(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a high risk and locally advanced prostate cancer session and a presentation by Dr. Christopher Sweeney discussing that patients with high-risk localized prostate cancer need the addition of an androgen receptor pathway inhibitor to radiotherapy + ADT. Dr. Sweeney started his portion of the debate by highlighting that in 2019, Yaxley et al.1 assessed the number of men with 68Ga-PSMA PET/CT avid metastasis at diagnosis among 1,253 consecutive men referred for treatment.
Metastatic disease was identified in 12.1% of men, including 8.2% with a PSA level of <10 ng/mL and 43% with a PSA level of >20 ng/mL. Metastases were identified in 6.4% with ISUP grade 2-3 and 21% with ISUP grade 4-5. Lymph node metastases were suspected in 107 men, with 47.7% outside the boundaries of an extended pelvic lymph node dissection. Moreover, skeletal metastases were identified in 4.7%. In men with intermediate-risk prostate cancer, metastases were identified in 5.2%, compared to 19.9% with high-risk disease. Thus, is there a role for adjuvant ADT + androgen receptor pathway inhibitor for “M0 conventional imaging” but PSMA PET positive disease beyond the prostate?
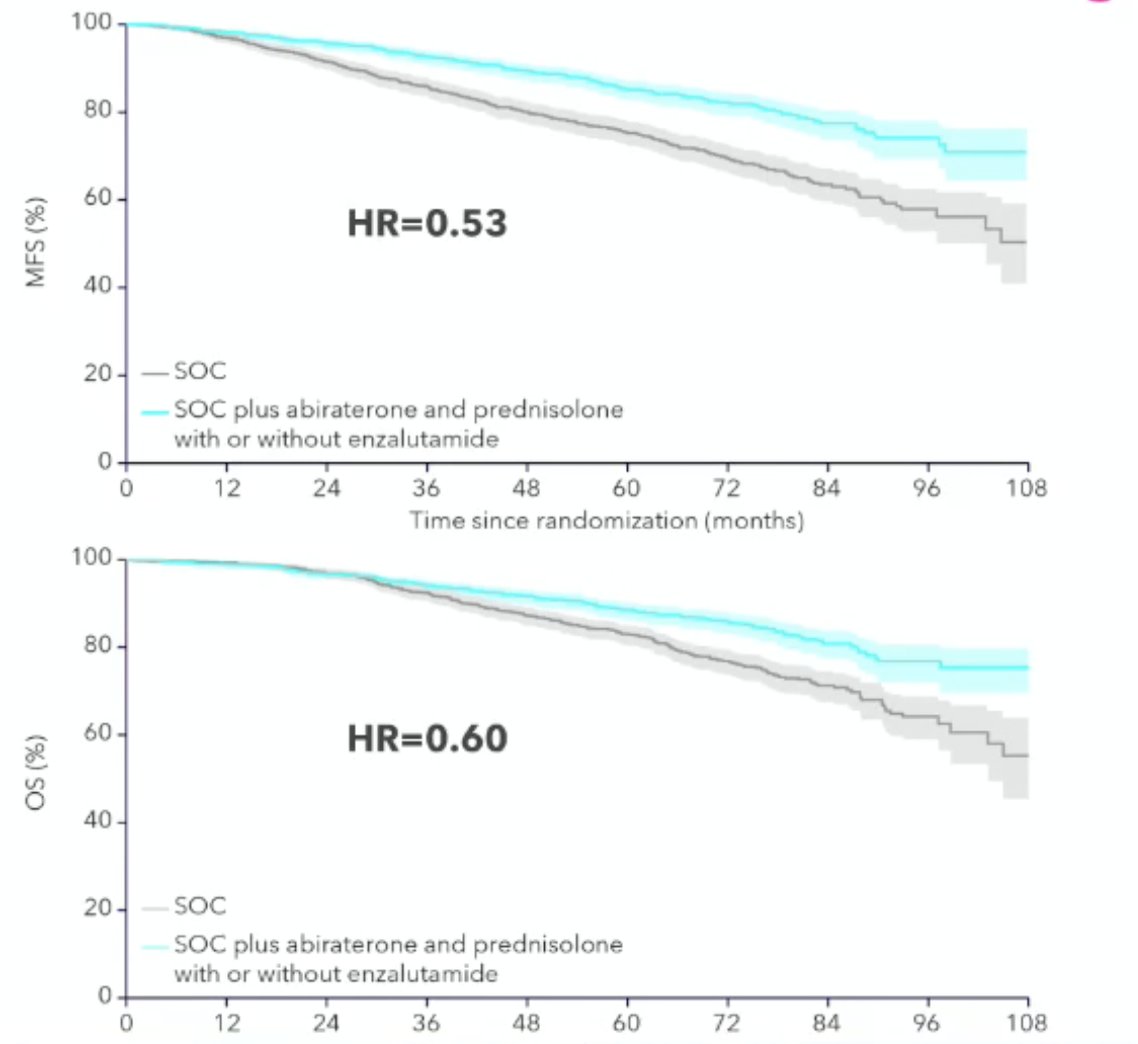
Dr. Sweeney notes that in the STAMPEDE arm of high-risk localized prostate cancer treated with either abiraterone or enzalutamide, there was a consistent effect with an androgen receptor pathway inhibitor regardless of metastatic burden.2 In this study, local radiotherapy (74 Gy in 37 fractions to the prostate and seminal vesicles or the equivalent using hypofractionated schedules) was mandated for node negative and encouraged for node positive disease. There were 1,974 patients randomized and over a median follow-up of 72 months (IQR 60–84), metastasis-free survival was significantly longer in the combination therapy groups (median not reached, IQR NE–NE) than in the control groups (not reached, 97–NE; HR 0.53, 95% CI 0.44–0.64). The 6-year metastasis-free survival was 82% (95% CI 79–85) in the combination-therapy group and 69% (66–72) in the control group. The overall survival median was not reached (IQR NE–NE) in the combination therapy groups versus not reached (IQR 103–NE) in the control groups (HR 0.60, 95% CI 0.48–0.73):
