(UroToday.com) The 2026 PSMA & Beyond conference featured a session on challenges of radioligand therapy and a presentation by Dr. Michael Hofman discussing the expansion of the theranostic dream. Only 8 years ago, in 2018, PSMA PET before and after 177Lu-PSMA-617 in 8 patients won image of the year for the Journal of Nuclear Medicine.
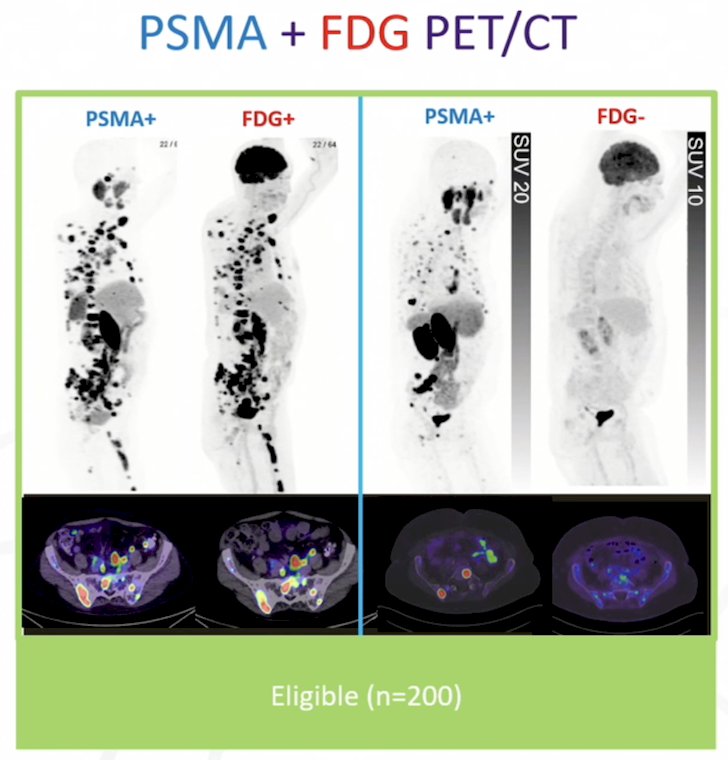
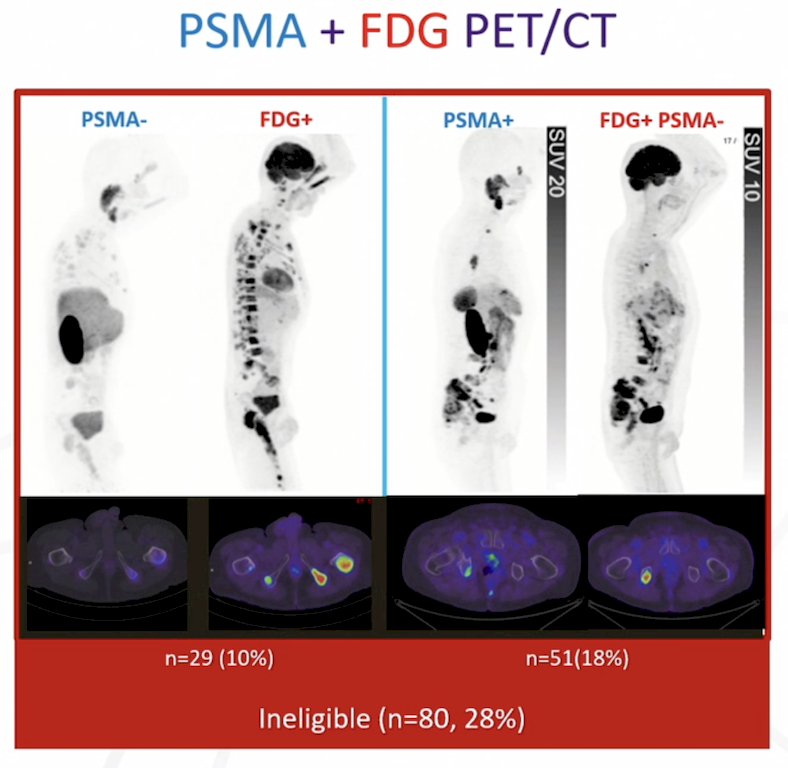
The TheraP trial1 was the first randomized study to evaluate 177Lu-PSMA-617 versus cabazitaxel for men with metastatic castration resistant prostate cancer (mCRPC) after docetaxel. In this open label, phase II trial, 200 men were randomized to either 177Lu-PSMA-617 or cabazitaxel. To screen into the study, all men had both 68Ga-PSMA-11 and 18F-FDG PET/CT and were required to have high PSMA-expression (at least one site with SUVmax ≥ 20) and no sites of FDG-positive/PSMA-negative disease:
All patients had progressive disease with rising PSA ≥ 20 ng/mL after docetaxel, and 91% had received prior enzalutamide or abiraterone. Overall, 200 patients were randomized 1:1 to 177Lu-PSMA-617 6-8 GBq every 6 weeks for up to 6 cycles of therapy or cabazitaxel 20 mg/m2 every 3 weeks for up to 10 cycles. Patients were stratified based on disease burden and prior anti-androgen therapy.
