(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a monitoring session and a presentation by Dr. Channing Paller discussing monitoring in metastatic hormone sensitive prostate cancer (mHSPC). Monitoring in mHSPC includes blood markers (PSA, LDH, alkaline phosphatase), imaging (whole body MRI, CT/bone scan, and PSMA PET), and discordant progression when radiographic and/or clinical progression occur without PSA progression.
With regards to PSA, a baseline PSA and every 3-6 months after initiation of ADT should be standard, with the caveat that there can be a transient PSA rise (flare) after starting therapy. PSA progression is defined as >= 25% and >= 2 ng/mL above nadir/baseline and confirmed by a second value >= 3 weeks later (PCWG3). According to PCWG4, this is defined as 0.2 mg/mL above nadir/baseline. Of note, PSA progression often precedes clinical or radiographic progression, and we should measure testosterone when PSA is increasing to screen for CRPC.
What about PSA as a predictive biomarker in mHSPC? We know that a PSA <0.2 ng/mL at 6-12 months of treatment is associated with a good prognosis. A PSA > 0.2 ng/mL after 6-12 months of treatment is associated with a poor prognosis and has led to a new set of treatment intensification trials:
- TRIPLE-SWITCH (SWOG/CCTG-PR26): ADT + androgen receptor pathway inhibitors +/- docetaxel
- PEACE 6: standard of care +/- LuPSMA
- INTENSIFY: ADT + androgen receptor pathway inhibitor +/- docetaxel
Similarly, for patients with a PSA <= 0.2 ng/mL after 6-12 months of treatment is associated with the best prognosis and the opportunity to enroll patients in de-intensification trials:
- LIBERTAS: apalutamide + intermittent versus continuous ADT
- DE-ESCALATE (EORTC 2238): intermittent ADT + androgen receptor pathway inhibitor
- A-DREAM: interruption ADT and androgen receptor pathway inhibitors
A high alkaline phosphatase level is associated with poor overall and progression free survival in prostate cancer. A transient alkaline phosphatase elevation may occur after starting systemic therapy in patients with prostate cancer and bone metastases. Similarly, an elevated lactate dehydrogenase is associated with poor overall and progression free survival in patients with metastatic disease. Taken together, both of these blood tests are prognostic biomarkers for prostate cancer and may help interpret discordant findings.
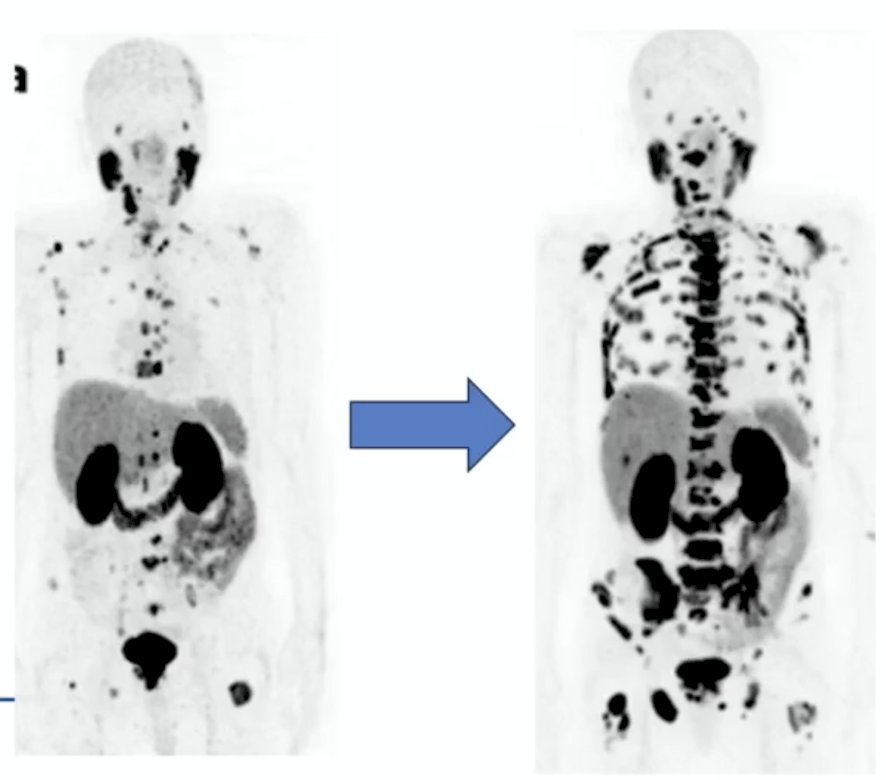
Whole body MRI is superior for detecting metastatic disease compared with conventional imaging. In one study, whole body MRI identified metastases in 11% of patients with a negative bone scan, and 35.7% of patients with an equivocal bone scan:

However, there is a financial and time cost associated with whole body MRI, in addition to whole body MRI not performing as well as PSMA PET/CT.
