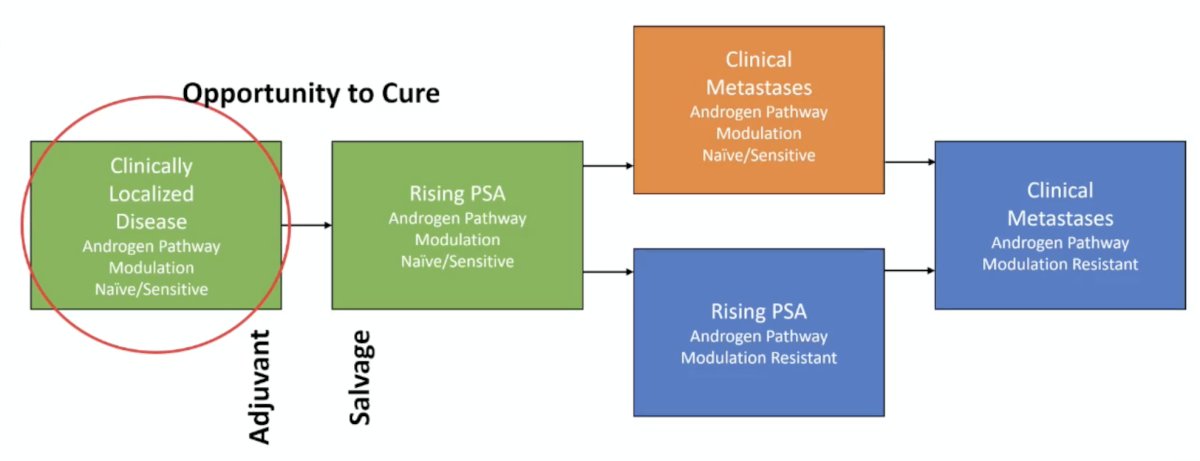
(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a high risk and locally advanced prostate cancer session and a presentation by Dr. Rana McKay discussing how to treat older patients with high-risk and locally advanced prostate cancer. Among the clinical states of prostate cancer, Dr. McKay notes that there is an opportunity for cure when patients have clinically localized disease and for those treated with adjuvant or salvage treatment for a rising PSA after localized treatment:
There are several epidemiological points to keep in mind when considering treating older patients with high risk prostate cancer:
- The median age at diagnosis is 66 years
- 60% of patients are diagnosed >65 years of age
- 20% of patients are diagnosed >75 years of age
- Men 70+ years of age carry the highest incidence of prostate cancer, with rates rising since 2014
- Distant stage disease increases at 6.2%/year among men 70+ years of age
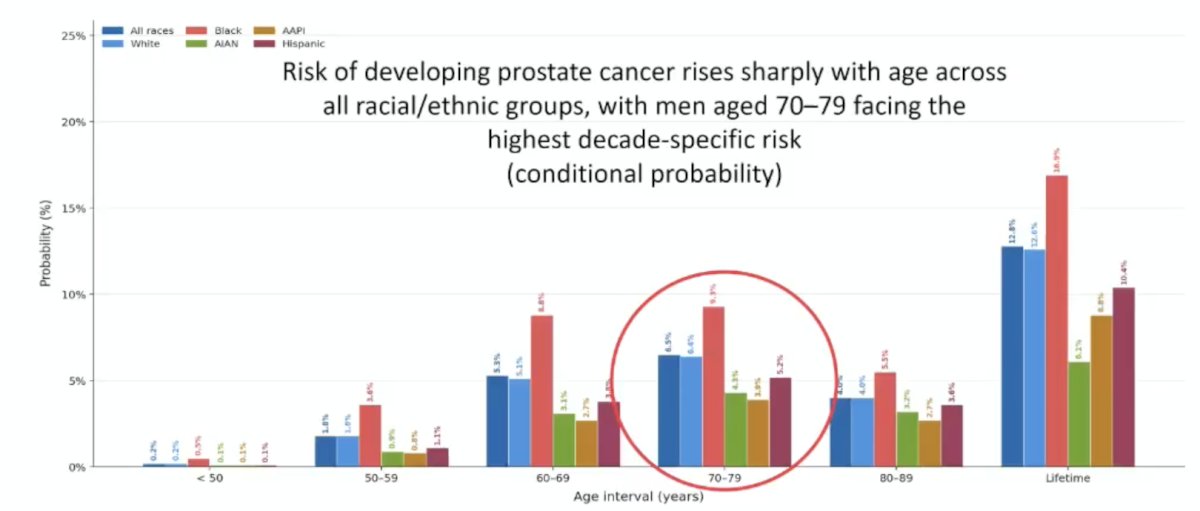
