(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a radioligand and radionuclide therapy in advanced prostate cancer session and a presentation by Dr. Michael Morris discussing how to optimally select patients for Lutetium-PSMA radioligand therapy. Dr. Morris stated that his goal for the presentation is to discuss the when, why, and who should be receiving radioligand therapy:
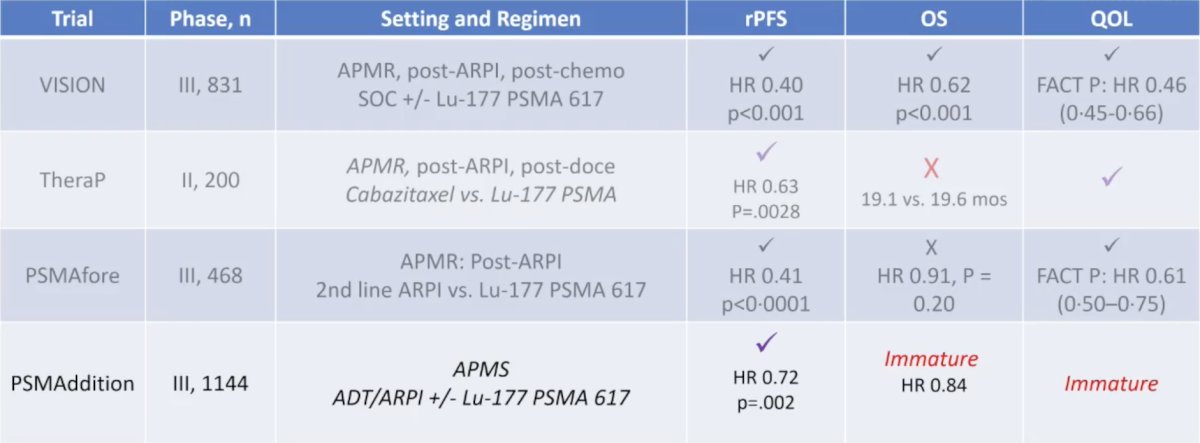
Based on the radiographic progression free survival, overall survival, and quality of life data from the VISION trial,1 APMR patients post-androgen receptor pathway inhibitor and post-taxane chemotherapy should all be strongly considered for 177Lu-PSMA-617 radioligand therapy:

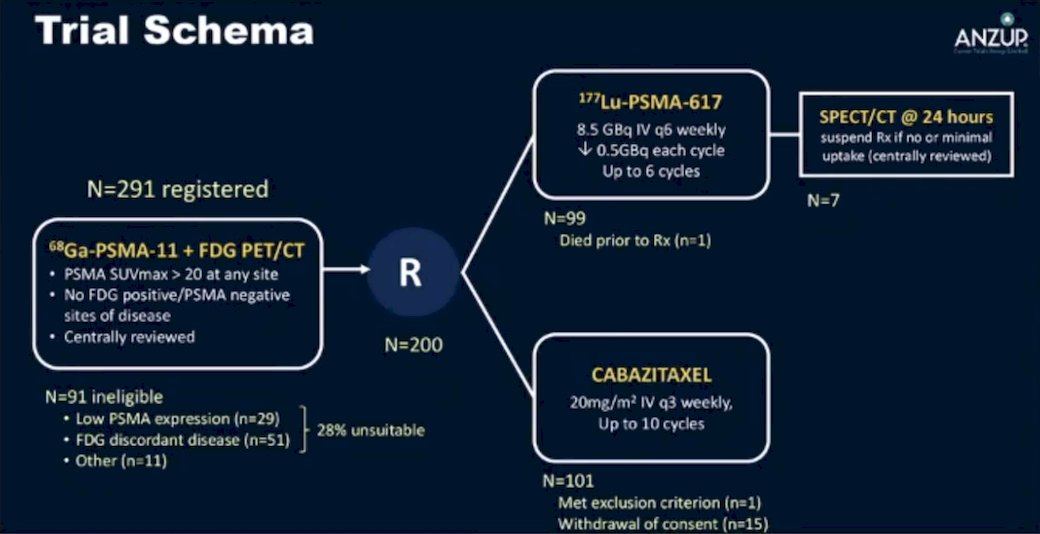
However, VISION had no chemotherapy control, unlike TheraP.2 The TheraP trial was the first randomized study to evaluate 177Lu-PSMA-617 versus cabazitaxel for men with APMR after docetaxel. In this open-label, phase II trial, 200 men were randomized to either 177Lu-PSMA-617 or cabazitaxel. To screen into the study, all men had both 68Ga-PSMA-11 and 18F-FDG PET/CT and were