During this time period of patients accruing to STAMPEDE, no PSMA PET/CTs were done, resulting in two hypotheses:
- Many patients are PSMA PET positive despite no disease on CT or bone scan
- There needs to be a prospective evaluation for patients who are M0 on conventional imaging but PSMA PET/CT positive versus PSMA PET/CT negative beyond pelvic lymph nodes
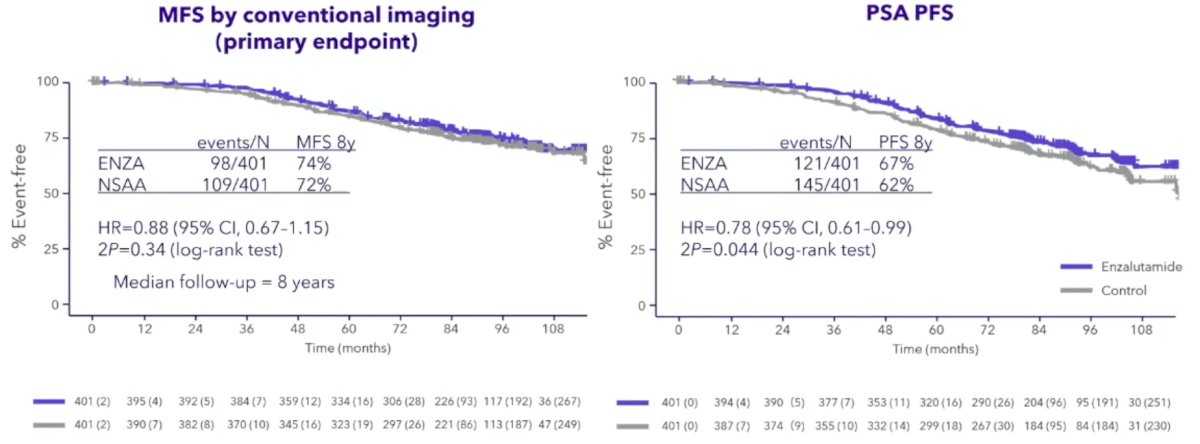
Dr. Sweeney then discussed the ENZARAD trial, which was initially presented at ESMO 2025. In ENZARAD, men with high-risk, localized prostate cancer suitable for external beam radiotherapy were randomized to: (i) enzalutamide (160 mg daily x 24 months) + LHRH agonist (24 months) + prostate external beam radiotherapy +/- brachytherapy +/- nodal irradiation 16 weeks after starting hormonal therapy versus (ii) conventional non-steroidal antiandrogen (6 months) + LHRH agonist (24 months) + prostate external beam radiotherapy +/- brachytherapy +/- nodal irradiation 16 weeks after starting hormonal therapy. Among 802 patients, 12% of patients had cN1 disease by conventional imaging, 90% had Gleason Score 8-10 disease, and 36% had a PSA level >20 ng/ml. Moreover, 40% were planned