(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a radioligand and radionuclide therapy in advanced prostate cancer session and a presentation by Dr. Michael Hofman discussing PSMA combination strategies beyond monotherapy. Dr. Hofman started his presentation by discussing the TheraP trial, which was the first randomized study to evaluate 177Lu-PSMA-617 versus cabazitaxel for men with metastatic castration resistant prostate cancer (mCRPC) after docetaxel. In this open label, phase II trial, 200 men were randomized to either 177Lu-PSMA-617 or cabazitaxel. To screen into the study, all men had both 68Ga-PSMA-11 and 18F-FDG PET/CT and were required to have high PSMA-expression (at least one site with SUVmax ≥ 20) and no sites of FDG-positive/PSMA-negative disease:


All patients had progressive disease with rising PSA ≥ 20 ng/mL after docetaxel, and 91% had received prior enzalutamide or abiraterone. Overall, 200 patients were randomized 1:1 to 177Lu-PSMA-617 6-8 GBq every 6 weeks for up to 6 cycles of therapy or cabazitaxel 20 mg/m2 every 3 weeks for up to 10 cycles. Patients were stratified based on disease burden and prior anti-androgen therapy.
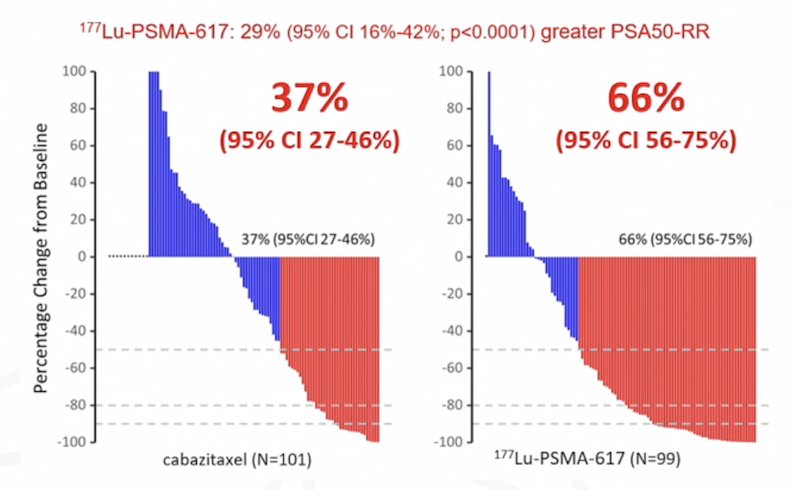
The primary endpoint of this study was a PSA decline of 50% (PSA50), and secondary endpoints included PSA progression free survival and overall survival. After a median follow up of 13 months, 177Lu-PSMA-617 significantly improved PSA progression free survival compared with cabazitaxel (HR 0.63, 95% CI 0.46 to 0.86) and had a much higher PSA50 rate (66% versus 37%):
According to RECIST 1.1, the objective response rate was 24% for cabazitaxel compared to 49% for 177Lu-PSMA-617:

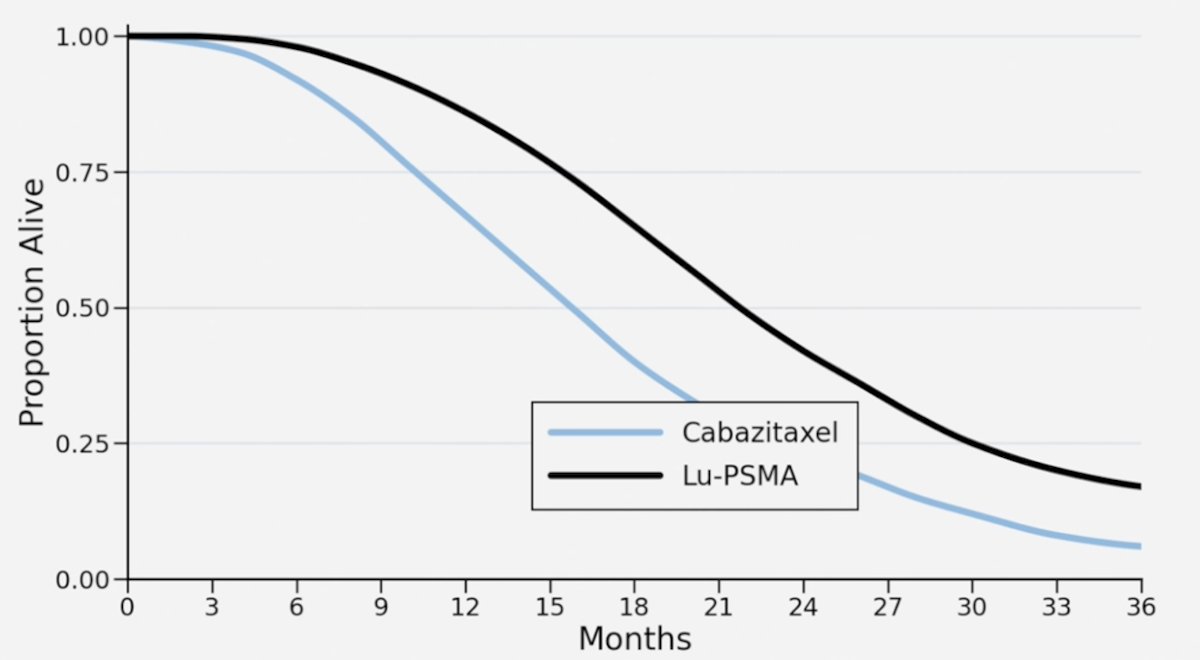
Based on these PSA and RECIST responses, Dr. Hofman states that they expected the overall survival curve for TheraP to look like this.