required to have high PSMA-expression (at least one site with SUVmax ≥ 20) and no sites of FDG-positive/PSMA-negative disease. All patients had progressive disease with rising PSA ≥ 20 ng/mL after docetaxel, and 91% had received prior enzalutamide or abiraterone. Overall, 200 patients were randomized 1:1 to 177Lu-PSMA-617 6-8 GBq every 6 weeks for up to 6 cycles of therapy or cabazitaxel 20 mg/m2 every 3 weeks for up to 10 cycles. Patients were stratified based on disease burden and prior anti-androgen therapy. The trial schema for TheraP is as follows:
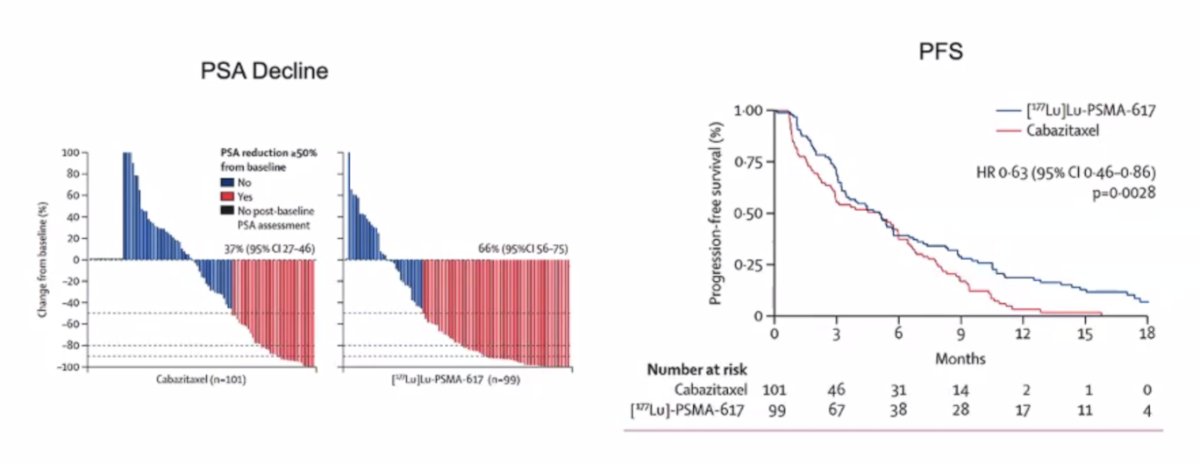
After a median follow-up of 13 months, 177Lu-PSMA-617 significantly improved PSA progression-free survival compared with cabazitaxel (HR 0.63, 95% CI 0.46 to 0.86) and a had a much higher PSA50 rate (66% vs 37%):
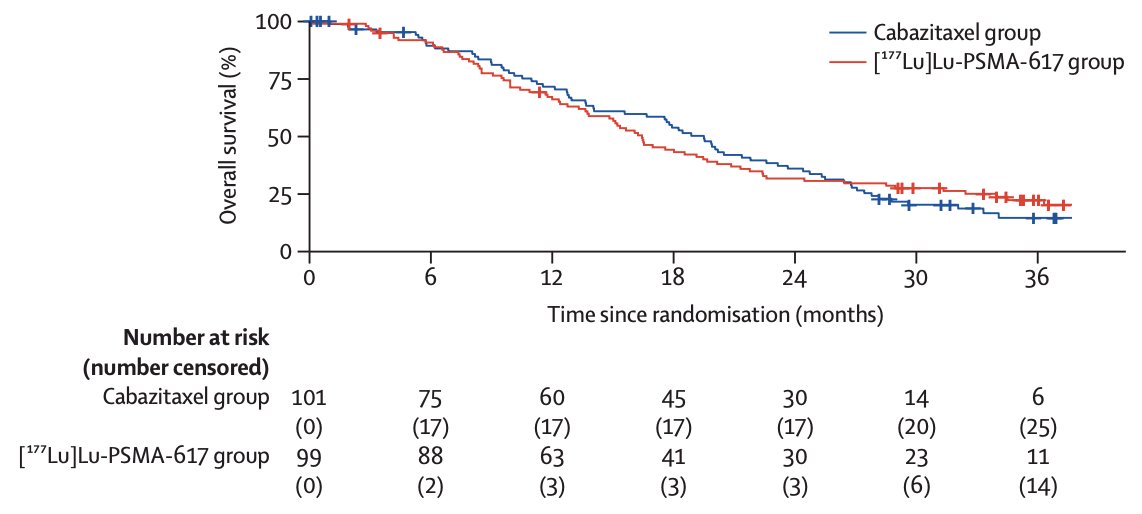
Subsequently, Hofman and colleagues3 noted that after a median follow-up of 35.7 months (IQR 31.1 to 39.2), 77 (78%) participants had died in the 177Lu-PSMA-617 group and 70 (69%) participants had died in the cabazitaxel group. Overall survival was similar among those assigned to 177Lu-PSMA-617 versus those assigned to cabazitaxel (restricted mean survival time 19.1 months vs 19.6; difference -0.5 months; p = 0.77):
