(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management and prevention of frequent side effects and modifying the metabolism session, and a presentation by Dr. Lisa Horvath discussing the evidence for using statins or low-dose aspirin in advanced prostate cancer.
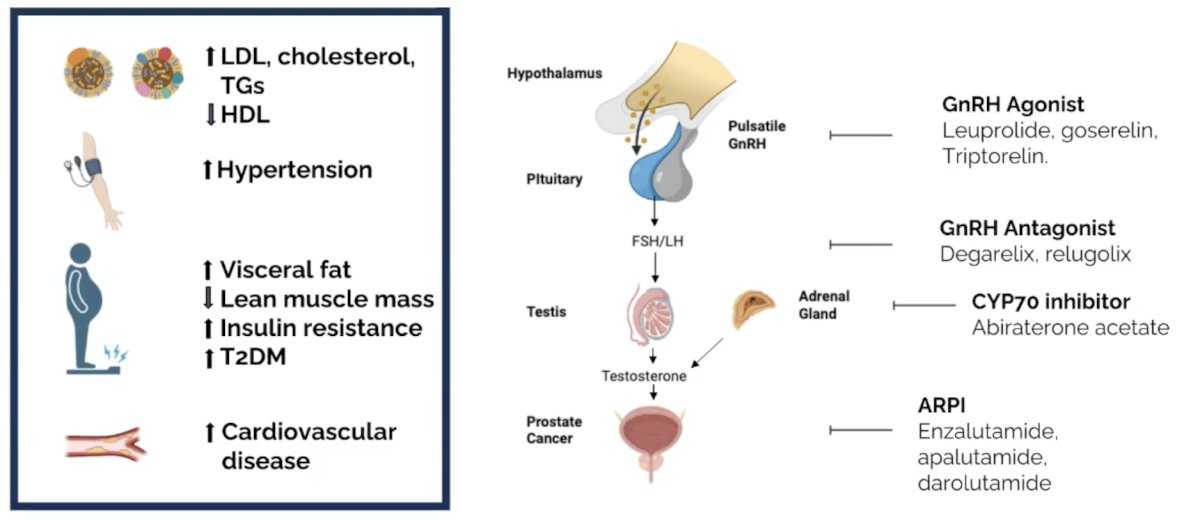
Dr. Horvath presented a case of a 70-year-old man with de novo low-volume mHSPC treated with leuprolide + enzalutamide, with a PSA < 0.01 ng/mL. The patient is wondering if he should take statins and aspirin, and whether this will improve prostate cancer survival and prevent a heart attack. The following figure highlights the metabolic effects of ADT +/- androgen receptor pathway inhibitor:
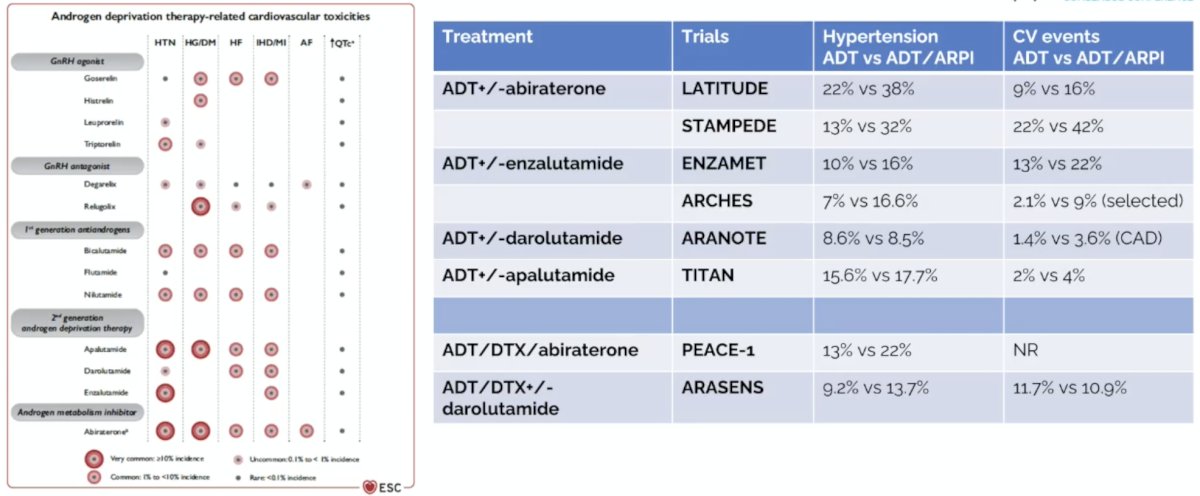
Cardiovascular toxicity is a concern for advanced prostate cancer systemic therapy, including for patients receiving ADT and ADT + androgen receptor pathway inhibitors in mHSPC:
The mechanism of statins for cardiovascular effects is to reduce arterial plaque and function as an anti-inflammatory. The statins and anticancer effect mechanism is also based on an anti-inflammatory effect, as well as a decrease in poor prognostic plasma sphingolipids, and decreased angiogenesis/cell proliferation/invasion, and increased apoptosis. The mechanism of aspirin for cardiovascular effects is to reduce anti-thrombotic and anti-inflammatory effects. The aspirin and anticancer effect mechanism is also based on an anti-inflammatory effect, changes in cellular metabolism, and antiplatelet treatment affects in tumor cell growth.
