(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a monitoring session and a presentation by Dr. Kim Chi discussing whether there is a role for the routine use of ctDNA in advanced prostate cancer. Apoptosing cells shed cell-free DNA (cfDNA) into the blood, and most normal cfDNA is from the blood lineage.
The median fragment length is 167 bp (the unit of the nucleosome), and the average person will have 5-10 ng DNA in 1mL of plasma. In a person with cancer, a fraction of cfDNA is tumor-derived (ctDNA), which is slightly smaller than cfDNA. ctDNA is identified by features absent in blood cfDNA and the germline:
- DNA mutations and structured rearrangements
- Lineage-specific methylation marks
- Lineage-specific nucleosome patterns (fragmentomics)
ctDNA% is related to the volume of active and proliferative cancer.
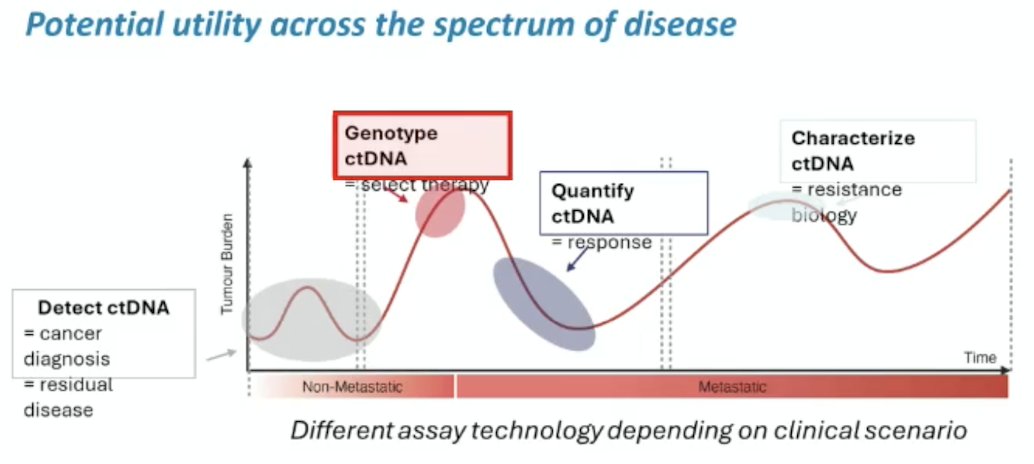
How can ctDNA tests help manage cancer? The primary importance of ctDNA may be in predicting treatment efficacy, with a potential utility across the spectrum of the disease:
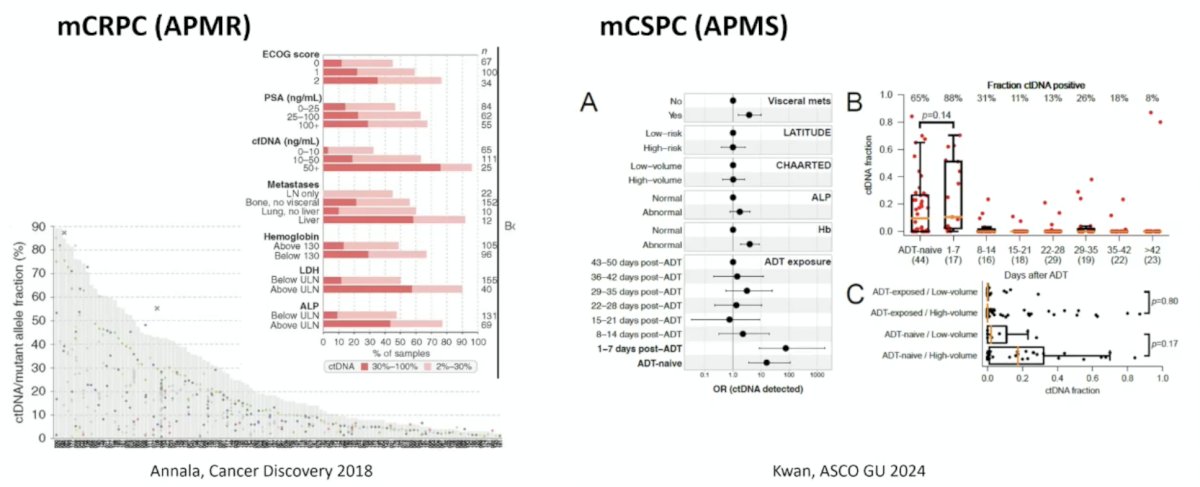
Dr. Chi notes that baseline ctDNA% is variable across mCRPC and mCSPC cohorts:
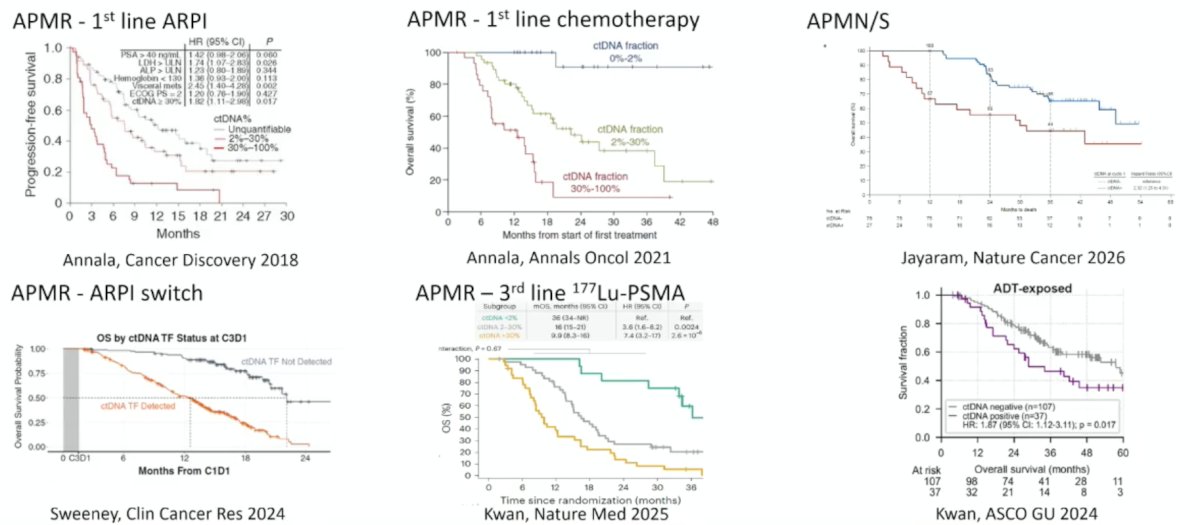
Additionally, across a number of disease spaces, baseline ctDNA% is also prognostic:
ctDNA% change may also potentially be used as a biomarker, predicting non-durable response (<6 months) independent of PSA decline (PPV 88%; NPV 92%):

The potential clinical utility for on-treatment ctDNA% change is as a measure of response for early drug development in conjunction with PSA decline and imaging. A ctDNA% change on treatment may also be an early endpoint in clinical trials, as well as guide treatment decisions: continuation of treatment if discordant