for pelvic radiotherapy, and 8% were planned for a brachytherapy boost. ENZARAD failed to meet its primary endpoint of a metastasis free survival benefit (8-year: 74% versus 72%; HR 0.88, 95% CI: 0.67–1.15, p = 0.34), although a significant progression free survival benefit was observed in favor of enzalutamide (8-year: 67% versus 62%; HR 0.78, 95% CI: 0.61–0.99, p = 0.044):
ENZARAD also showed no difference in overall survival (HR 0.87, 95% CI 0.63–1.20) and no difference in prostate cancer-specific survival (HR 0.90, 95% CI 0.41–1.97):
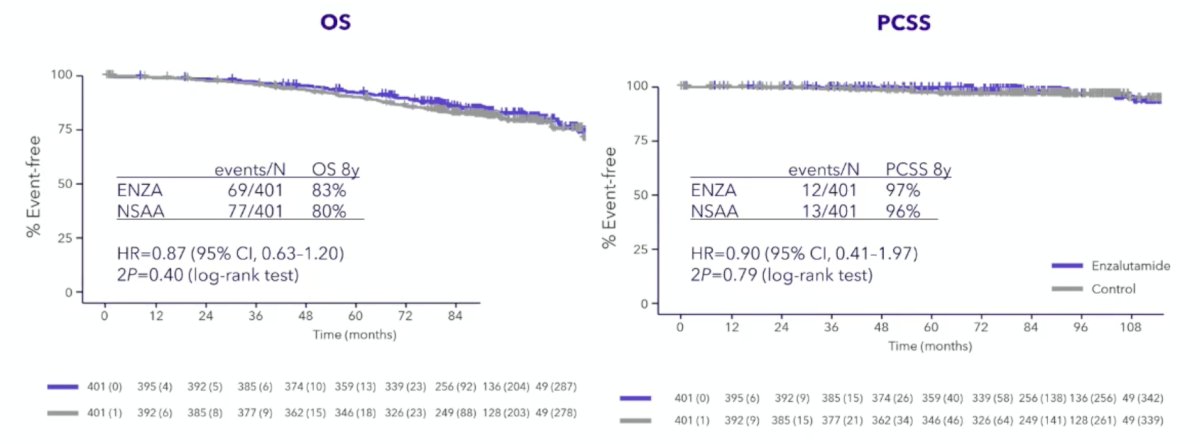
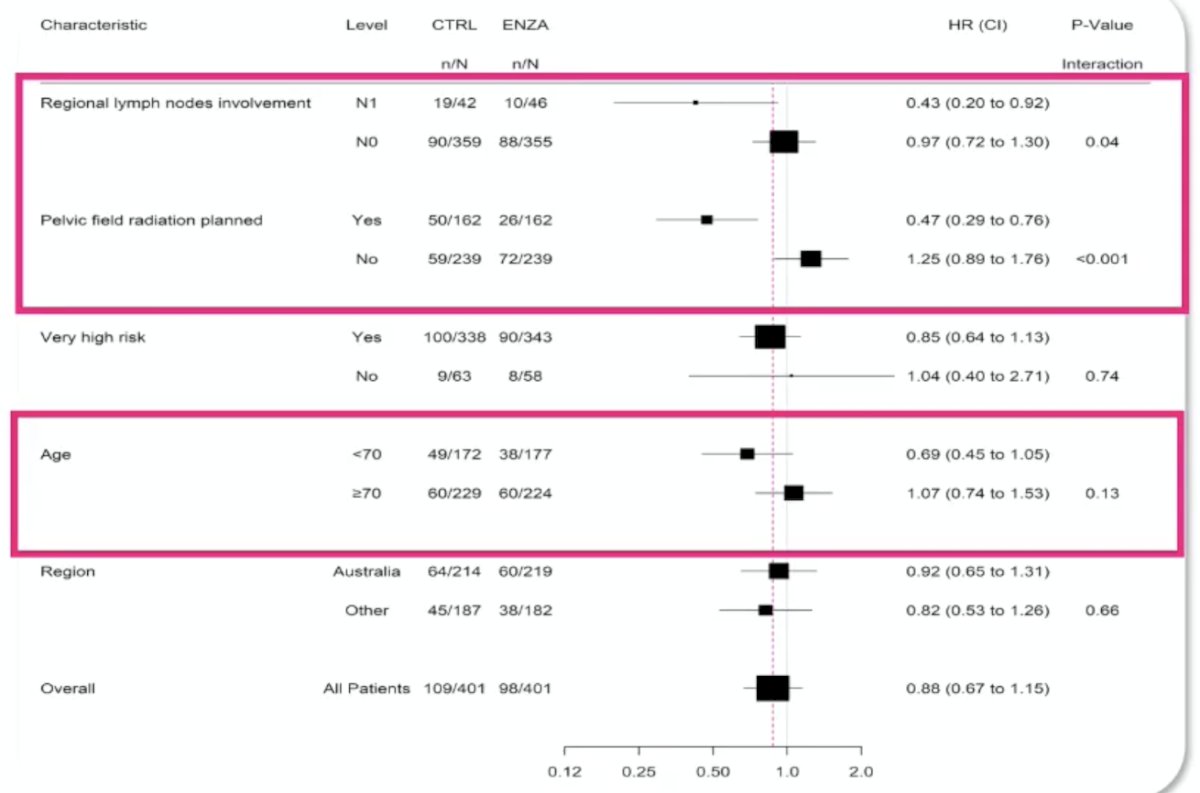
Dr. Sweeney notes that only 27% of patients in the control arm and 22% of patients in the enzalutamide arm had PSA progression by 8 years, resulting in ~3% prostate cancer mortalities. Subgroup analyses demonstrated that a significant metastasis free survival benefit may be observed in patients with regional lymph node involvement (cN1; HR 0.43, 95% CI: 0.20–0.92) and those with planned pelvic field radiation (HR 0.47, 95% CI: 0.29–0.76), but with no benefit among those with ‘very high-risk’ disease (HR 0.85, 95% CI: 0.64–1.13):