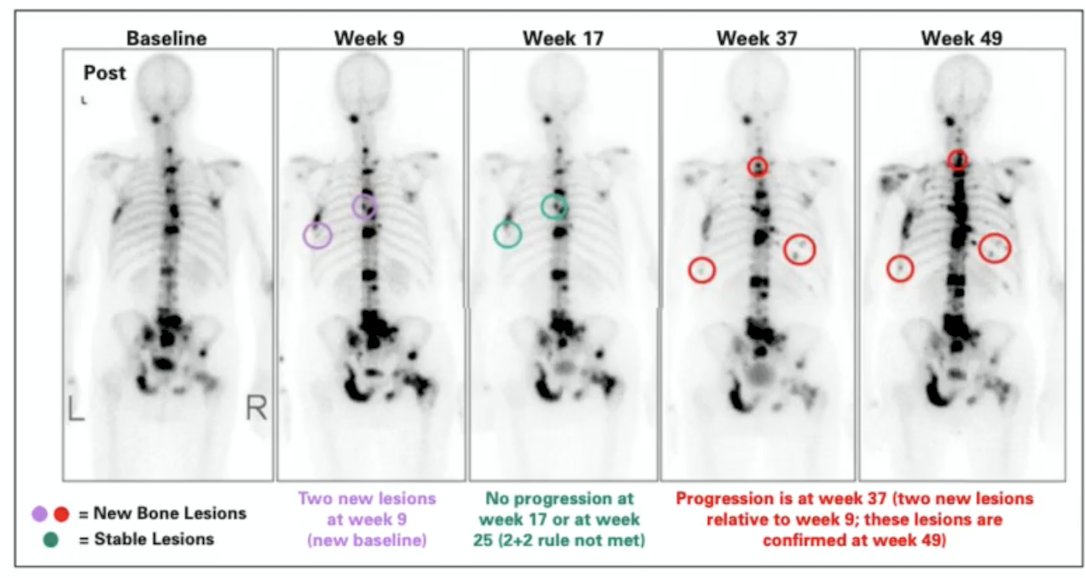
Conventional imaging is defined as a CT scan (modified RECIST) and a bone scan (PCWG3), which can result in a flare phenomenon occurring in up to 50% of patients. This requires repeated bone scans with the use of the 2+2 rule:
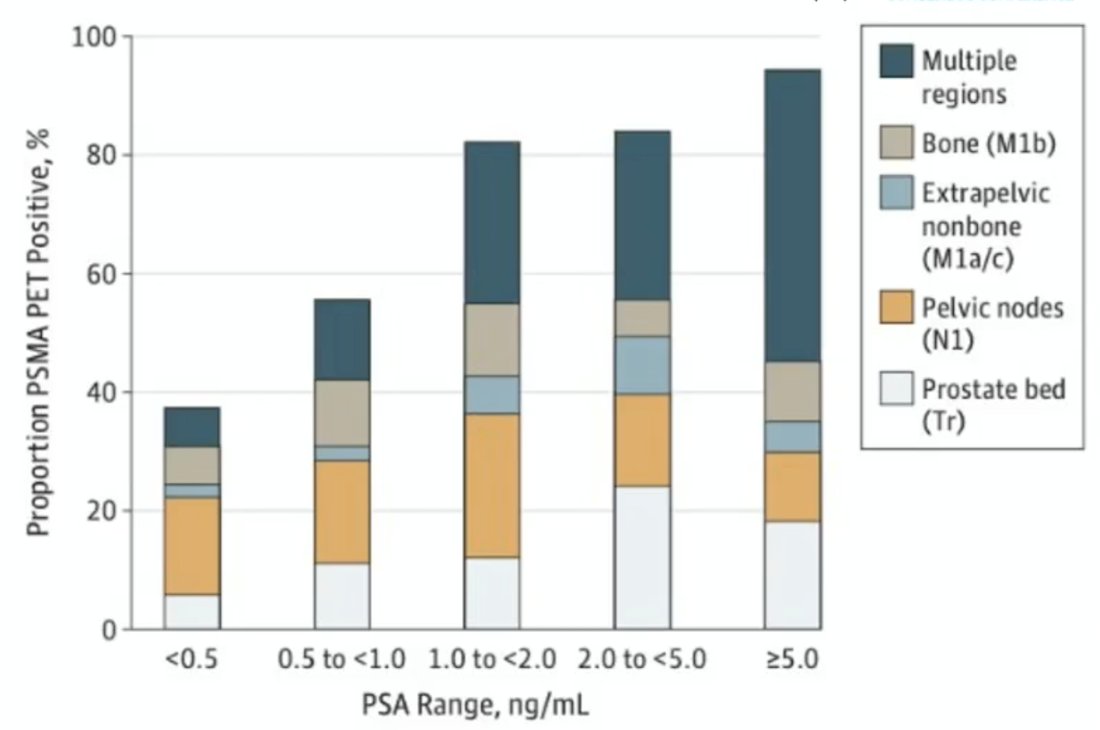
PSMA PET has redefined staging accuracy and therapeutic stratification of mHSPC. Compared to conventional imaging, PSMA PET has superior sensitivity and specificity for detecting nodal and osseous metastatic lesions. In high risk non metastatic HSPC, by conventional imaging, PSMA PET was positive in 84% of patients, suggesting understaging by conventional imaging:1
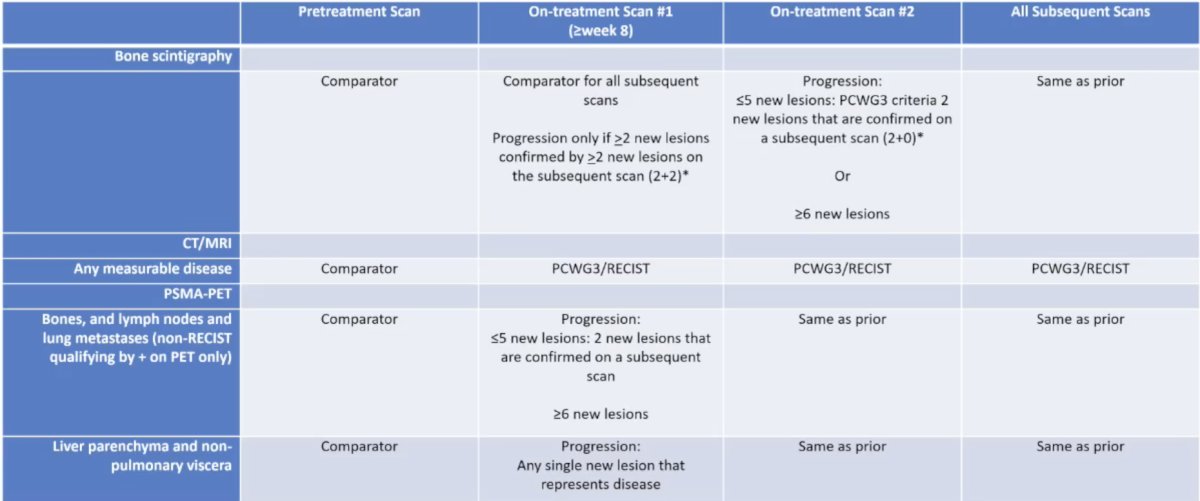
Initially presented at ASCO GU 2026, PCWG4 incorporates for the first time PSMA PET. For a new lesion, Dr. Paller advocates a high reader confidence based on a combination of factors, including intensity of PSMA uptake, anatomic correlates on cross sectional imaging, and pattern of spread. If the PSMA PET is performed earlier than 8 weeks, the information is non-actionable, whereas if a scan has new disease at 8 weeks or beyond, this information can be taken at face value. Changes in disease volume or SUV parameters are investigational and are not progression criteria at this time, and collection of data in these situations is key. Thus, there are no partial responses or progressive disease by SUVs or volume of disease. RECIST still applies to the CT component, we must get contrast with the PSMA PET/CT. Dr. Paller also noted