(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a high-risk and locally advanced prostate cancer session and a presentation by Dr. Jeff Michalski discussing that patients with high-risk localized prostate cancer do not need the addition of an androgen receptor pathway inhibitor to radiotherapy + ADT. Dr. Michalski started his portion of the debate by noting that based on 2022 STAMPEDE data, there is a benefit from an androgen receptor pathway inhibitor for these men, with a notable improvement in metastasis free survival and overall survival with abiraterone, as well as a 6-year prostate cancer specific survival benefit (93% with abiraterone versus 85% without abiraterone; HR 0.49, 95% CI 0.37-0.65).1
However, based on 2025 ENZARAD data, patients do not benefit from an androgen receptor pathway inhibitor, based on no difference in metastasis-free survival or overall survival with enzalutamide, as well as no difference in 8-year prostate cancer-specific survival (97% with enzalutamide versus 96% with a non-steroidal antiandrogen; HR 0.90, 95% CI 0.41-1.97). Dr. Michalski emphasized that both the STAMPEDE and ENZARAD trials used conventional imaging for staging. Notably, STAMPEDE had higher-risk patients enrolled compared to ENZARAD, including more cN1 patients (39% versus 11%), more clinical T3/T4 patients (92% versus 47%), and a higher median PSA (35 ng/mL versus 14 ng/mL):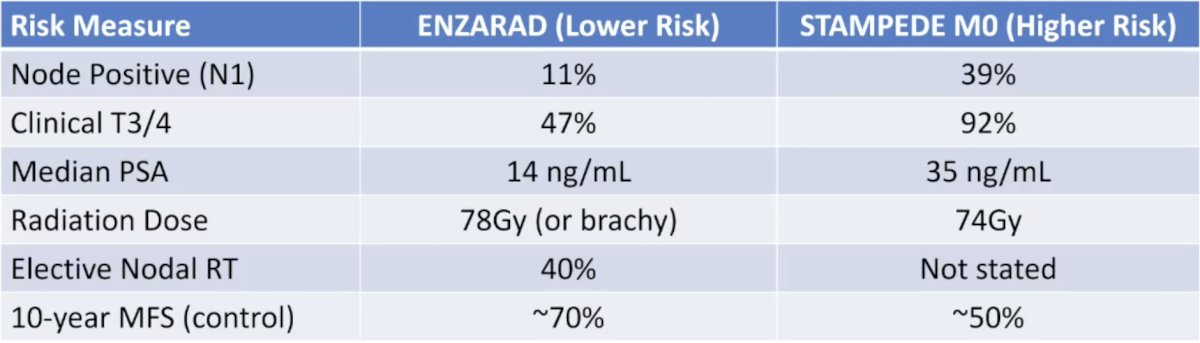