Dr. McKay notes that the risk of developing prostate cancer rises sharply with age across all racial/ethnic groups, with men aged 70-79 facing the highest decade-specific risk (conditional probability):
Moreover, the burden of death also shifts dramatically to older men, with 80% of the projected 35,770 deaths in 2025 occurring in men aged 70 and older:

Assessing age alone is not enough, given that chronological age is not equivalent to biological age. Further, frailty is not equivalent to comorbidity, which is not equivalent to disability. Dr. McKay emphasized that ECOG and Karnofsky performance status are inadequate in older adults, and we need better measures to assess fitness for treatment. As follows are several important definitions:
- Comorbidity: coexisting chronic disease
- Disability: dependence on activity of daily living
- Frailty: reduced physiologic reserve and vulnerability to stressors leading to poor outcomes
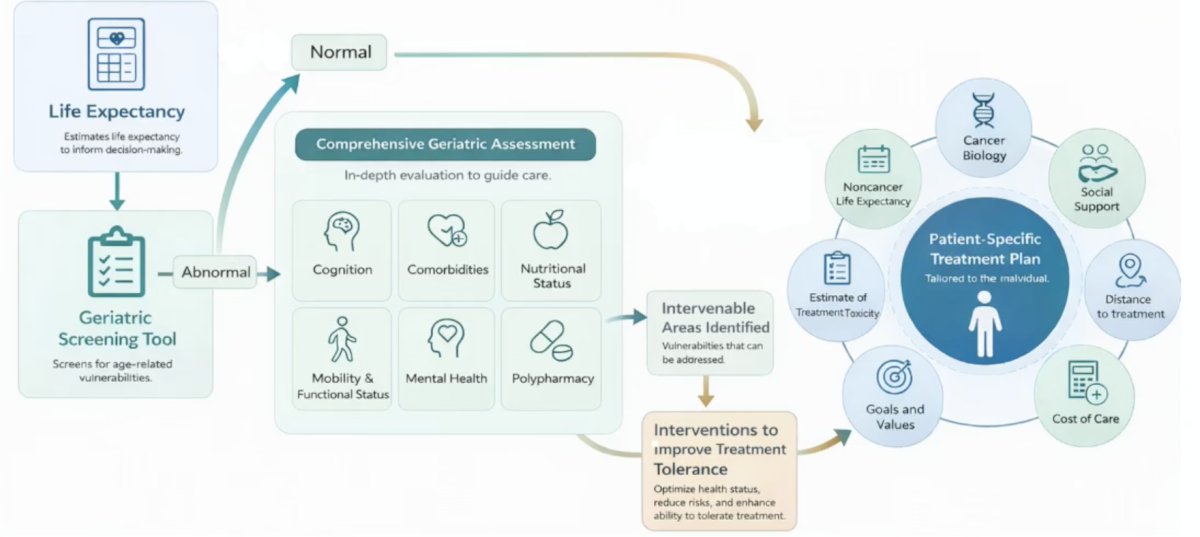