The following table highlights statins and aspirin for preventing cardiovascular events:

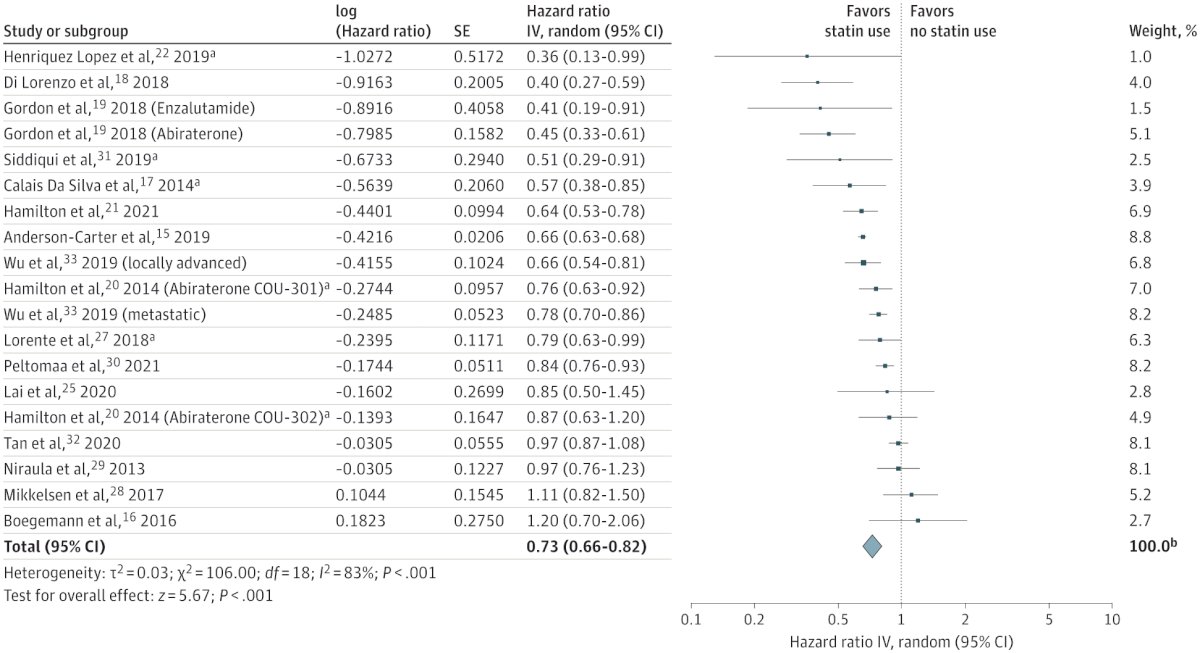
Jayalath et al.1 performed a systematic review and meta-analysis assessing statin use and survival among men receiving therapy for advanced prostate cancer. There were 25 studies comprising 119,878 men (65,488 statin users). Concurrent statin use was associated with a 27% reduction in the risk of overall mortality (HR 0.73, 95% CI 0.66-0.82):
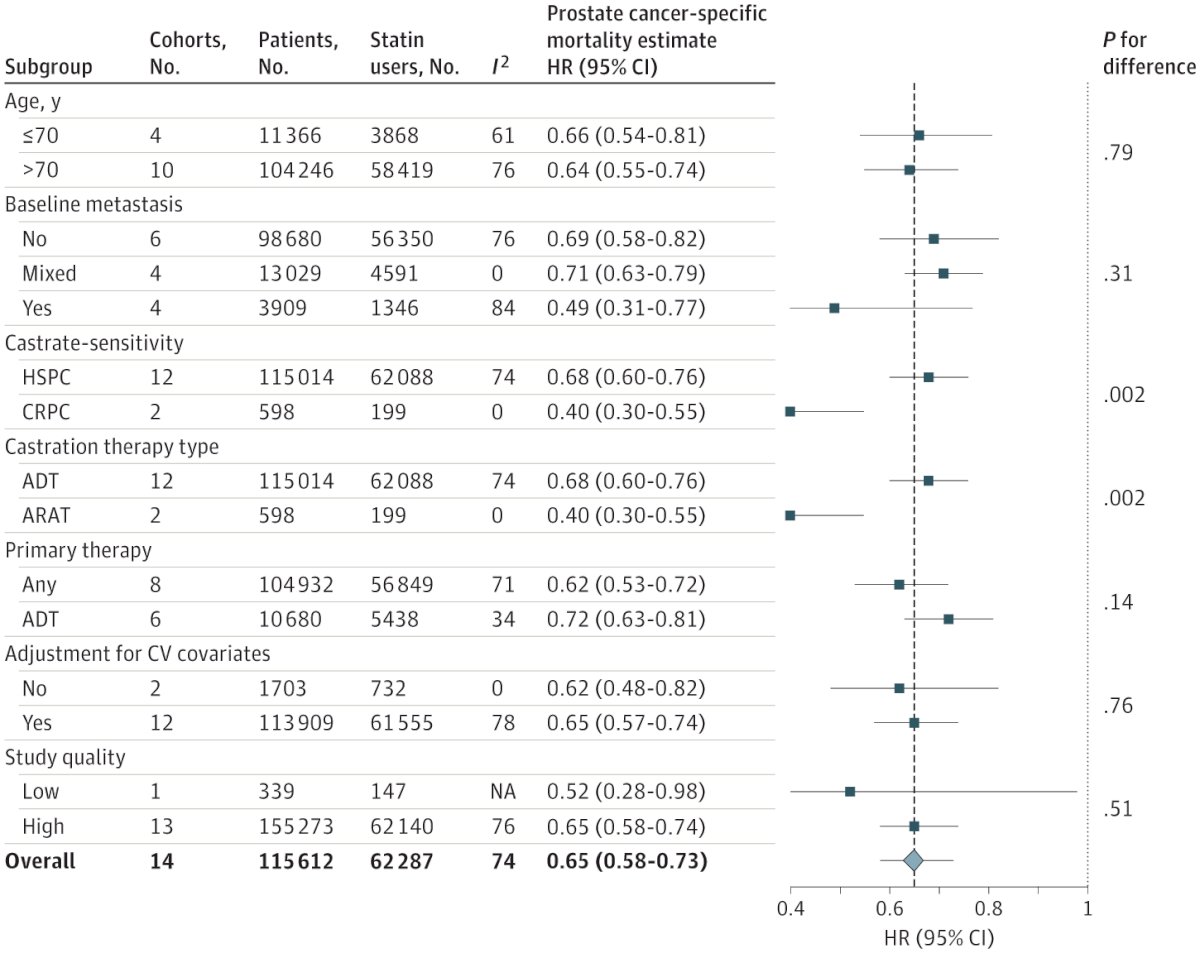
Concurrent statin use was also associated with a 35% reduction in the risk of prostate cancer-specific mortality (HR 0.65, 95% CI 0.58-0.73):
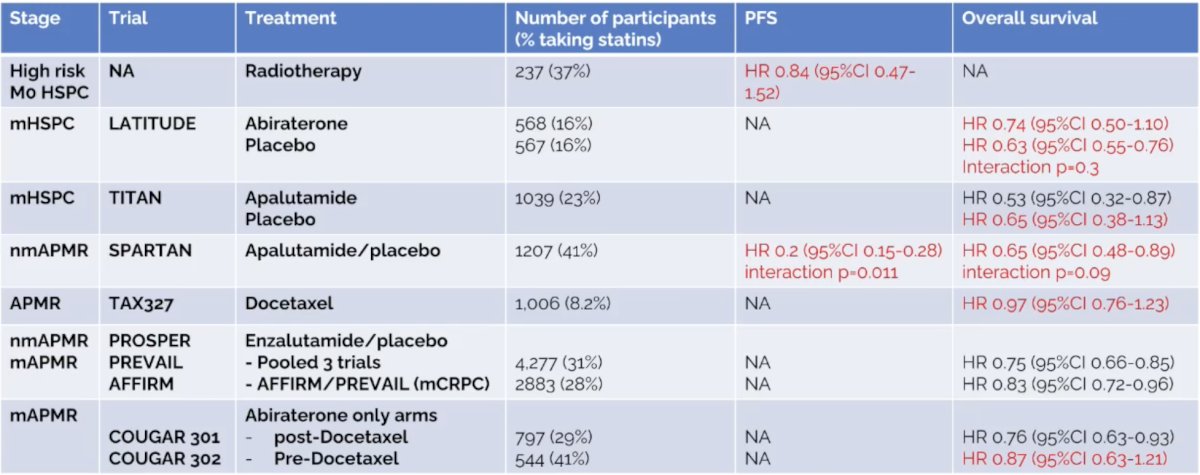
Dr. Horvath provided the following table highlighting statin use in advanced prostate cancer:
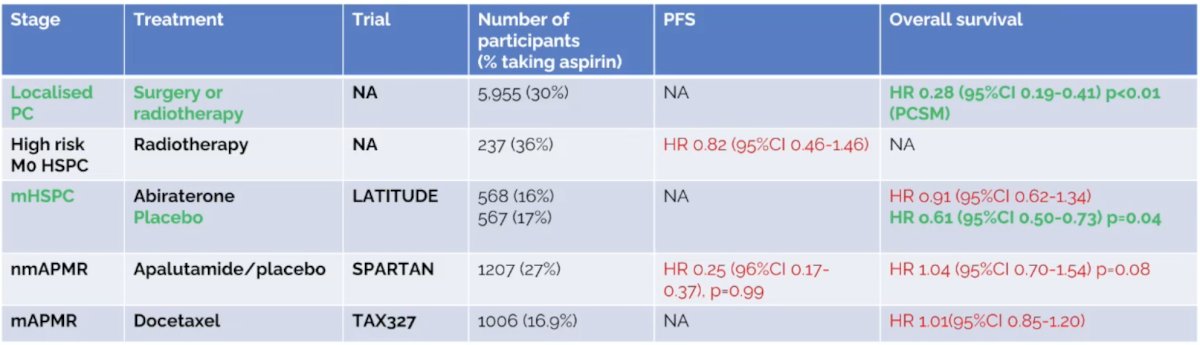
With regards to aspirin use in advanced prostate cancer, a meta-analysis of >10 million patients (60 studies) found a decreased prostate cancer incidence (RR 