But what they found was that there was no overall survival benefit for 177Lu-PSMA-617 versus cabazitaxel:
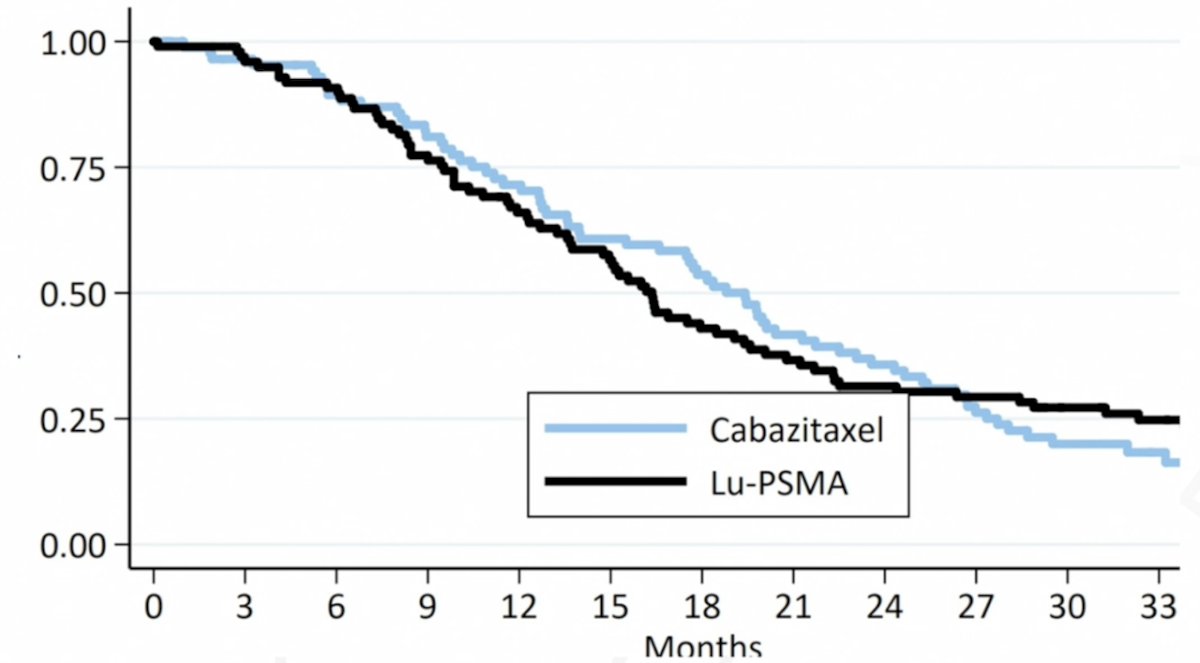
Tumor targeted 177Lu-PSMA-617 is very effective in tumor mass shrinkage and decreases PSA; it may be less effective at stopping new metastases, which is where taxane based chemotherapy may be much better than 177Lu-PSMA-617:

In addition to monotherapy 177Lu-PSMA-617, Dr. Hofman stated that there are many combination theranostics with PSMA, including hormone therapy, chemotherapy, immunotherapy, PARP inhibitors, radioligand therapy, surgery, and external beam radiotherapy:

The ENZA-p trial2 assessed 177Lu-PSMA-617 + enzalutamide versus enzalutamide monotherapy. The impetus for this study is that enzalutamide has been shown to upregulate expression of PSMA on subsequent imaging. ENZA-p included mCRPC patients not previously treated with chemotherapy or androgen receptor pathway inhibitors (prior abiraterone and/or docetaxel for hormone-sensitive disease were allowed), 68Ga-PSMA1-positive disease on PET, and at least 2 risk factors associated with early progression on enzalutamide. In the enzalutamide + 177Lu-PSMA-617 arm, 81% of patients received four doses of 177Lu-PSMA-617. PSA50 and PSA90 improved with 177Lu-PSMA-617 + enzalutamide. Over a median follow up of 20 months (IQR 18-21), PSA progression free survival was longer with enzalutamide + 177Lu-PSMA-617 vs enzalutamide-alone (median 13 vs 7.8 months; HR 0.43, 95% CI 0.29-0.63, p < 0.001). There was also a trend towards improved radiographic progression free survival, favoring 177Lu-PSMA-617 (HR 0.68, 95% CI 0.45-1.03):

A total of 96 deaths were reported after a median follow-up of 34 months (IQR 29-39): 53 among those assigned enzalutamide-alone and 43 among those assigned enzalutamide + 177Lu-PSMA-617. Overall survival was longer in the enzalutamide + 177Lu-PSMA-617 group than the enzalutamide-alone group: median 34 months versus 26 months (HR 0.55, 95% CI 0.36 to 0.84; p = 0.005):3