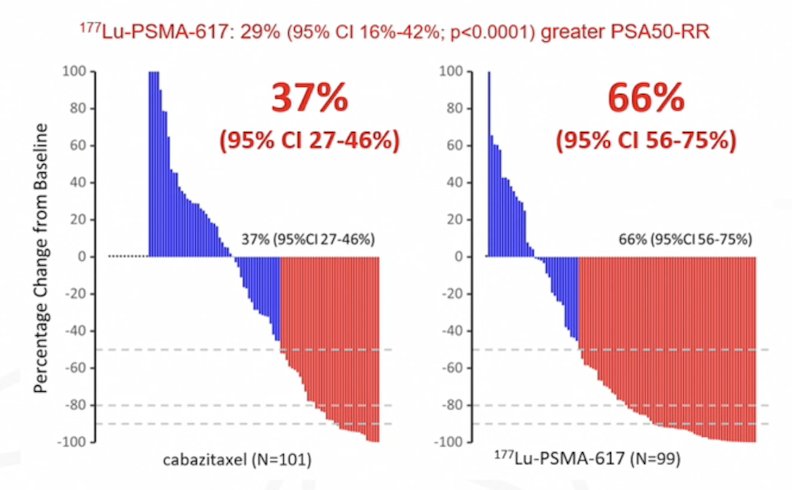
The primary endpoint of this study was a PSA decline of 50% (PSA50), and secondary endpoints included PSA progression free survival and overall survival. After a median follow up of 13 months, 177Lu-PSMA-617 significantly improved PSA progression free survival compared with cabazitaxel (HR 0.63, 95% CI 0.46 to 0.86) and had a much higher PSA50 rate (66% versus 37%):
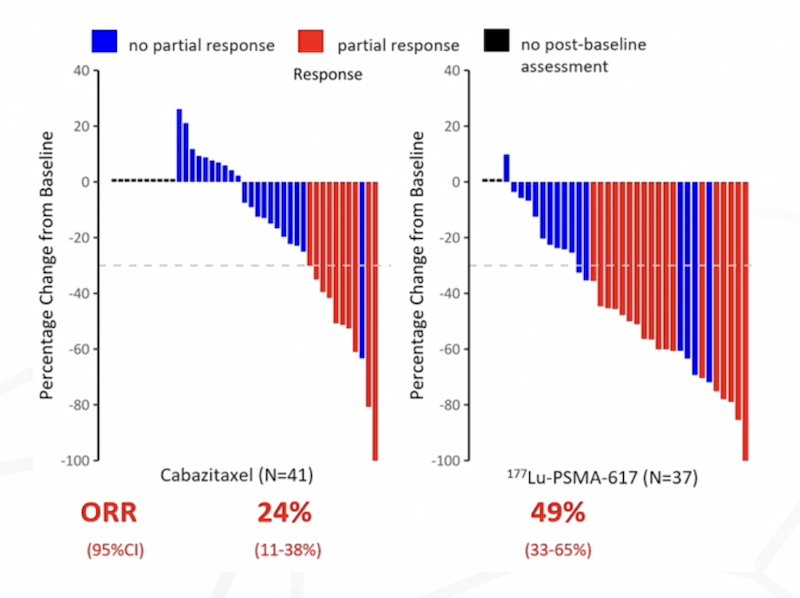