The following framework for risk assessment is provided from the 2023 ASCO Educational Book:
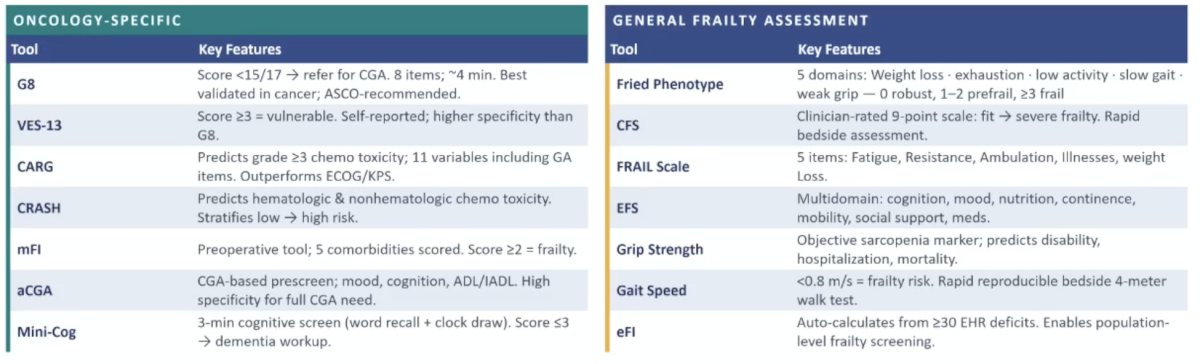
The 2026 ASCO Educational Book also provides oncology specific and general frailty assessments, recommending the Geriatric 8 as the first line screen in older adults with cancer:
The purpose of the Geriatric 8 screening tool is a brief oncology screening tool to identify older patients who need a full cognitive geriatric assessment. The tool is structured with 8 items: nutrition, weight loss, BMI, mobility, neuropsychological status, polypharmacy (>3 medications), self-rated health, and age. Scoring ranges from 0-17, with <= 14 as abnormal and triggering a cognitive geriatric assessment referral:
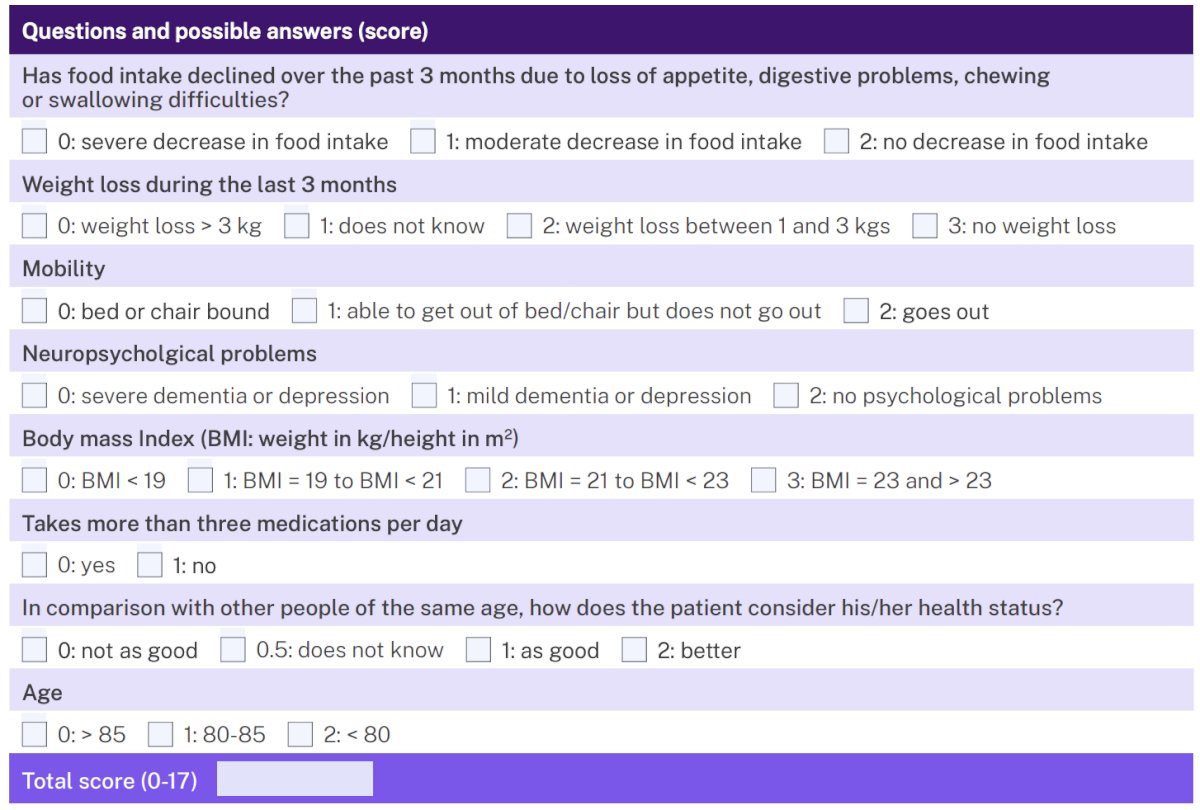
The Geriatric 8 screening tool has a high sensitivity (~77-92%), moderate specificity, and predicts survival, chemotherapy toxicity, and functional decline. Finally, the tool is endorsed by ASCO, SIOG, and NCCN, and is an acceptable first line screening tool alongside VES-13.