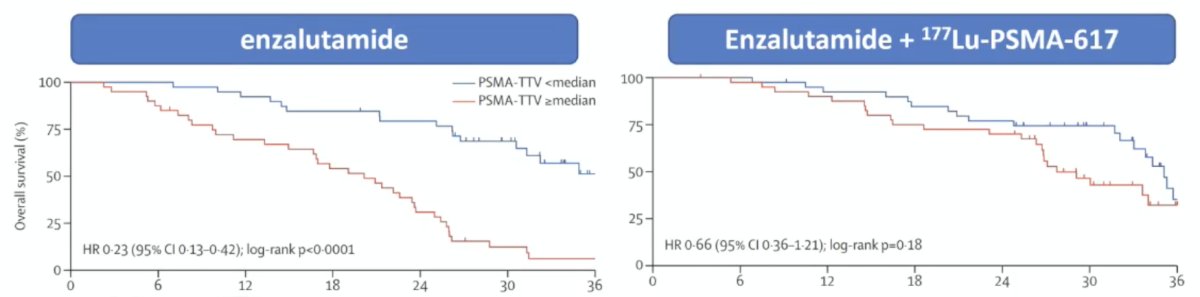
Total tumor volume in ENZA-p was noted to be predictive for the benefit of adding 177Lu-PSMA-617:
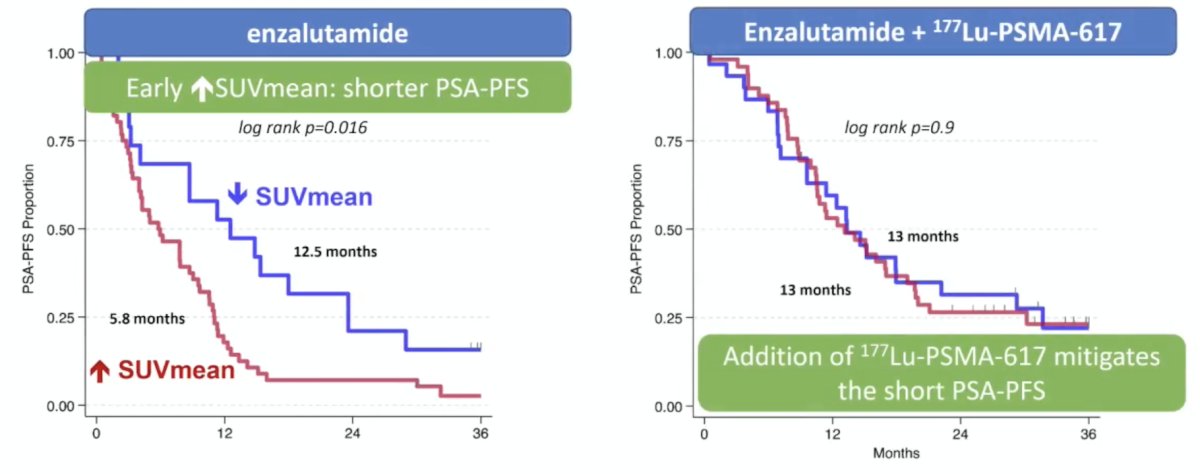
Published earlier in 2026, Emmett et al.4 evaluated the predictive value of early PSMA upregulation for the response to enzalutamide +/- 177Lu-PSMA-617 among patients in ENZA-p. The median PSA progression free survival with increasing SUV mean at day 15 was 5.8 (95% CI 4.0-8.7) versus 13.1 (95%CI 10.5-17.0) months for enzalutamide versus enzalutamide + 177Lu-PSMA-617 (HR 0.38, 95%CI 0.25-0.58). With decreasing SUV mean, the median PSA progression free survival was 12.5 (95%CI 3.2-23.6) versus 13.3 (95%CI 9.6-22.2) months for enzalutamide versus enzalutamide + 177Lu-PSMA-617 (HR 0.80, 95%CI 0.42-1.53). The interaction between SUV mean increase or decrease, and treatment arm for PSA progression free survival was p = 0.055. Thus, the addition of 177Lu-PSMA-617 to enzalutamide mitigated the short PSA progression free survival in those with early PSMA SUV mean increase:
Dr. Hofman then discussed PARP inhibitors as a radiosensitizer for 177Lu-PSMA-617, with the following schematic:

The combination trial for 177Lu-PSMA-617 + PARP inhibitors is the LuPARP trial, which is a phase I trial of 177Lu-PSMA-617 and olaparib with the following trial schema:

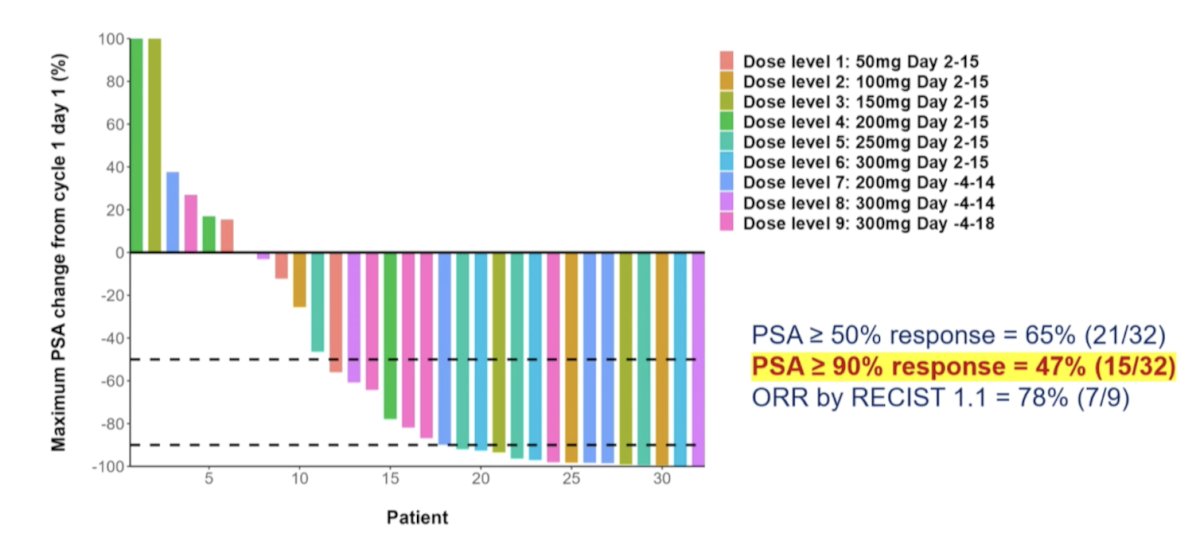
For treatment-related adverse events, no dose limiting toxicities were reported across the dose levels, and there were no grade 4 adverse events. One treatment-related serious adverse event occurred (febrile neutropenia), and dose delay due to hematological toxicity occurred in 3 (9%) patients (cohorts 2, 5, and 6). Dose reduction was required in 4 patients (12%), with 3 due to hematological toxicity and 1 due to xerostomia. The recommended