According to RECIST 1.1, the objective response rate was 24% for cabazitaxel compared to 49% for 177Lu-PSMA-617:
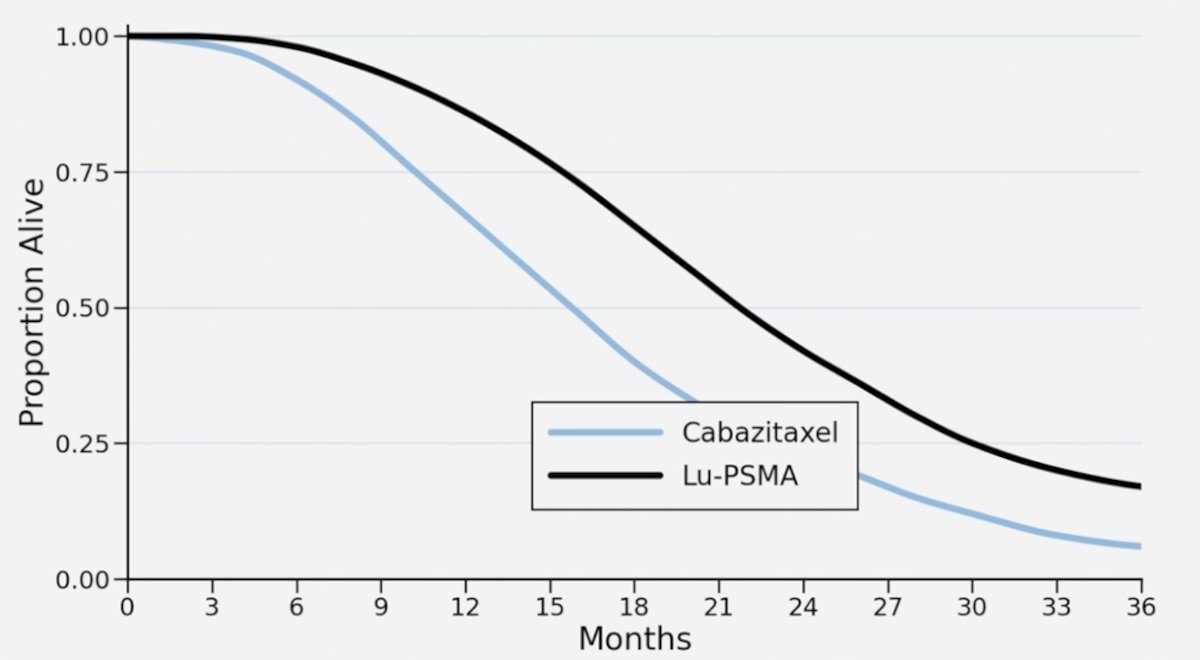
Based on these PSA and RECIST responses, Dr. Hofman states that they expected the overall survival curve for TheraP to look like this:
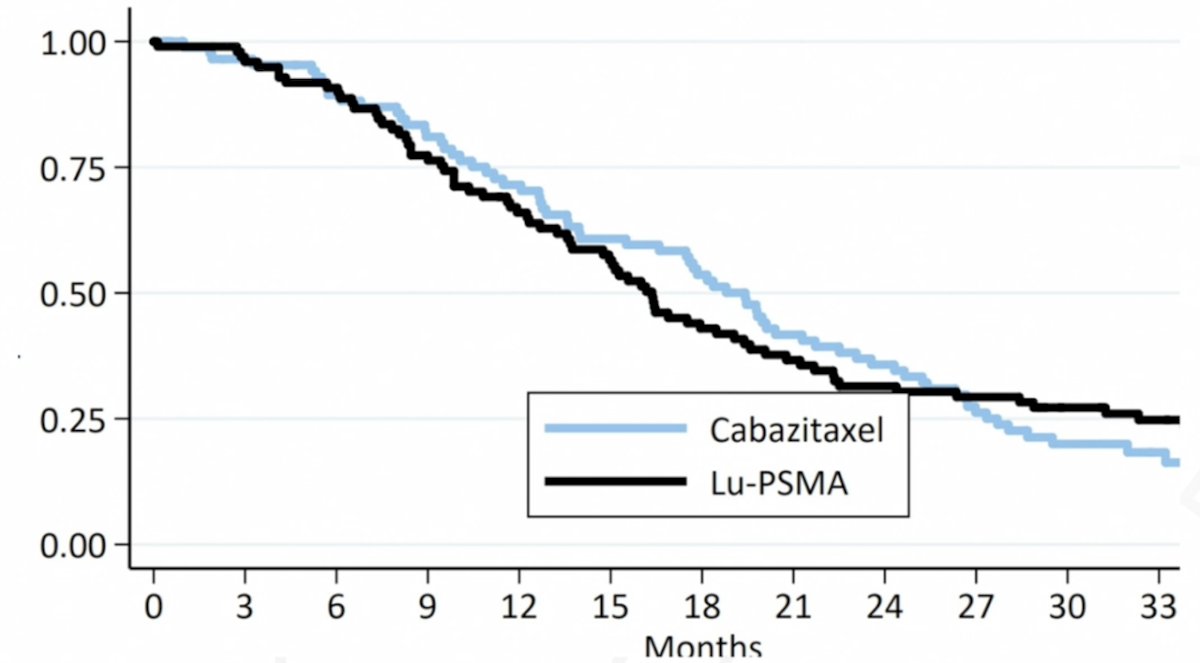
But what they found was that there was no overall survival benefit for 177Lu-PSMA-617 versus cabazitaxel:
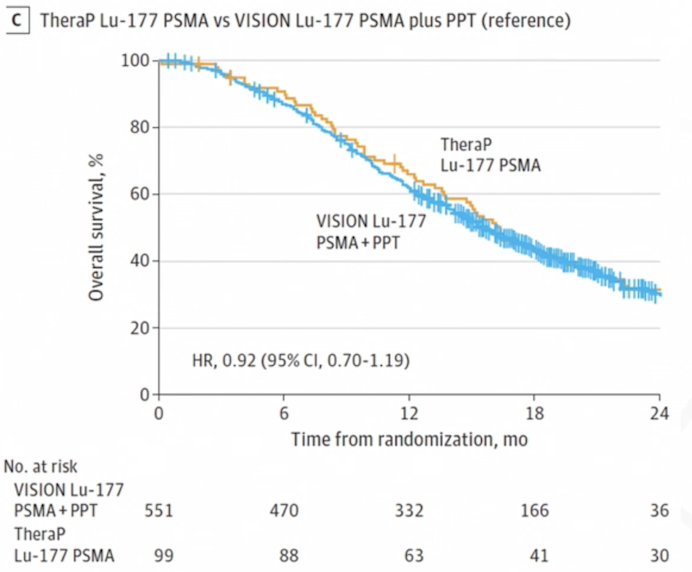