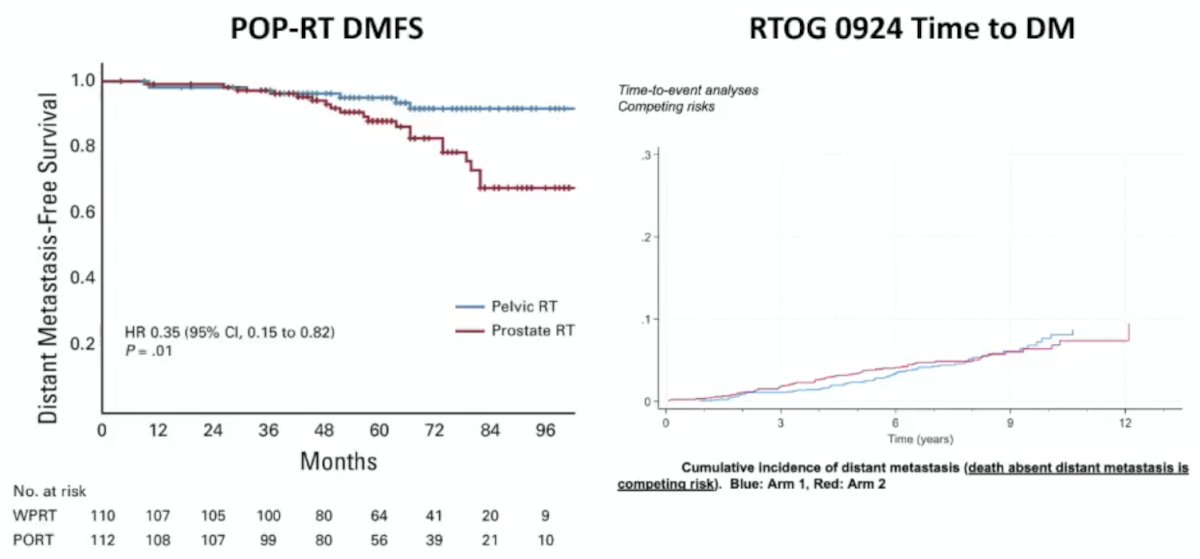
Dr. Michalski states that we have seen this pattern before, specifically when considering elective pelvic lymph node irradiation. The POP-RT trial2 included 224 high or very high risk patients, with a lymph node risk >20%, a median PSA of 28 ng/mL, 80% receiving a PSMA PET/CT or FACBC scan, and 100% receiving long-term ADT. The RTOG 0924 trial included 2,473 unfavorable intermediate or high-risk patients, lymph node risk > 15%, PSA < 20 ng/mL in 84%, 100% staged with conventional imaging, and 30% of patients on long-term ADT. POP-RT reported an improvement in distant metastasis-free survival for elective pelvic nodal irradiation (HR 0.35, 95% CI 0.15-0.82), whereas RTOG 0924 showed no difference in time to distant metastases:
Dr. Michalski states that this may be secondary to:
- A greater disease burden benefits from more intense therapy
- An interaction between pelvic radiotherapy and ADT may manifest in patients with a greater disease burden
- This principle may apply to the intensification of systemic therapy (ie. androgen receptor pathway inhibitor)