phase 2 dose was 7.4 Gb of 177Lu-PSMA-617 in conjunction with olaparib 300 mg twice daily on days -4 to 18 of each 6 weekly cycle. In the overall cohort (i.e., Cohorts 1 to 9), the PSA50 and PSA90 response rates were 65% and 47%, respectively, and the objective response rate by RECIST v1.1 criteria was 78%:
Next, Dr. Hofman discussed the LuCAB trial, which was designed to assess whether cabazitaxel combined with 177Lu-PSMA-617 could improve response rates and durability of treatment in patients with mCRPC. The LuCAB phase I/II trial is a single center, ongoing trial combining 177Lu-PSMA-617 up to six cycles with cabazitaxel up to 12 doses, with cabazitaxel dose escalation:

The primary objective was assessing the maximal tolerated dose of cabazitaxel and 177Lu-PSMA-617, with secondary objectives including adverse events, PSA50, response rate, radiographic progression free survival, PSA progression free survival, overall survival, objective response rate, and evaluation of pain and health-related quality of life. Results for LuCAB are expected at the end of 2026.
Dr. Hofman then discussed the PRINCE trial, which is a phase 1b/2 trial of 177Lu-PSMA-617 in combination with pembrolizumab in mCRPC.5 Among 37 patients, they received a median of 4 cycles of 177Lu-PSMA-617 and 8 doses of pembrolizumab. Treatment-related adverse events (>=10%) were low grade (1-2) and included xerostomia (76%), fatigue (43%), nausea (24%), rash (22%), pruritus (19%), elevated ALT (11%), diarrhea (11%), and bone pain (11%). The PSA50 response was 76% and the PSA90 response was 46%:

Deep PSA response (PSA90) was seen regardless of PSMA total tumor volume, and more commonly with SUVmean >= 10 (63%). Additionally, tumor mutational burden was generally low, and PSA90 was noted irrespective of tumor mutational burden. One patient with biallelic loss of MSH2 and high tumor mutational burden had a 99.9% PSA decline.