Dr. McKay highlighted the complexity of treatment decision making for locally advanced disease, including:
- Choice of local therapy (ie. surgery, radiation, no treatment)
- Choice of ADT (+/- ADT and agent choice)
- Choice of ADT intensity (+/- androgen receptor pathway inhibitor and agent choice)
- Choice of ADT duration
Specific to local therapy, there are several considerations:
- Radical prostatectomy
- Feasible for fit men with a life expectancy of 10+ years
- Higher incontinence and erectile dysfunction
- Requires cardiopulmonary and cognitive reserve
- Anesthetic risk
- Radiation therapy
- Well tolerated across age groups
- Hypofractionation/stereotactic body radiotherapy reduce treatment burden
- Genitourinary/gastrointestinal toxicity is not age dependent
- ADT toxicity is the age-specific concern
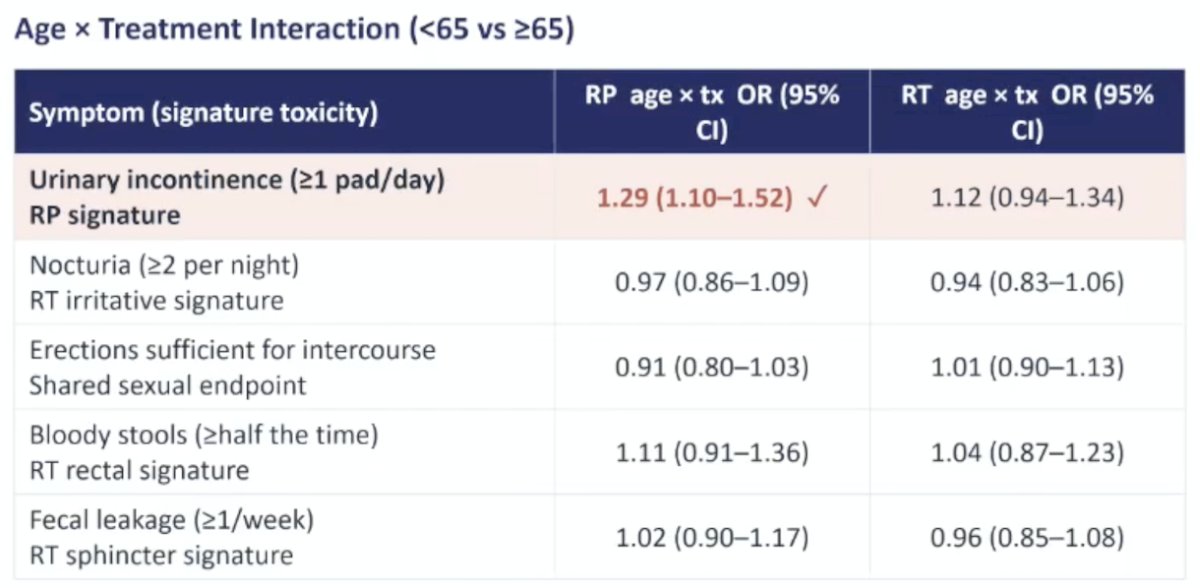
The 12 year patient reported outcomes form the ProtecT trial1 noted that post-radical prostatectomy incontinence was the only age-dependent treatment toxicity: pad use was 22-27% in men >= 65 years of age versus 15-22% in men <65 years, 7-12%:
Regarding systemic therapy, patients with STAMPEDE high risk disease (2/3 of T3-T4, Gleason score 8-10, or PSA 40+ ng/mL) had a treatment benefit with abiraterone regardless of age: <70 years HR 0.52, 95% CI 0.41-0.66; >=70 years HR 0.55, 95% CI 0.41-0.73.2 However, in ENZARAD, which assessed the addition of enzalutamide to ADT + radiotherapy for high risk patients, there was no benefit in the intention to treat population, as well as for patients <70 years of age (HR 0.69, 95% CI 0.45-1.05) and >=70 years of age (HR 1.07, 95% CI 0.74-1.53).