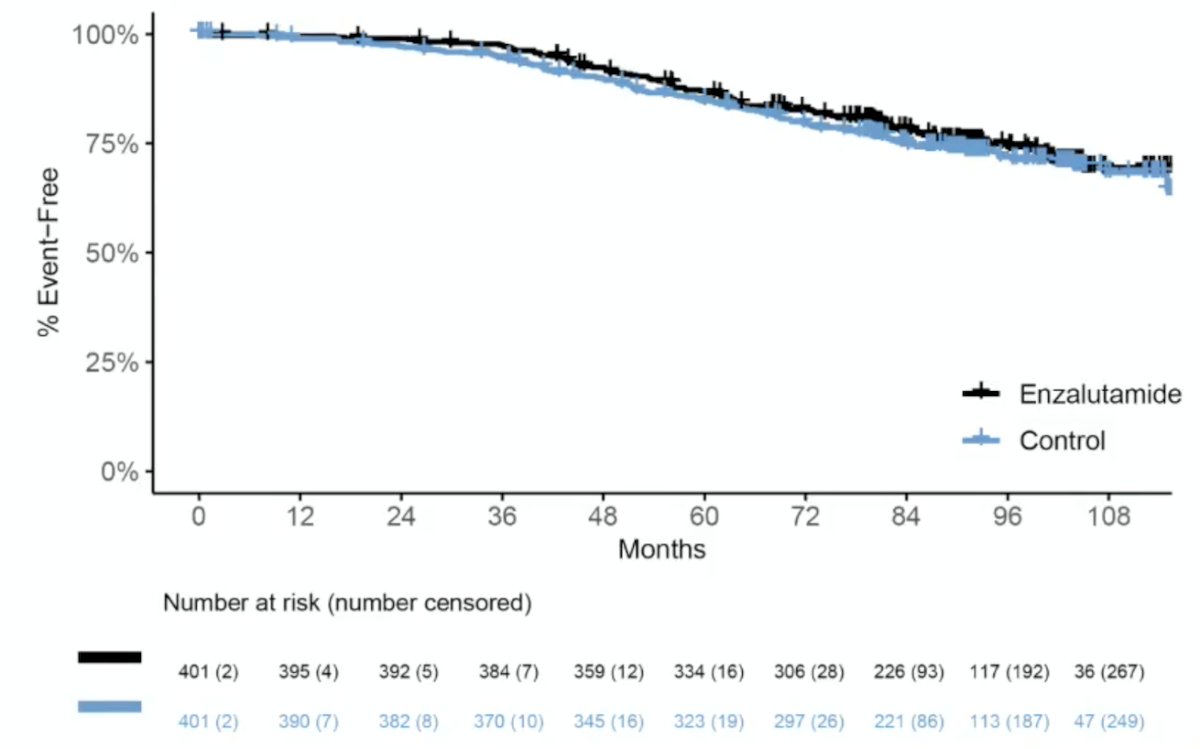
In ENZARAD, patients failed to meet the primary endpoint of a metastasis-free survival benefit (8-year: 74% versus 72%; HR 0.88, 95% CI: 0.67–1.15, p = 0.34):
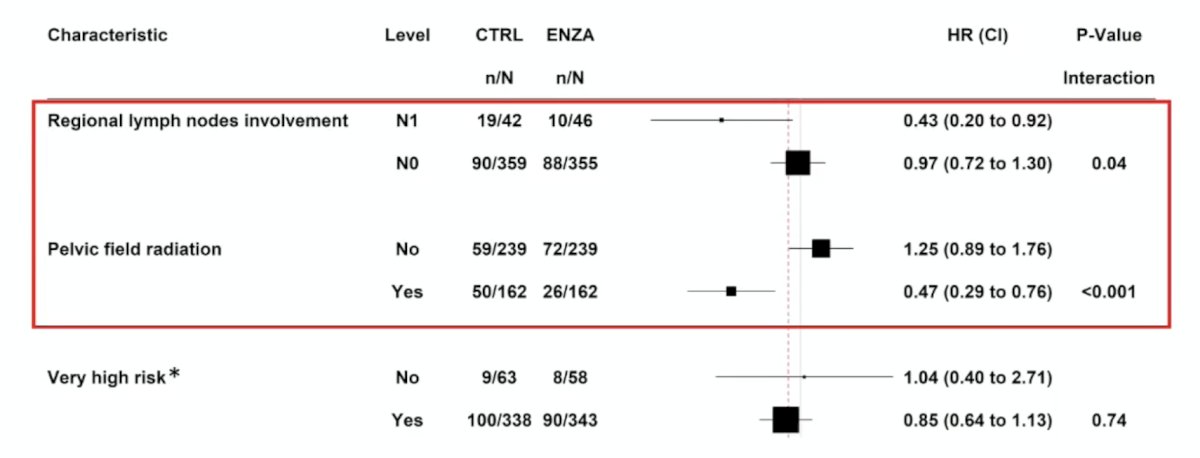
Subgroup analyses from ENZARAD demonstrated that a significant metastasis free survival benefit may be observed in patients with regional lymph node involvement (cN1; HR 0.43, 95% CI: 0.20–0.92) and those with planned pelvic field radiation (HR 0.47, 95% CI: 0.29–0.76), but with no benefit among those with ‘very high-risk’ disease (HR 0.85, 95% CI: 0.64–1.13):
Biomarkers will be important to select patients who may benefit from the addition of an androgen receptor pathway inhibitor, including multimodal artificial intelligence (MMAI) models:
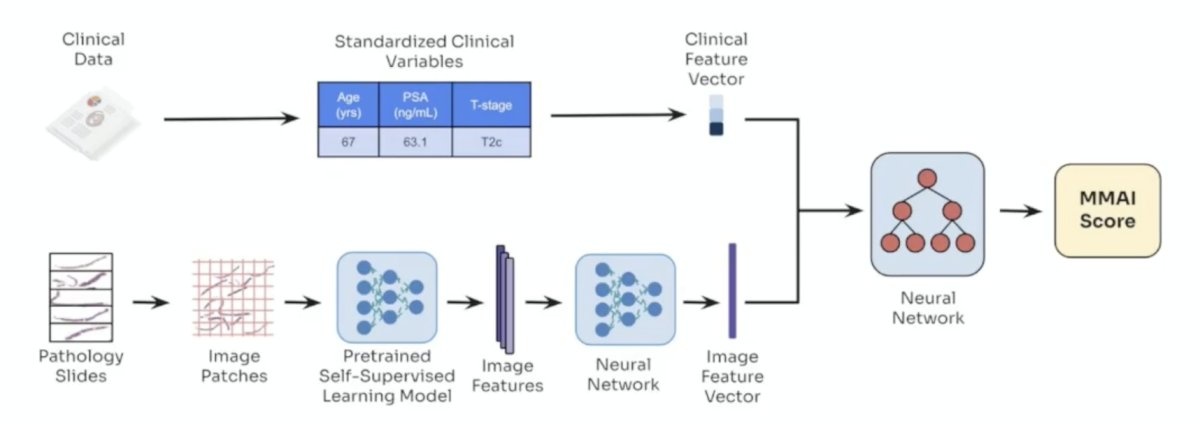
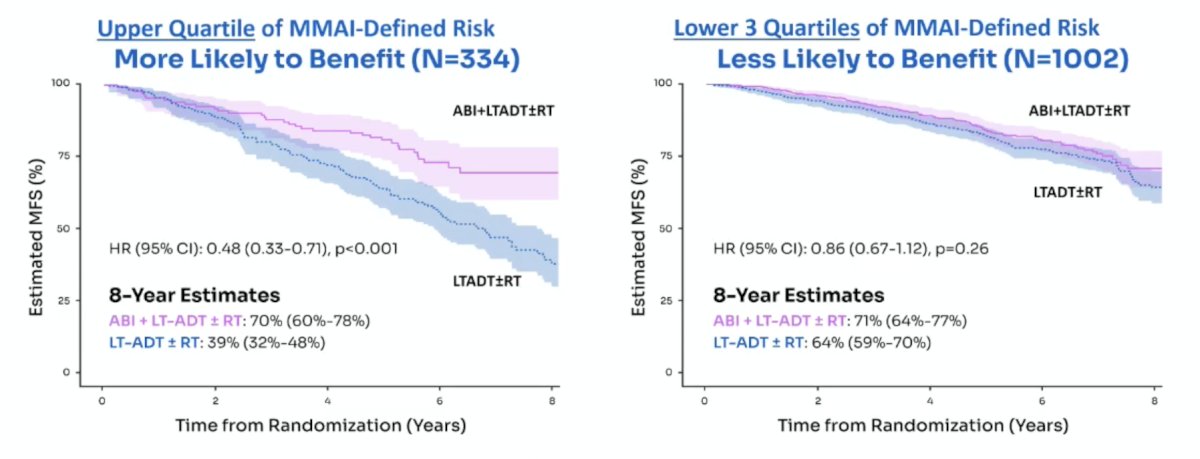
At ASCO 2025, Dr. Nicholas James presented data from STAMPEDE assessing an MMAI model to identify patients that may benefit from an androgen receptor pathway inhibitor in high-risk non-metastatic prostate cancer patients. M0 patients with MMAI scores in the upper quartile of risk were significantly more likely to benefit from the addition of abiraterone, with a hazard ratio for metastasis-free survival of 0.48 (95% CI 