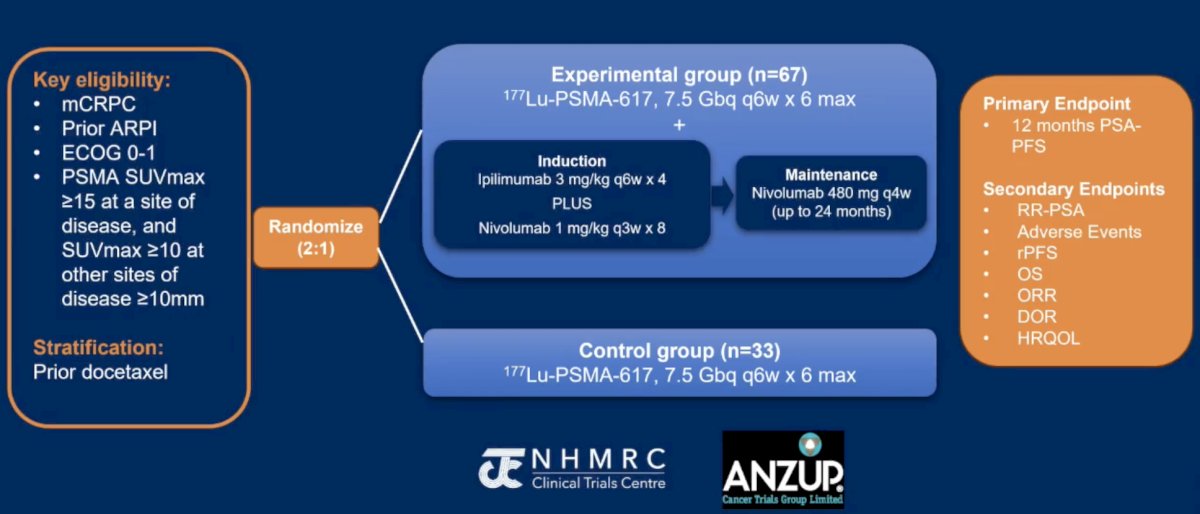
The hypothesis of the EVOLUTION trial is that the combination of a radionuclide (177Lu-PSMA-617) and immune checkpoint inhibitors (ipilimumab and nivolumab) may act synergistically, whereby 177Lu-PSMA-617 may induce immunogenic cell death enhancing the clinical efficacy of ipilimumab/nivolumab, leading to improved long-term clinical outcomes. EVOLUTION will randomize 100 patients in a 2:1 fashion to either the intervention arm of 177Lu-PSMA-617 7.5 GBq every 6 weeks for up to 6 doses plus ipilimumab 3 mg/kg every 6 weeks x 4 doses and nivolumab 1 mg/kg every 3 weeks x 8 doses during induction, followed by nivolumab 480 mg every 4 weeks x 18 doses during maintenance or 177Lu-PSMA-617 alone. The primary endpoint is 12-month PSA progression-free survival. The trial schema is as follows:
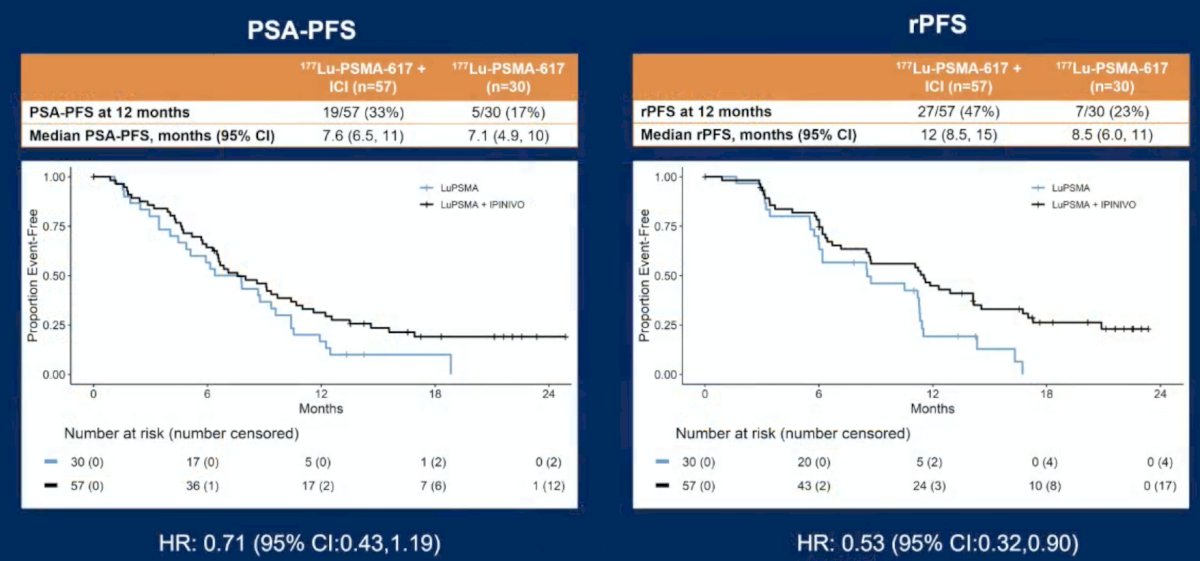
Over a median follow-up of 18 months (IQR: 16-22), PSA progression free survival at 12 months was higher in participants assigned 177Lu-PSMA-617 + immune checkpoint inhibitors than 177Lu-PSMA-617-alone (33% versus 17%; HR 0.71, 95% CI 0.43-1.19), in addition to improvement in radiographic progression free survival (47% versus 23%; HR 0.53, 95% CI 0.32-0.90):
Grade 3-4 adverse events were reported in more participants assigned 177Lu-PSMA-617 + immune checkpoint inhibitors than 177Lu-PSMA-617-alone (75% versus 29%). Among those assigned 177Lu-PSMA-617 + immune checkpoint inhibitors, Grade 3-4 adverse events in ≤5% were: colitis (19%), anemia (11%), hypophysitis (14%), lung infection (9%), fatigue (7%), thrombocytopenia (7%), hepatitis (7%), pneumonitis (7%), thromboembolic event (5%), and rash (5%). Myocarditis was reported in 4 participants (7%) assigned 177Lu-PSMA-617 + immune checkpoint inhibitors. There were 2 deaths during 177Lu-PSMA-617 + immune checkpoint inhibitor treatment: myocarditis (treatment related) and sepsis (not treatment related).