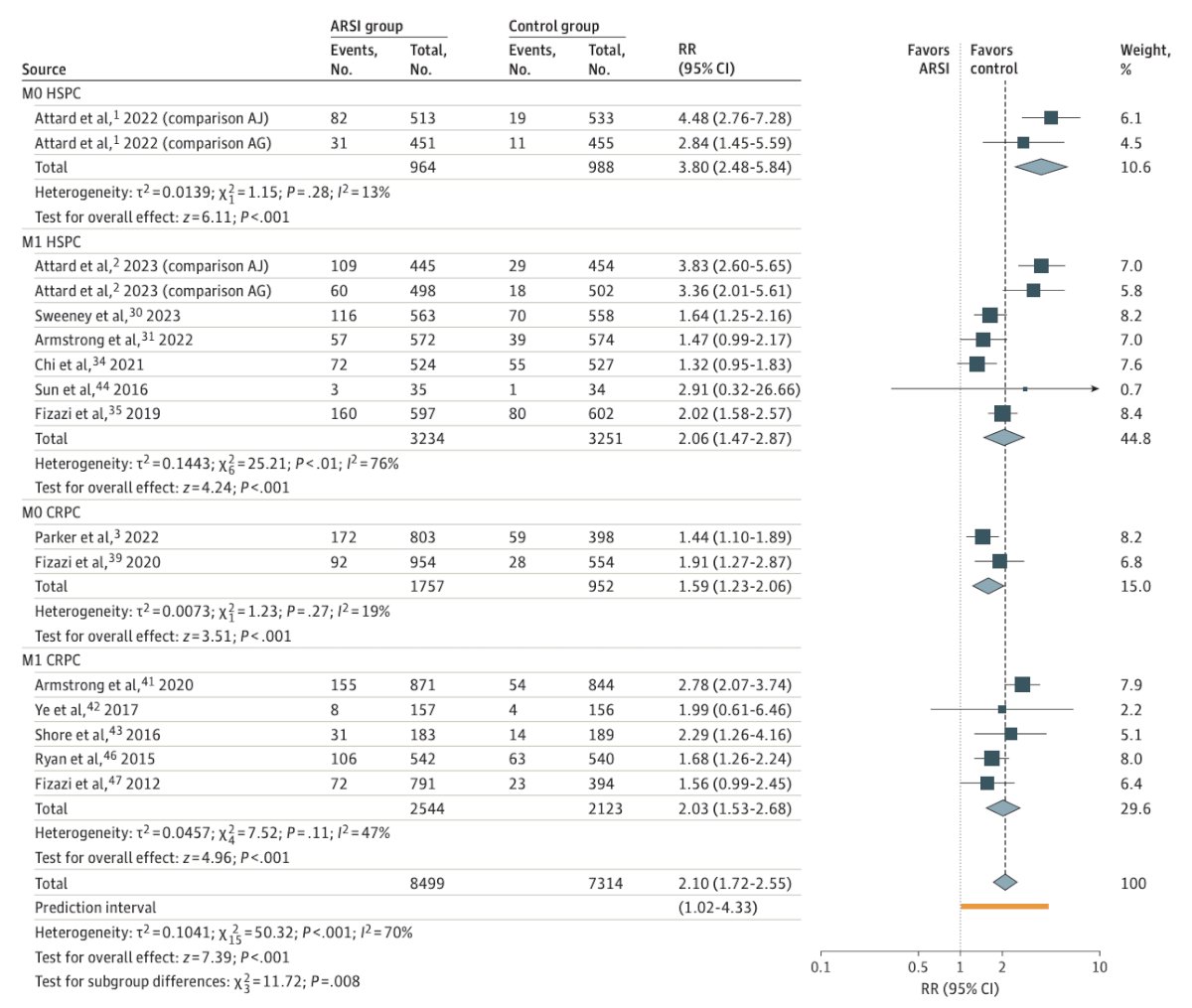
In 2024, El-Taji et al.3 performed a systematic review and meta-analysis of 24 studies assessing cardiovascular events and androgen receptor signaling inhibitors in advanced prostate cancer. The median age was 63–77 years, with ~67% of androgen receptor pathway inhibitor treated men have ≥1 cardiovascular risk factor. Overall, androgen receptor pathway inhibitor + ADT doubled grade ≥3 cardiovascular events (15.6% versus 7.8%; RR 2.10), and M0 hormone sensitive prostate cancer had the highest relative risk across states (Grade ≥3 cardiovascular events: 6.9% versus 2.4–3.6%; RR 3.80). Of note, age did not moderate cardiovascular risk, whereas comorbidity burden did:
Ultimately, shared decision among elderly, high risk prostate cancer patients is crucial.
Dr. McKay concluded her presentation discussing how to treat older patients with high-risk and locally advanced prostate cancer with the following take-home points:
- There is a rising prostate cancer burden among older men, who carry higher rates of comorbidity, polypharmacy, and frailty
- Frailty should be assessed as it shapes treatment tolerance, outcomes, and survival
- Local therapy, choice of ADT, androgen receptor pathway inhibitor use, and ADT duration should be individualized to life expectancy, disease risk, frailty, and patient preference
Presented by: Rana McKay, MD, University of California – San Diego, San Diego, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:
- Donovan JL, Hamdy FC, Lane JA, et al. Patient-reported outcomes 12 years after localized prostate cancer treatment. NEJM Evid. 2023 Apr;2(4):EVIDoa2300018.
- Attard G, Murphy L, Clarke NW, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: A meta-analysis of primary results from two randomized controlled phase 3 trials of the STAMPEDE platform protocol. Lancet 2022 Jan 29;399(10323):447-460.
- El-Taji O, Taktak S, Jones C, et al. Cardiovascular events and androgen receptor signaling inhibitors in advanced prostate cancer: A systematic review and meta-analysis. JAMA Oncol. 2024 Jul 1;10(7):874-884.