(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a radioligand and radionuclide therapy in advanced prostate cancer session and a presentation by Dr. Daniel Heinrich discussing how to optimally select patients for radionuclide therapy with radium-223. In general, patient selection is via biomarkers, clinical scenario, patient individual factors, and health care system factors. Currently, there are no biomarkers for selecting patients for radium-223, including no genomic/genetic biomarkers, no circulating biomarkers, and no radiologic/radiographic biomarkers. DNA repair/HRR deficiency has been proposed as a biomarker, but there are very limited numbers, and studies are retrospective and single institutional. Dr. Heinrich notes that, at best, this is hypothesis generating data, and we already have targeted therapies for these patients.
However, there are biomarkers to exclude patients from radium-223 therapy. This includes a complete lack of Technetium uptake on bone can (and maybe superscans too), as well as significant visceral metastasis on imaging.
The ALSYMPCA trial was published in 2013 and was a phase 3, randomized, double-blind, placebo-controlled trial that randomized 921 patients in a 2:1 fashion to receive six injections of radium-223 (at a dose of 50 kBq per kilogram of body weight intravenously) or matching placebo.1 All patients received additional best standard of care. Of note, patients could have received prior docetaxel (57% of included patients). Patients receiving radium-223 had significantly improved median overall survival (14.9 versus 11.3 months; HR 0.70, 95% CI 0.58 to 0.83):
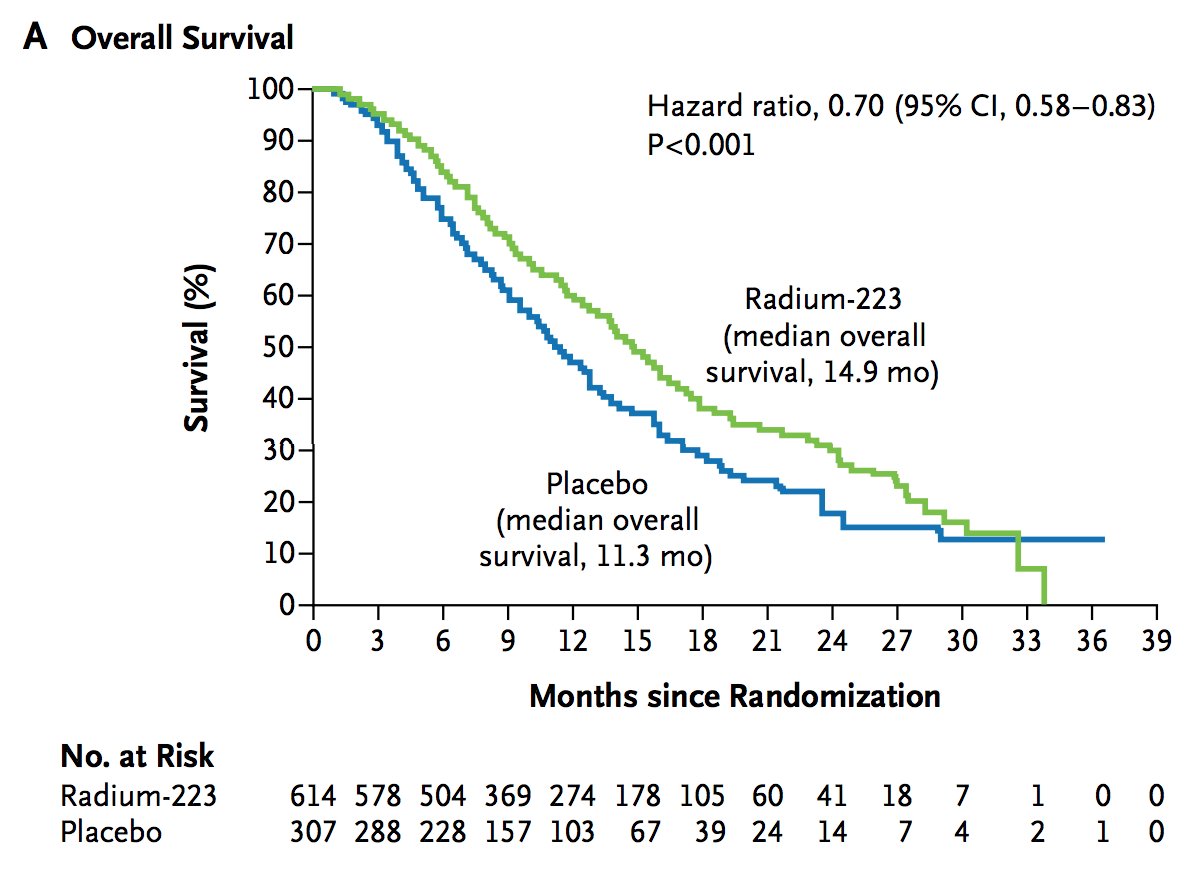
Dr. Heinrich notes that ALSYMPCA was before the androgen receptor pathway inhibitor era, and was a last line mCRPC study at that time. Importantly, the overall survival benefit noted in ALSYMPCA aligned with results from other later line mCRPC trials, including TROPIC2 (cabazitaxel versus mitoxantrone; HR 0.70, 95% CI 0.59-0.83), CARD3 (cabazitaxel versus androgen signaling targeted inhibitor; HR 0.64, 95% CI 0.46-0.89), PROfound4 (olaparib versus control; HR 0.79, 95% CI 0.61-1.03), and VISON5 (177Lu-PSMA-617 versus standard of care; HR 0.62, 95% CI 0.52-0.74).