Patient-reported outcomes also overwhelmingly favor the 177Lu-PSMA-617 group compared to cabazitaxel:

Thus, based on TheraP, Dr. Morris notes that patients are living better with 177Lu-PSMA-617 than with cabazitaxel.
PSMAfore,4 assessing 177Lu-PSMA-617 in APMR post androgen receptor pathway inhibitor but before taxane chemotherapy demonstrated a radiographic progression-free survival benefit, but no overall survival benefit (which may be secondary to the 84.2% crossover to 177Lu-PSMA-617 in the control arm):

Does the sequence of 177Lu-PSMA-617 impact overall survival? The CCTG PR21 trial was an open-label, randomized, phase II trial that allowed for crossover between the two study arms. The key eligibility criteria were as follows:
- Chemotherapy-naïve APMR progressing after an androgen receptor pathway inhibitor
- PSMA PET positive disease (ie, uptake >liver)
- Patients were excluded if >50% of extra-osseous lesions, or >5 cm soft tissue lesions were PSMA negative
- Adequate end-organ function
- Prior docetaxel for APMS permitted if ≥12 months prior
Eligible patients were randomized 1:1 to:
- 177Lu-PSMA-617 7.4 GBq IV every 6 weeks x 6 cycles
- Docetaxel 75 mg/m2 every 3 weeks x 12 cycles

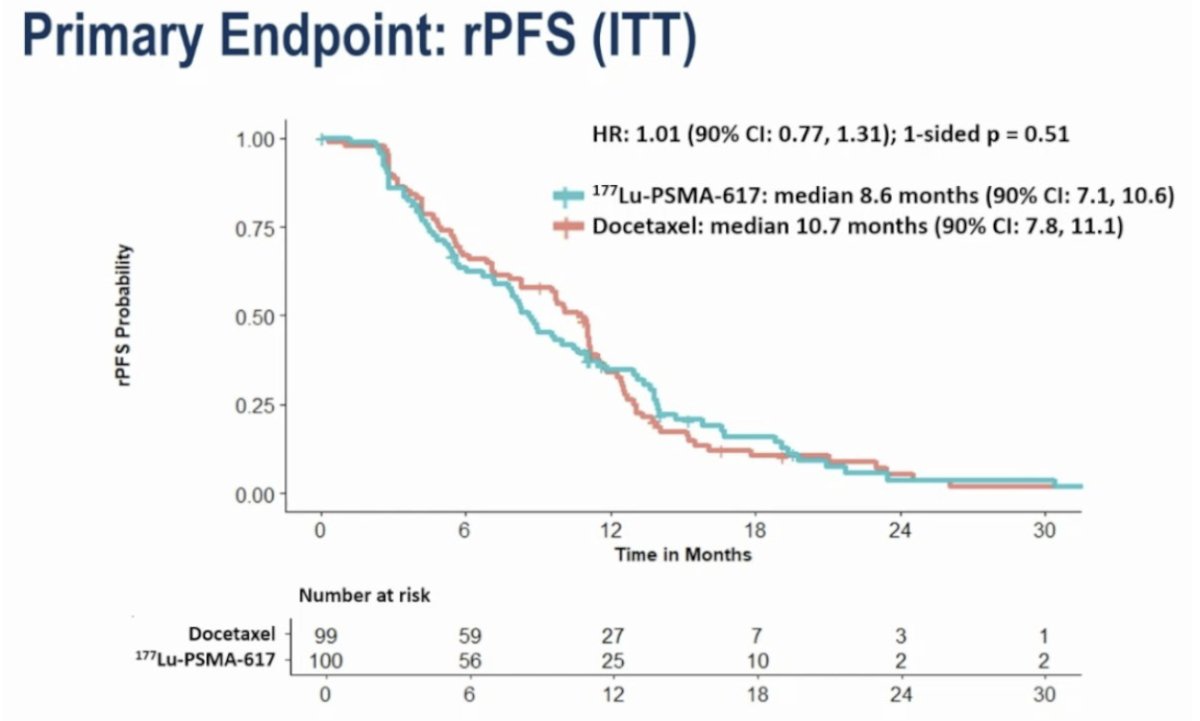
There was no difference in radiographic progression-free survival between the two arms. The median radiographic progression-free survival values were 8.6 and 10.7 months for the 177Lu-PSMA-617 and docetaxel arms, respectively (HR 1.01, 95% CI 0.77–1.31, p = 0.51).
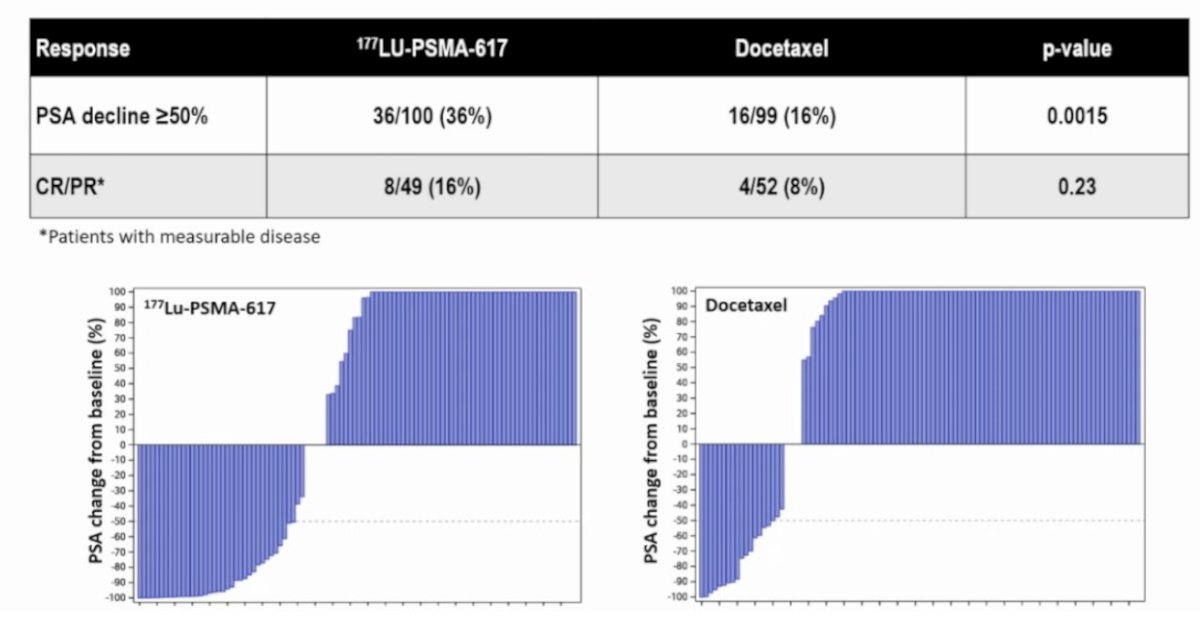
Disease response rates favored 177Lu-PSMA-617:
- PSA50 response: 36% versus 16% (p = 0.0015)
- Complete or partial response: 16% versus 8% (p = 0.23)
Overall survival also favored patients initially randomized to the docetaxel arm (HR 1.64, 95% CI 1.14–2.35, p = 0.02). The median overall survival was 14.3 and 18.2 months, respectively, in favor of initial randomization to docetaxel (ie, docetaxel followed by 177Lu-PSMA-617):

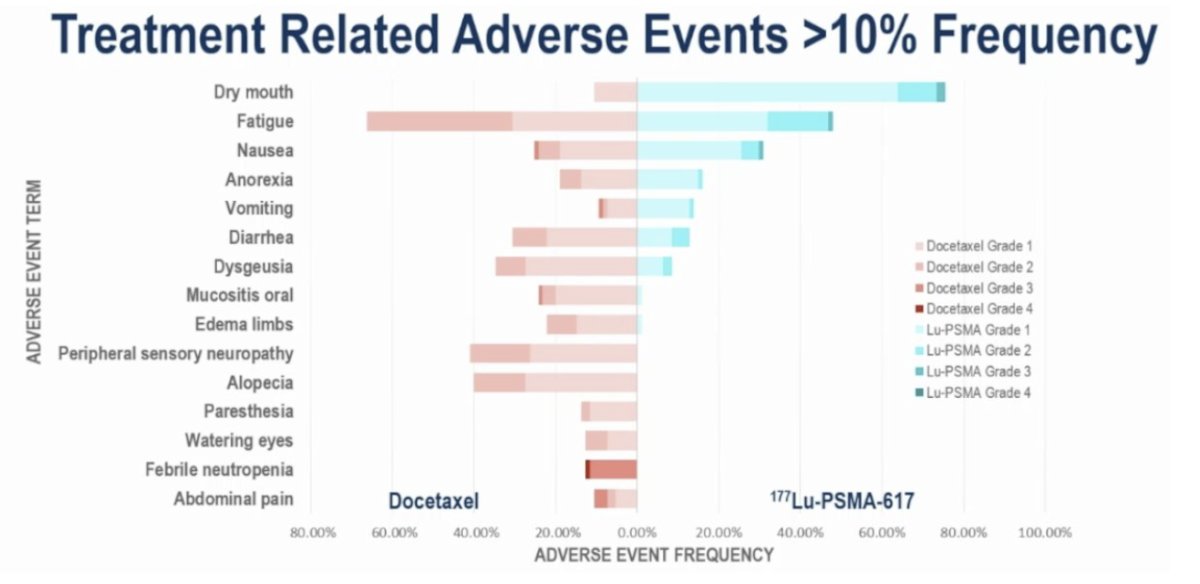
Grade 3-4 treatment-related adverse events were more common in the docetaxel arm (34% versus 13%). Two treatment-related deaths were observed (sepsis, not otherwise specified), both in the docetaxel arm. The most common adverse events in either arm were as expected for both treatments:
When assessing VISION + TheraP + PSMAfore + PR21 for APMR, 177Lu-PSMA-617 had superior quality of life than:
- Second-line androgen receptor pathway inhibitor in PSMAfore
- First-line chemotherapy in PR21
- Second-line chemotherapy in TheraP
- Supportive measures in VISION, with a clear overall survival advantage in the post-androgen receptor pathway inhibitor/post-taxane disease space
With regards to APMS and the PSMAddition trial, this was a positive trial with a benefit in radiographic progression-free survival (HR 0.72, p = 0.002), with immature data for overall survival and quality of life:
What about pre- or post-PARP inhibitors for DNA repair defects? PSMAfore excluded patients eligible for PARP inhibitors who had not received one, and currently, there is no high-quality data suggesting that HRR-deficient patients are better responders to radioligand therapy than to PARP inhibitors.