The phase I/II ongoing ALPHABET trial is testing the combination of 177Lu-PSMA-I&T + radium-223. The hypothesis is that radium-223 in combination with 177Lu-PSMA-I&T can lead to deeper and more durable responses. Patients receiveed 177Lu-PSMA-I&T 7.4 GBq IV every 6 weeks + radium-223 IV every 6 weeks for up to 6 cycles/doses, with the following clinical trial design:
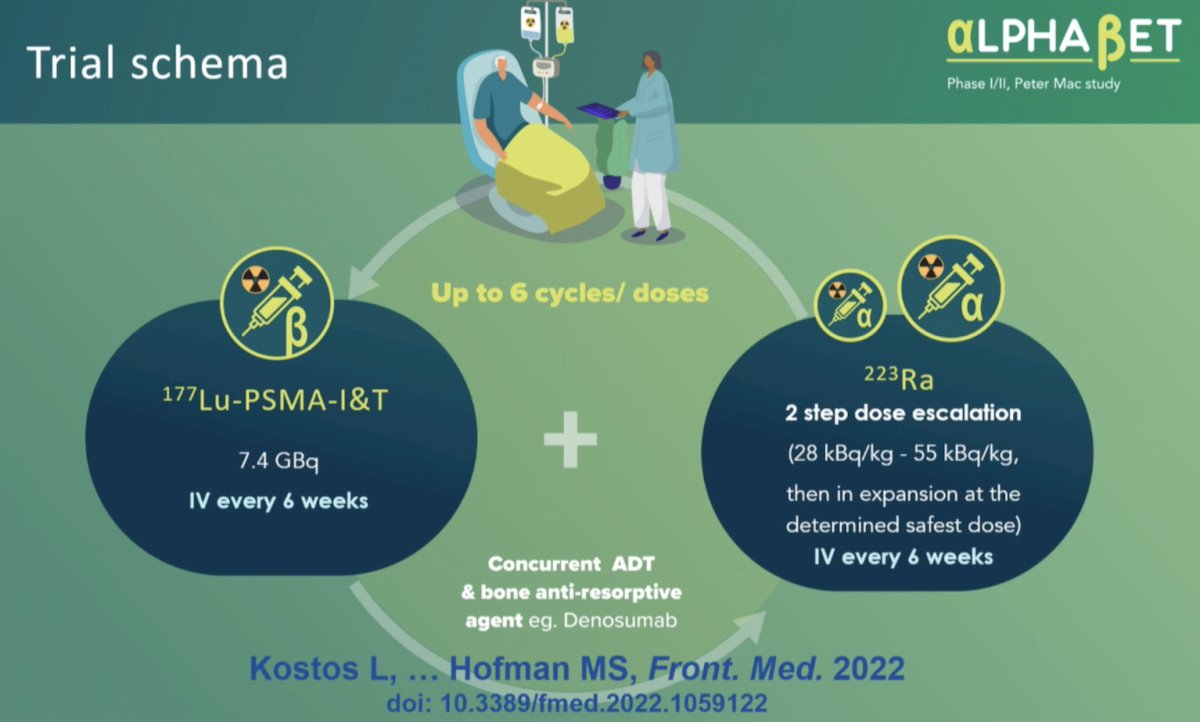
The co-primary objective is determining the maximum tolerated dose of radium-223 when combined with 177Lu-PSMA-I&T, and the PSA50 rate. Interim results were presented at ESMO 2025. Between November 3, 2022, and November 5, 2024, 36 patients were enrolled. The median age was 72.5 years (IQR 67.0-78.0), median baseline PSA was 22 ng/mL (IQR 5.8-113.0), and median ALP was 111.5 U/L (IQR 81.5-157.2). Overall, 19 patients (53%) received prior docetaxel, and no dose-limiting toxicities were observed. The maximum tolerated dose and recommended phase II dose was 55 KBq/kg radium-223 with 7.4 GBq 177Lu-PSMA-I&T. There were 11 patients (31%) that received 6 cycles of both radium-223 and 177Lu-PSMA-I&T. Grade ≥3 treatment-related adverse events occurred in 14% of patients and included anemia (n = 4) and neutropenia (n = 3) (non-clinically significant lymphopenia, n = 10); there were 4 patients (11%) that experienced grade 2 thrombocytopenia. No fractures or treatment-related deaths occurred. PSA50 and PSA90 response rates were 55% (95% CI 36–72) and 18% (7–35), respectively. Over a median follow-up of 13.3 months, the median PSA progression free survival was 5.3 months (95% CI 4.0–9.0), and median radiographic progression free survival was 10.0 (95% CI 6.7–13.5).