0.96, 95% CI 0.95-0.98) and decreased prostate cancer mortality (RR 0.88, 95% CI 0.82-0.95). In a subgroup analysis, there was a decreased incidence and mortality reached significance only in the Americas, but not in Europe or Oceania. The following table shows the current literature for aspirin use in advanced prostate cancer:
Statins and aspirin are associated with the following side effects:
- Statins
- Muscle pain: 7% excess in year 1
- Type 2 diabetes mellitus: 0.5-2%/year (dose dependent)
- Transaminitis: <1%/year
- Edema: <2%/year
- Aspirin
- Gastrointestinal disturbance: 15-20%
- Gastric ulcers: 5 extra cases /1000 aspirin users/year
- Gastrointestinal bleeding: 1-2 extra cases /1000 aspirin users/year
- Intracranial bleeding: 1-2 extra cases /10,000 aspirin users/year
Statins are associated with several drug-drug interactions, including (i) enzalutamide/apalutamide decreasing statin levels, (ii) abiraterone raising statin levels (especially simvastatin), and (iii) darolutamide raising statin levels (especially rosuvastatin). Notably, aspirin does not have any significant drug-drug interactions.
Future research includes the PEACE-4 trial randomizing patients to standard of care versus standard of care + aspirin 100 mg versus standard of care + atorvastatin 80 mg versus standard of care + aspirin 100 mg + atorvastatin 80 mg.
Dr. Horvath concluded her presentation discussing the evidence for using statins or low-dose aspirin in advanced prostate cancer by emphasizing what we should be telling patients:
- Discuss statins for improved cardiovascular health, depending on cholesterol level and potential anti-cancer effect
- Do not take aspirin unless there is a cardiovascular reason for doing so (ie, secondary prevention after a cardiovascular event)
Presented by: Lisa Horvath, MBBS, PhD, Chris O’Brien Lifehouse, Professor of Medical Oncology (Genitourinary Cancers), University of Sydney, Sydney, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.