there are no practice-changing trials in progress assessing metformin in advanced prostate cancer. The following table summarizes the evidence for metformin, with practical implications, for metformin in advanced prostate cancer:
Dr. Joshua concluded his presentation discussing the evidence for using metformin in advanced prostate cancer with the following take-home points:
- Metformin is not routinely warranted in advanced (or early) prostate cancer
- The metabolic benefits of metformin are mild but could be overtaken by studies with SGLT2 and GLP-1 medications that are directly cardio-protective
- 30% of diabetic patients are metformin non-responders
- Even if we accept the STAMPEDE result, albeit not one that was pre-specified, what more, as a community, do we need to do to successfully repurpose a drug for prostate cancer?
- Do we need better endpoints?
- It behooves us as a community to be aware and act proactively to address the effects of ADT and age
Presented by: Anthony Joshua, BSc (Med), MBBS (HONS), PhD, FRACP, St. Vincent’s Clinical School, University of New South Wales, Sydney, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
- Gillessen S, Murphy L, James ND, et al. Metformin for patients with metastatic prostate cancer starting androgen deprivation therapy: A randomized phase 3 trial of the STAMPEDE platform protocol. Lancet Oncol. 2025 Aug;26(8):1018-1030.
- Gillessen S, Gobat K, Cathomas R, et al. Enzalutamide plus metformin versus enzalutamide alone in metastatic castration-resistant prostate cancer: A randomized phase 2 trial (SAKK 08/14). Eur Urol Oncol. 2026 Mar 19 [Epub ahead of print].