Is sequencing an issue, and does the sequence matter? Dr. Heinrich notes that it is important to find the individual sequence that’s best for each patient and that includes most life prolonging therapies, rather than trying to find the “one magic best sequence.” Radium-223 before or after docetaxel is feasible, radium-223 before or after 177Lu-PSMA-617 is feasible, and any sequencing with PARP inhibitors seems feasible as well. There is no concern to include radium-223 anywhere in a sequence of life prolonging therapies for mCRPC.
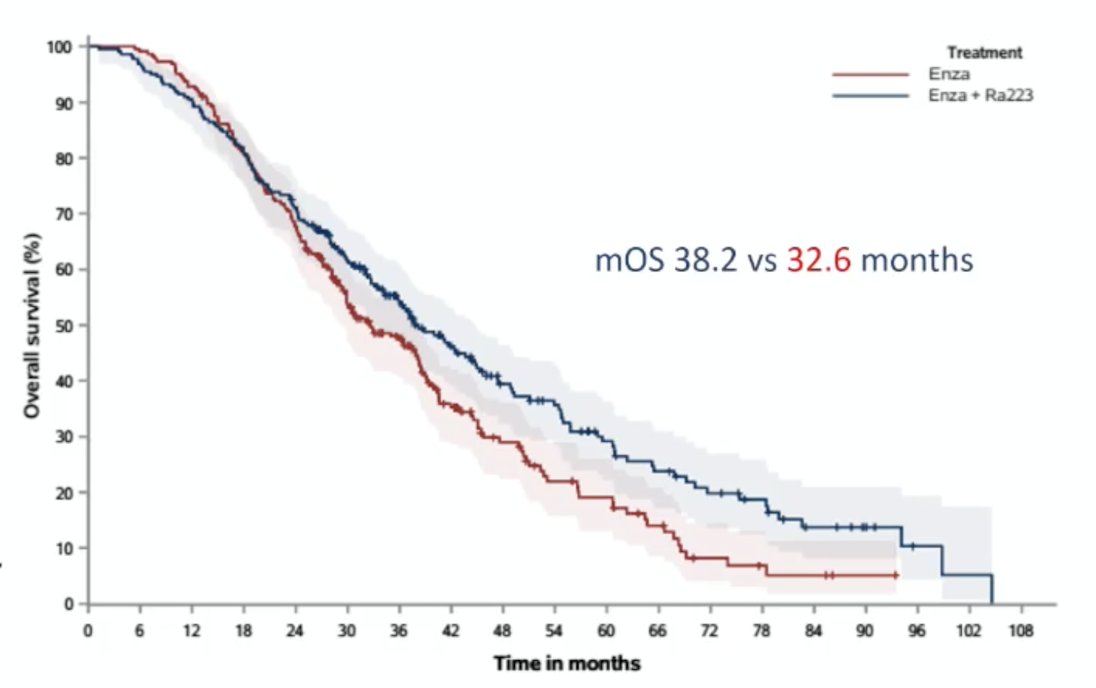
Another clinical scenario where radium-223 may useful is in the PEACE-3 setting. PEACE-3 is the second phase III radium-223 trial to demonstrate an overall survival benefit.6
This was a randomized, open-label, multicenter phase III trial evaluating the addition of radium-223 to enzalutamide in mCRPC with bone metastases. In PEACE-3, a total of 446 asymptomatic or mildly symptomatic patients (Brief Pain Inventory <4) with mCRPC and ≥2 bone metastases were randomized 1:1 to enzalutamide 160 mg daily alone or combined with six intravenous injections of radium-223 (55 kBq/kg every 4 weeks). The median overall survival was 38.2 months for enzalutamide + radium 223 and 32.6 months for enzalutamide alone, corresponding to a hazard ratio of 0.76 (95% CI 0.60–0.96; one-sided stratified log rank p-value 0.0096, with a preset level of significance at final analysis of < 0.0248). Based on the permutation test, the statistical test on overall survival is significant (resulting in a 1-sided p-value of 0.0088 < 0.0248):
Dr. Heinrich notes that based on his clinical practice, androgen receptor pathway inhibitor naïve first line mCRPC patients still exist, estimating ~10% in his practice in Norway.