the PCWG4 “rule of 5” (bone, nodes, lung): <=5 new lesions must have 2 lesions that are confirmed on a subsequent scan, and >= 6 new lesions are deemed progression of disease. PSMA PET findings should be reported separately from bone scan findings and reported separately from CT findings. Of note, there are no implications for treatment until these findings are validated, with the exception that any single liver, adrenal, or non-pulmonary visceral lesion constitutes progression:
PCWG4 imaging delays and prevents endpoints:
Dr. Paller then reviewed her 10 years of lessons learned regarding PSMA PET false positives:
- This has led to stage and risk migration
- We must consider lead time and length time bias
- Potential false positive findings include: Paget’s disease of the bone, peripheral ganglia, proximal small bowel, liver, spleen, kidneys, salivary glands, lacrimal glands, vocal cords, reactive lymph nodes, non-small cell lung cancer, adrenal/renal cell cancer, gastric/colon cancer, adenocarcinoma, and neuroendocrine tumors
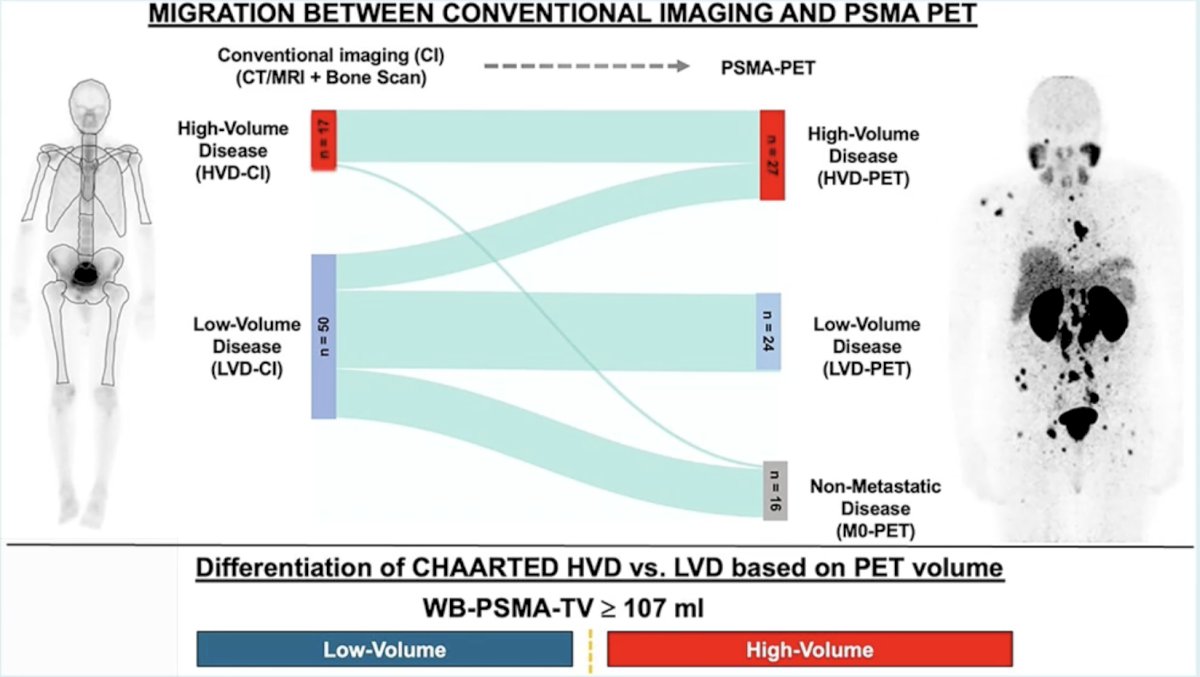
In 2025, Unterrainer et al.2 published a retrospective multicenter study to compare the conventional imaging-based disease volume criteria to PSMA PET-based volume definitions in a CHAARTED-like cohort of 67 patients with paired PSMA PET and bone scans. On the basis of conventional imaging, 17 of 67 patients had high volume disease on conventional imaging (25.4%), and 50 of 67 patients had low volume disease on conventional imaging (74.6%). On the basis of PSMA PET, 27 