Moving to the mHSPC disease space, Dr. Hofman discussed the UpFrontPSMA trial,6 which included patients with de novo high-volume mHSPC who had received ≤4 weeks of ADT and had a PSA >10 ng/ml at diagnosis. Eligibility was limited to those patients with evidence of high tumor uptake and high-volume disease on PET scans. Patients were also required to have the majority of their metastatic disease demonstrating PSMA positivity. Eligible patients were randomized to:
- Experimental arm: 177Lu-PSMA-617 7.5 GBq x 2 cycles + docetaxel 75 mg/m2 x 6 cycles
- Control arm: Docetaxel 75 mg/m2 x 6 cycles
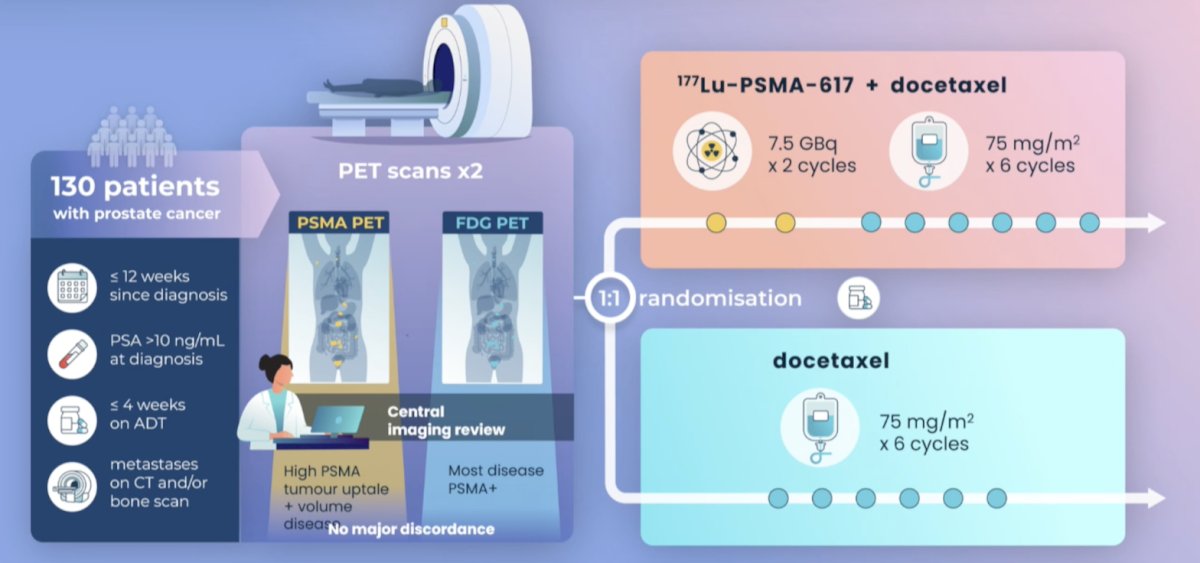
Between May 2020 and April 2023, 130 patients were recruited and underwent randomization (experimental: 63, control: 67). The median follow-up was 2.5 years. For the primary outcome, an undetectable PSA at week 48 was observed in 41% of patients in the 177Lu-PSMA + docetaxel arm versus 16% of patients in the docetaxel control arm (OR 3.88, 95% CI 1.61–9.38, p = 0.002). An undetectable PSA at any point was observed in 51% and 32% of patients, respectively (OR 2.14, p = 0.042). There were no differences in undetectable PSA levels at week 12 between the two arms (p = 0.9).
Time-to-event analyses demonstrated that patients in the experimental arm had superior PSA progression-free survival (median: 31 versus 20 months; HR 0.60, p = 0.039) and freedom from castration resistance (HR 0.60, p = 0.033). Radiographic progression-free survival similarly favored 177Lu-PSMA + docetaxel (HR 0.58, p = 0.067). Adverse events were similar in both arms, with grade 3–4 events in 27–29% of cases, and there were no new safety signals. As expected, patients in the 177Lu-PSMA arm had a higher frequency of dry mouth (37% versus 0% – all grade 1–2).