PSA and imaging versus early discontinuation, intensification, or change in treatment. The biggest challenge precluding routine use of ctDNA% is that the supporting data for ctDNA in prostate cancer is limited at this time and significant validation is required. Additional challenges include:
- Pre-analytic variability
- Confounders of ctDNA% change are incompletely defined
- The optimal timing and frequency of blood collections
- Analytic variability
- Variety of assays
- Limits of detection and accuracy
- Minimal benchmarking across assays
- Response and progression definitions
- Detectable/undetectable versus increase/decrease versus continuous/categorical
- Timing
- Treatment dependency
- The need for larger datasets and meta-cohorts focused on specific clinical scenarios
- The need for prospective clinical trials with ctDNA% as an integral biomarker
Dr. Chi concluded his presentation discussing whether there is a role for the routine use of ctDNA in advanced prostate cancer with the following take-home points:
- Plasma ctDNA% is typically high in patients with metastatic prostate cancer, correlated with disease burden and aggression, and is independently prognostic
- On treatment changes in ctDNA% are associated with progression-free survival and overall survival, and can provide additional prognostic information beyond PSA declines and imaging
- ctDNA% on treatment kinetics is a promising biomarker for response and as an early endpoint for clinical trials
- We require more correlative data to better define clinically meaningful changes in ctDNA%
Presented by: Kim N. Chi, MD, FRCPC, University of British Columbia, BC Cancer – Vancouver Center, Vancouver, British Columbia, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.