of 67 patients had high volume disease on PET imaging (40.3%), and 24 of 67 patients had low volume disease on PET imaging (35.8%). In total, 16 of 67 patients (22.4%) had no visible lesion or only locoregional pelvic disease (M0) with PSMA PET. Stage migration between conventional imaging and PSMA PET occurred in 27 of 67 patients (40.3%) by both upstaging and downstaging: 11 of 50 (22%) low volume disease on conventional imaging patients were high volume disease on PET imaging, whereas 1 of 17 (5.9%) high volume disease on conventional imaging and 15 of 50 (30%) of low volume disease on conventional imaging patients were PSMA PET negative:
In the TITAN trial, nearly half of patients with mHSPC treated with apalutamide experienced radiographic progression without PSA progression, suggesting that reliance on PSA monitoring may be inadequate for assessing disease activity:3

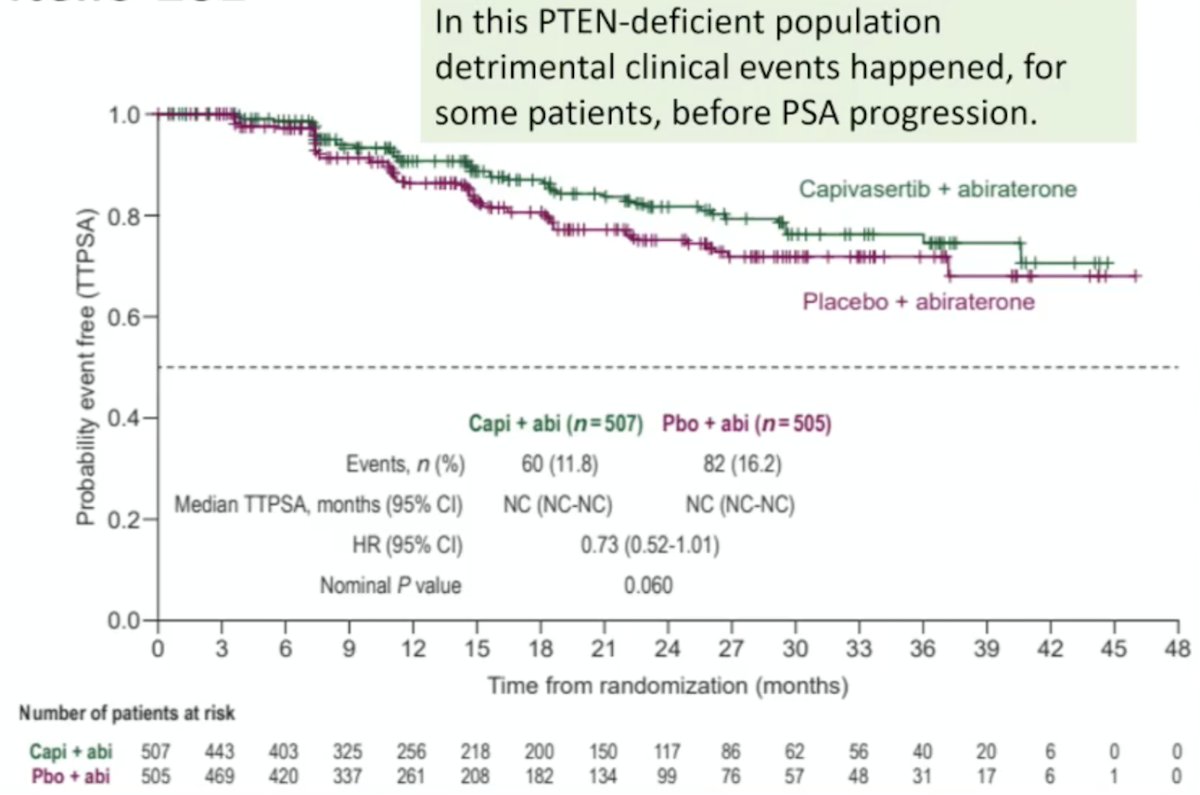
In CAPItello-281,4 capivasertib + abiraterone improves radiographic progression free survival versus placebo + abiraterone, with a 7.5 month improvement in median radiographic progression free survival (overall survival is immature). Early PSA progression was less common in both arms, particularly when compared to clinical progression events. In this PTEN-deficient population detrimental clinical events happened, for some patients, before PSA progression:
Dr. Paller concluded her presentation discussing monitoring mHSPC with the following take-home points:
- PSA remains the primary, non-invasive biomarker for serial monitoring in mHSPC:
- Prognostic
- PSA alone is insufficient
- Alkaline phosphatase and lactate dehydrogenase: prognostic
- PCWG4: PSMA PET progression criteria
- There is no set interval for imaging, and imaging can show progression in the absence of PSA progression:
- These findings highlight the need for integrated monitoring methods, combining PSA/LDH/ALKP changes, pathology, and other evolving biomarkers, with clinical assessment and appropriate imaging
Presented by: Channing Paller, MD, The Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins University School of Medicine, Baltimore, MD
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:
- Fendler WP, Calais J, Eiber M, et al. Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer: A Prospective Single-Arm Clinical Trial. JAMA Oncol 2019 Jun 1;5(6):856-863.
- Unterrainer LM, Hope TA, Fendler WP, et al. Low- and high-volume disease in metastatic hormone-sensitive prostate cancer: From CHAARTED to PSMA PET-An International Multicenter Retrospective study. J Nucl Med. 2025 Jan 3;66(1):54-60.
- Fukuokaya W, Yanagisawa T, Mori K, et al. Radiographic progression without corresponding prostate-specific antigen progression in patients with metastatic castration-sensitive prostate cancer receiving apalutamide: Secondary analysis of the TITAN trial. Eur Urol Oncol. 2025;8(2):263-269.
- Fizazi K, Clarke NW, De Santis M, et al. Capivasertib plus abiraterone in PTEN-deficient metastatic hormone-sensitive prostate cancer: CAPItello-281 phase III study. Ann Oncol. 2026 Jan;37(1):53-68.