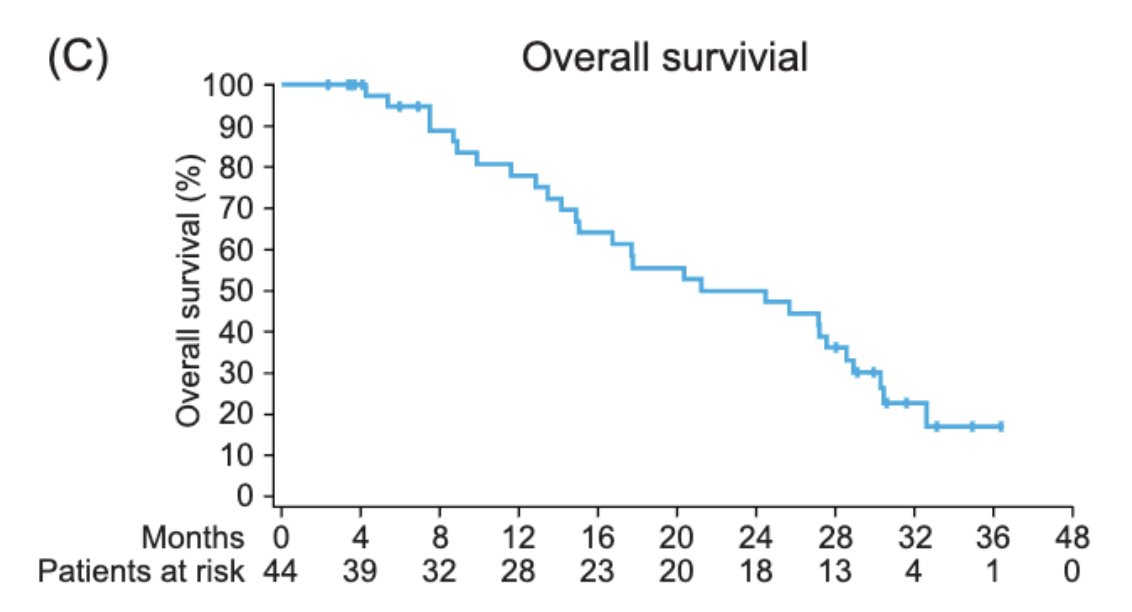
A final clinical scenario for using radium-223 is in the retreatment setting. In 2019, Dr. Sartor and colleagues [7] evaluated the safety and efficacy findings from 2-year follow-up of the radium-223 re-treatment. Among 44 patients re-treated with radium-223, 29 (66%) completed all 6 injections, and 34 (77%) entered 2-year active follow-up, during which no new safety concerns and no serious drug-related adverse events were noted. Radiographic progression free survival occurred in 19 (43%) of 44 patients, with a median radiographic progression free survival of 9.9 months. The median overall survival was 24.4 months:
There are also patient individual factors that may assist with selecting a patient for radium-223, including those that do not want chemotherapy, those with comorbidities that exclude them from other options, and patients with remaining side effects from earlier treatment lines. Dr. Heinrich also cautions that we cannot forget bone protecting agents, no matter how a patient was selected for radium-223 therapy. This includes adding bisphosphonates or denosumab, and if there is time, we should consider administering 1-2 doses before the first cycle of radium-223.
Dr. Heinrich concluded his presentation discussing how to optimally select patients for radionuclide therapy with radium-223 with the following take-home points:
- There are currently no biomarkers for selecting patients for radium-223
- We should use radium-223 as a part of a sequence of life prolonging therapies (ALSYMCA indication)
- First line mCRPC radium-223 in combination with enzalutamide is a “no brainer” for androgen receptor pathway inhibitor naive patients
- Re-treatment is feasible in selected patients
- We must use bone protecting agents whenever using radium-223
Presented by: Daniel Heinrich, MD, Innlandet Hospital Trust, Gjøvik, Norway
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
Related content: Clinical Scenario and Patient Preference Guide Radium-223 Use in mCRPC - Daniel Heinrich
References:
- Parker C, Nilsson S, Heinrich D, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med 2013;369(3):213-223.
- de Bono JS, Oudard S, Ozguroglu M, et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: A randomised open-label trial. Lancet 2010;376(9747):1147-1154.
- de Wit R, de Bono J, Sternberg CN, et al. Cabazitaxel versus Abiraterone or Enzalutamide in Metastatic Prostate Cancer. N Engl J Med 2019 Dec 26;381(26):2506-2518.
- de Bono J, Mateo J, Fizazi K, et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med 2020 May 28;382(22):2091-2102.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Tombal B, Choudhury A, Saad F, et al. Enzalutamide plus radium-223 in metastatic castration-resistant prostate cancer: results of the EORTC 1333/PEACE-3 trial. Ann Oncol. 2025 Sep;36(9):1058-1067.
- Sartor O, Heinrich D, Mariados N, et al. Re-treatment with radium-223: 2-year follow-up from an international, open-label, phase 1/2 study in patients with castration-resistant prostate cancer and bone metastases. Prostate. 2019 Oct;79(14):1683-1691.