ctDNA looks like a good predictor of response for radioligand therapy based on work from TheraP. Kwon et al5 assessed prostate cancer driver genes across 290 serial plasma cell-free DNA samples from 180 molecular imaging-selected patients with APMR.6 A low (ctDNA <2%) pretreatment ctDNA fraction predicted a superior progression-free survival and overall survival compared to higher (ctDNA 2-30% and >30%) pretreatment ctDNA fractions:
![ctDNA looks like a good predictor of response for radioligand therapy based on work from TheraP. Kwon et al [5] assessed prostate cancer driver genes across 290 serial plasma cell-free DNA samples from 180 molecular imaging-selected patients with APMR [6]. A low (ctDNA <2%) pretreatment ctDNA fraction predicted a superior progression-free survival and overall survival compared to higher (ctDNA 2-30% and >30%) pretreatment ctDNA fractions:](/images/com-doc-importer/262-apccc-2026/apccc-2026-how-to-optimally-select-patients-for-lutetium-psma-radioligand-therapy/image-13.jpg)
To explore the association between quantitative baseline 68Ga-PSMA-11 PET/CT parameters and treatment response and outcomes in the VISION trial, Kuo et al. found that whole-body tumor SUVmean was the best predictor of 177Lu-PSMA-617 efficacy, with an HR range of 0.86-1.43 for all outcomes (all p < .001).6 A 1-unit whole-body tumor SUVmean increase was associated with a 12% and 10% decrease in risk of a radiographic progression-free survival event and death, respectively. Higher baseline PSMA-positive tumor volume and tumor load were associated with worse radiographic progression-free survival (HR range, 1.44-1.53 [p < 0.05] and 1.02-1.03 [p < 0.001], respectively) and overall survival (HR range, 1.36-2.12 [p < 0.006] and 1.04 [p < 0.001], respectively):
![To explore the association between quantitative baseline 68Ga-PSMA-11 PET/CT parameters and treatment response and outcomes in the VISION trial, Kuo et al. found that whole-body tumor SUVmean was the best predictor of 177Lu-PSMA-617 efficacy, with an HR range of 0.86-1.43 for all outcomes (all p < .001) [6]. A 1-unit whole-body tumor SUVmean increase was associated with a 12% and 10% decrease in risk of a radiographic progression-free survival event and death, respectively. Higher baseline PSMA-positive tumor volume and tumor load were associated with worse radiographic progression-free survival (HR range, 1.44-1.53 [p < 0.05] and 1.02-1.03 [p < 0.001], respectively) and overall survival (HR range, 1.36-2.12 [p < 0.006] and 1.04 [p < 0.001], respectively):](/images/com-doc-importer/262-apccc-2026/apccc-2026-how-to-optimally-select-patients-for-lutetium-psma-radioligand-therapy/image-14.jpg)
Dr. Morris concluded his presentation discussing how to optimally select patients for Lutetium-PSMA radioligand therapy with the following take-home points:
- Post-androgen receptor pathway inhibitor and post-chemotherapy – unquestionably beneficial
- Post-androgen receptor pathway inhibitor, better quality of life – unclear overall survival advantage, but better quality of life than other standards of care
- APMS – Too early to tell
- Regarding HRR mutations, especially BRCA – leverage the genomically directed therapy first
- Patients who are most likely to respond are those with:
- For predicting overall survival, we do not have a good predictive biomarker specifically for radioligand therapy
Presented by: Michael J. Morris, MD, Prostate Cancer Section Head, GU Oncology, Steven A. Greenberg Chair in Prostate Cancer Research, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.
- Hofman MS, Emmett L, Sandhu S, et al. Overall survival with [177Lu]Lu-PSMA-617 versus cabazitaxel in metastatic castration-resistant prostate cancer (TheraP): Secondary outcomes of a randomized, open-label, phase 2 trial. Lancet Oncol. 2024 Jan;25(1):99-107.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.
- Kwan EM, Ng SWS, Tolmeijer SH, et al. Lutetium-177-PSMA-617 or cabazitaxel in metastatic prostate cancer: circulating tumor DNA analysis of the randomized phase 2 TheraP trial. Nat Med. 2025 Aug;31(8):2722-2736.
- Kuo PH, Morris MJ, Hesterman J, et al. Quantitative 68Ga-PSMA-11 PET and Clinical Outcomes in Metastatic Castration-resistant prostate cancer following 177Lu-PSMA-617 (VISION Trial). Radiology. 2024 Aug;312(2):e233460.