0.33–0.71; p < 0.001). Notably, the interaction between MMAI risk score and treatment effect was statistically significant (interaction p = 0.01), supporting the potential role of MMAI as a predictive biomarker to guide selective treatment intensification with abiraterone in high-risk prostate cancer:
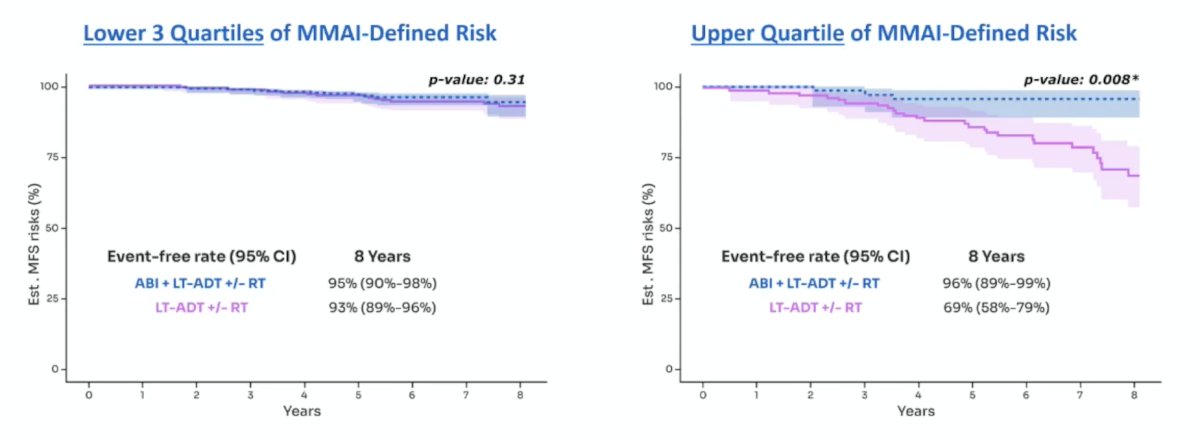
The differential treatment benefit from abiraterone remained evident even within the more clinically homogeneous subgroup of N0M0 patients. Those with MMAI scores in the upper quartile of risk were significantly more likely to benefit from the addition of abiraterone, reinforcing the score’s predictive value. In this subgroup, the MMAI-treatment interaction effect remained statistically significant (p = 0.02):
Adverse events >= grade 3 in ENZARAD and STAMPEDE are also noteworthy:
- ENZARAD
- Fatigue: 4% versus 1.5%
- Hypertension: 11% versus 6%
- Nervous system: 6% versus 4%
- STAMPEDE
- Fatigue: 10% versus 2%
- Hypertension: 14% versus 5%
- Transaminase: 13% versus 5%
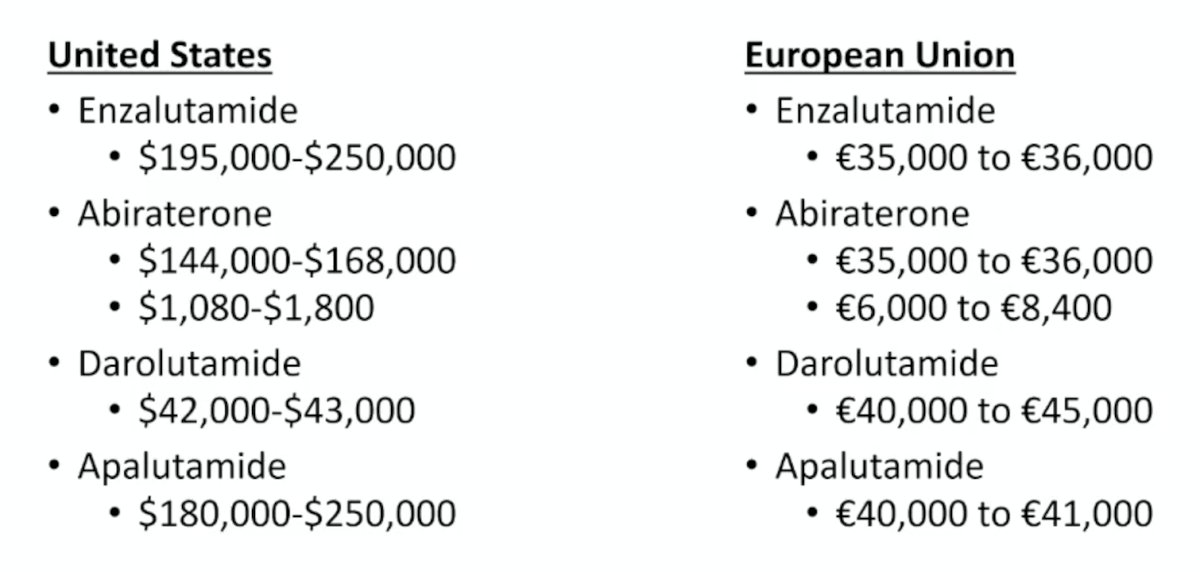
Additionally, the cost of one year of androgen receptor pathway inhibitors can be expensive in both the United States and the European Union, as highlighted below:
Dr. Michalski concluded his presentation discussing that patients with high-risk localized prostate cancer do not need the addition of an androgen receptor pathway inhibitor to radiotherapy + ADT with the following take-home points:
- Androgen receptor pathway inhibitor use in all patients with high-risk prostate cancer is:
- Unnecessary
- Toxic
- Expensive
- Selective use for patients is appropriate, specifically:
- Node positive and patients deemed to benefit from whole pelvis radiotherapy
- Biomarker-positive patients
- PROTEUS is pending readout for high-risk prostate cancer +/- androgen receptor pathway inhibitor and will provide additional data in this disease space
Presented by: Jeff Michalski, MD, MBA, FACR, FASTRO, Professor, Washington University School of Medicine, St. Louis, MO
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:- Attard G, Murphy L, Clarke NW, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: A meta-analysis of primary results from two randomized controlled phase 3 trials of the STAMPEDE platform protocol. Lancet 2022 Jan 29;399(10323):447-460.
- Murthy, V, Maitre P, Kannan S, et al. Prostate-only versus whole-pelvic radiation therapy in high-risk and very high-risk prostate cancer (POP-RT): Outcomes from phase III randomized controlled trial. J Clin Oncol. 2021;39:1234-1242.