Dr. Sweeney emphasized that the ENZARAD benefit in cN1 patients is consistent with STAMPEDE, although ENZARAD enrolled “less poor” poor-risk patients:
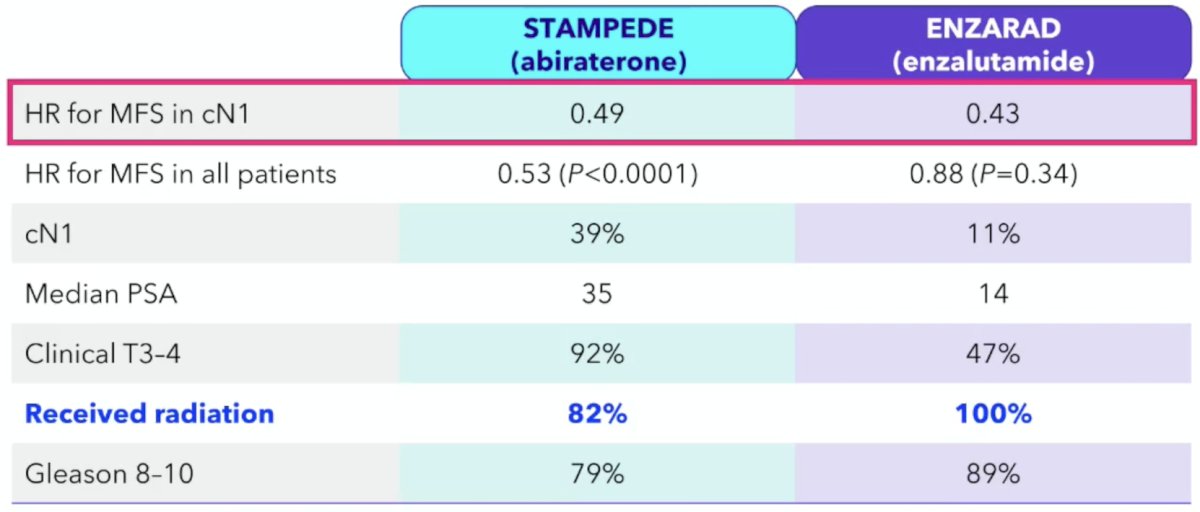
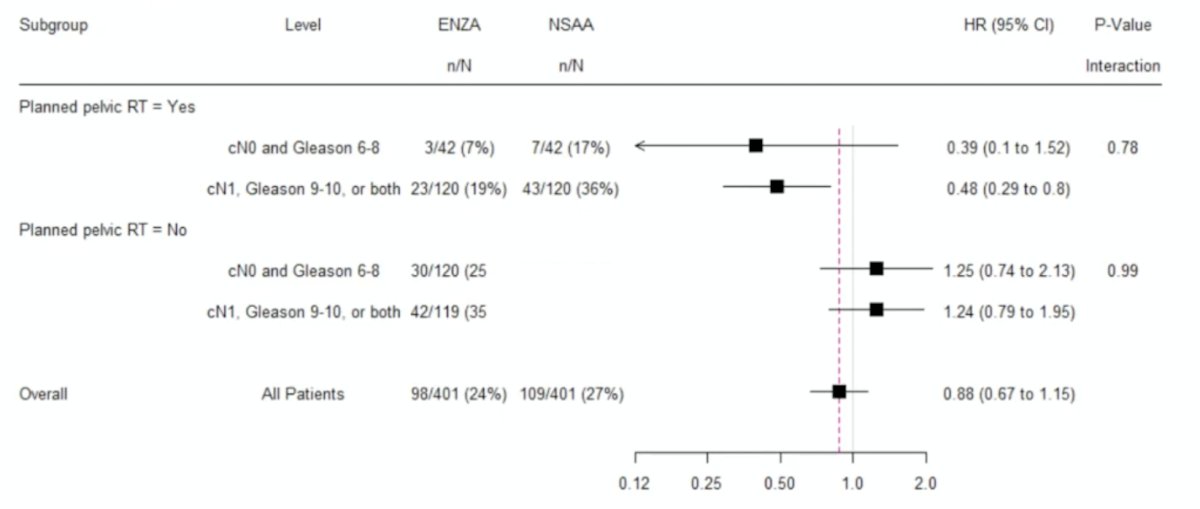
Additionally, in ENZARAD, the effect of enzalutamide did not appear to vary by clinical features within groups defined by pelvic radiotherapy status:
However, when looking at the outcomes for all patients treated with pelvic radiation, there was a 9% absolute improvement in 5-year metastasis-free survival with the addition of enzalutamide, as well as a 9% absolute improvement in 8-year overall survival:

Dr. Sweeney described two hypotheses arising from the observation of metastasis-free survival and overall survival benefits from adding enzalutamide to ADT + external beam radiotherapy:
- Do physicians intuitively select patients with very high-risk disease who benefit from pelvic radiation and enzalutamide eradicated micrometastatic disease?
- Is there a biological interaction between pelvic radiation and ADT + potent androgen inhibition (ie, amplification of an anti-cancer systemic (abscopal) immune response)?