The LUNAR phase II trial7enrolled patients with recurrent oligometastatic hormone sensitive prostate cancer, characterized by 1-5 lesions outside the prostate or prostate bed on PSMA PET/CT. Patients were randomized in a 1:1 fashion to receive either stereotactic body radiotherapy to all metastatic lesions versus 2 cycles of neoadjuvant 177Lu-PSMA PNT2002 (6.8 GBq/cycles) 6-8 weeks apart followed by stereotactic body radiotherapy to all metastatic lesions. Stratification was based on number of lesions (1 versus 2-3 versus 4-5) and PSMA-based stage (N1/M1a versus M1b versus M1c):

At a median follow-up of 20 months, the addition of 177Lu-PSMA to stereotactic body radiotherapy significantly improved median progression free survival from 7.4 months (95% CI 6.0-13.5 months) to 17.6 months (95% CI 15 months – not reached; HR 0.37, 95% CI 0.22-61):

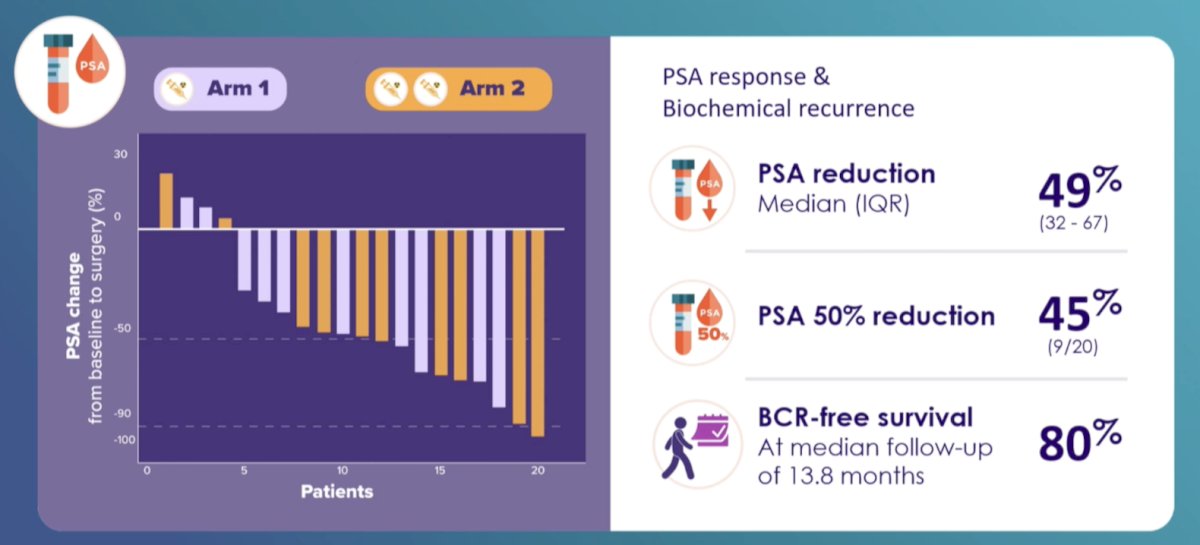
The final combination trial discussed by Dr. Hofman was the LuTectomy trial,8 with initial results published in 2023. This is a single-center, single-arm, phase 1/2 study assessing the administration of 177Lu-PSMA-617 prior to radical prostatectomy in men with high-risk localized prostate cancer:
This study included 20 patients, 10 in Cohort A (received one cycle of therapy) and 10 in Cohort B (received two cycles of therapy), followed by radical prostatectomy six weeks later. Overall, nine (45%) patients achieved >50% PSA decline, histopathological evidence of treatment effect was seen in 16 (80%) patients, one had minimal residual disease on final histology, and no patients achieved a complete pathological response. A summary of the results from LuTectomy is as follows:
Dr. Hofman concluded his presentation discussing PSMA combination strategies beyond monotherapy by emphasizing that it is time to start phase 3 trials assessing these combinations:

Presented by: Michael S. Hofman, MBBS, Peter MacCallum Cancer Center, Melbourne, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
Related content: Combination Approaches in Lutetium PSMA Therapy in mCRPC - Michael Hofman
References:
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.
- Emmett L, Subramaniam S, Crumbaker M, et a. [177Lu]Lu-PSMA-617 plus enzalutamide in patients with metastatic castration-resistant prostate cancer (ENZA-p): An open-label, multicentre, randomized, phase 2 trial. Lancet Oncol. 2024 May;25(5):563-571.
- Emmett L, Subramaniam S, Crumbaker M, et al. Overall survival and quality of life with [177Lu]Lu-PSMA-617 plus enzalutamide versus enzalutamide alone in metastatic castration-resistant prostate cancer (ENZA-p): Secondary outcomes from a multicentre, open-label, randomized, phase 2 trial. Lancet Oncol. 2025 Mar;26(3):291-299.
- Emmett L, Swiha M, Papa N, et al. Predictive value of early PSMA upregulation for the response to enzalutamide +/- 177Lu-PSMA-617 in poor-risk, metastatic, castration-resistant prostate cancer: Substudy of the randomized, phase 2 ENZA-p trial. Nat Cancer. 2026 Apr;7(4):622-630.
- Sandhu S, Joshua AM, Emmett L, et al. [177Lu]Lu-PSMA-617 in combination with pembrolizumab for treatment of metastatic castration resistant prostate cancer (PRINCE): A single-arm, phase 1b/2 study. Lancet Oncol. 2026 Apr;27(4):470-479.
- Azad AA, Bressel M, Tan H, et al. Sequential [(177)Lu]Lu-PSMA-617 and docetaxel versus docetaxel in patients with metastatic hormone sensitive prostate cancer (UpFrontPSMA): A multicentre, open label, randomized, phase 2 study. Lancet Oncol. 2024 Oct;25(10):1267-1276.
- Kishan AU, Valle LF, Wilhalme H, et al. 177Lu-Prostate-Specific Membrane Antigen Neoadjuvant to Stereotactic Ablative Radiotherapy for Oligorecurrent Prostate Cancer (LUNAR): An open-label, randomized, controlled, phase II study. J Clin Oncol. 2025 Dec 20;43(36):3812-3821.
- Eapen RS, Buteau JP, Jackson P, et al. Administering [177Lu]Lu-PSMA-617 Prior to Radical Prostatectomy in Men with High-risk Localized Prostate Cancer (LuTectomy): A Single-centre, single-arm, phase 1/2 study. Eur Urol. 2023 Oct 25:S0302-2838(23)03087-7.