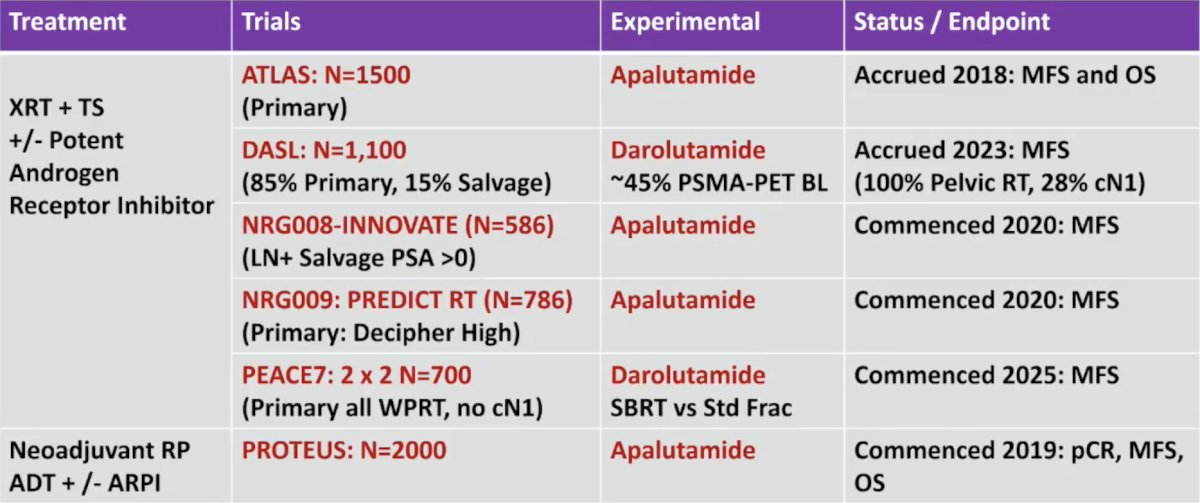
Post-ENZARAD, Dr. Sweeney emphasized that there is a plethora of data coming in this disease space, including the first results of PROTEUS being presented at ASCO 2026:
With the advent of (i) more effective and convenient local therapy (ie. radiation and surgery), (ii) more effective systemic therapy for biochemical relapse, mHSPC, nmCRPC, and mCRPC, (iii) PSMA PET/CT imaging to identify micrometastatic disease (especially regional lymph nodes even if not cN1 who may benefit from pelvic radiation + enzalutamide), and (iv) molecular biomarkers (ie. RNA profiling), the previous definitions of high risk localized disease are no longer associated with high risk of death from prostate cancer, but still associated with a high risk of relapse, which often leads to anxiety, life-long monitoring, and therapy (including castration). New endpoints are needed to document the benefit from preventing a biochemical relapse: “freedom from clinical detriment” with similar or improved metastasis-free survival and/or overall survival.
Dr. Sweeney concluded his presentation discussing that patients with high-risk localized prostate cancer need the addition of an androgen receptor pathway inhibitor to radiotherapy + ADT, with the following take-home points:
- Future research should and will focus on optimizing therapy with imaging and molecular biomarkers such that we can avoid “castration” where possible and cure men:
- With truly localized disease with low morbidity and convenient localized therapy only
- With solely androgen receptor-driven micrometastatic disease, with an androgen receptor pathway inhibitor alone without testosterone suppression
- With less androgen receptor sensitive micrometastatic disease with:
Presented by: Christopher Sweeney, MBBS, Director, South Australian ImmunoGENomics Cancer Institute (SAIGENCI), Professor of Medicine, University of Adelaide, Consulting Medical Oncologist, Royal Adelaide Hospital in Adelaide, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:- Yaxley JW, Raveenthiran S, Nouhaud FX, et al. Risk of metastatic disease on 68 gallium-prostate-specific membrane antigen positron emission tomography/computed tomography scan for primary staging of 1253 men at the diagnosis of prostate cancer. BJU Int. 2019 Sep;124(3):401-407.
- Attard G, Murphy L, Clarke NW, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: A meta-analysis of primary results from two randomized controlled phase 3 trials of the STAMPEDE platform protocol. Lancet 2022 Jan 29;399(10323):447-460.