In 2024, Dr. Hofman and colleagues2 investigated factors associated with the observed difference in treatment effects on overall survival in the TheraP [1] and VISION3 trials, including differences in the risk of crossover from randomized treatment after disease progression. What they found suggested that the choice of comparator treatments (ie. cabazitaxel (TheraP) versus protocol permitted treatments (VISION)) may explain the difference in the observed effect of 177Lu-PSMA-617 on overall survival between the two trials:
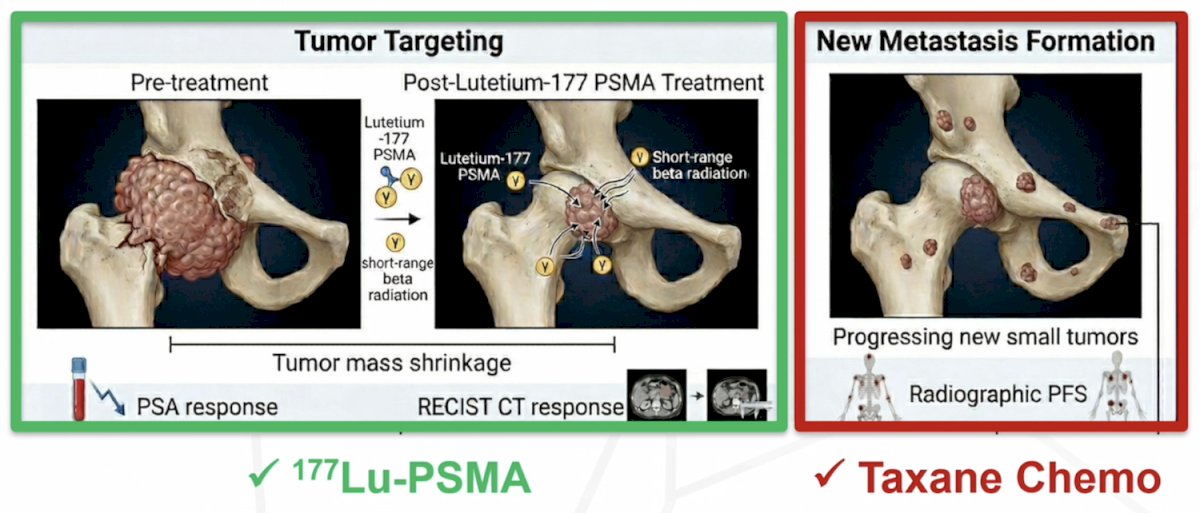
Tumor targeted 177Lu-PSMA-617 is very effective in tumor mass shrinkage and decreases PSA, however it may be less effective at stopping new metastases, which is where taxane based chemotherapy may be much better than 177Lu-PSMA-617:
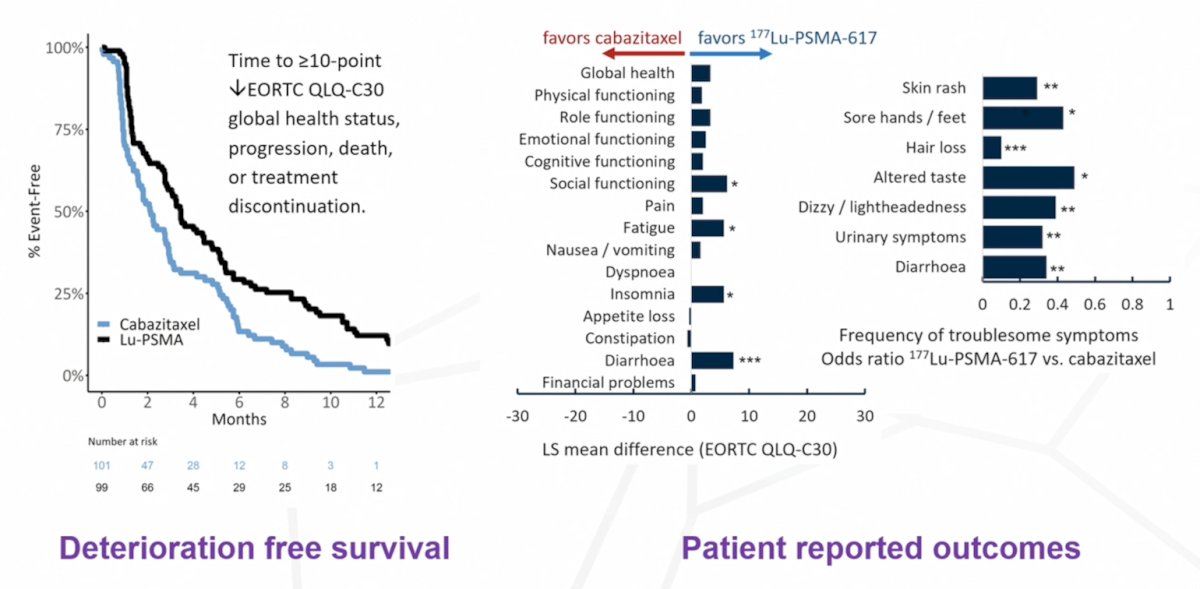
In TheraP, 177Lu-PSMA-617 was quite well tolerated compared to chemotherapy, improving deterioration free survival, and was generally favored based on patient reported outcomes:
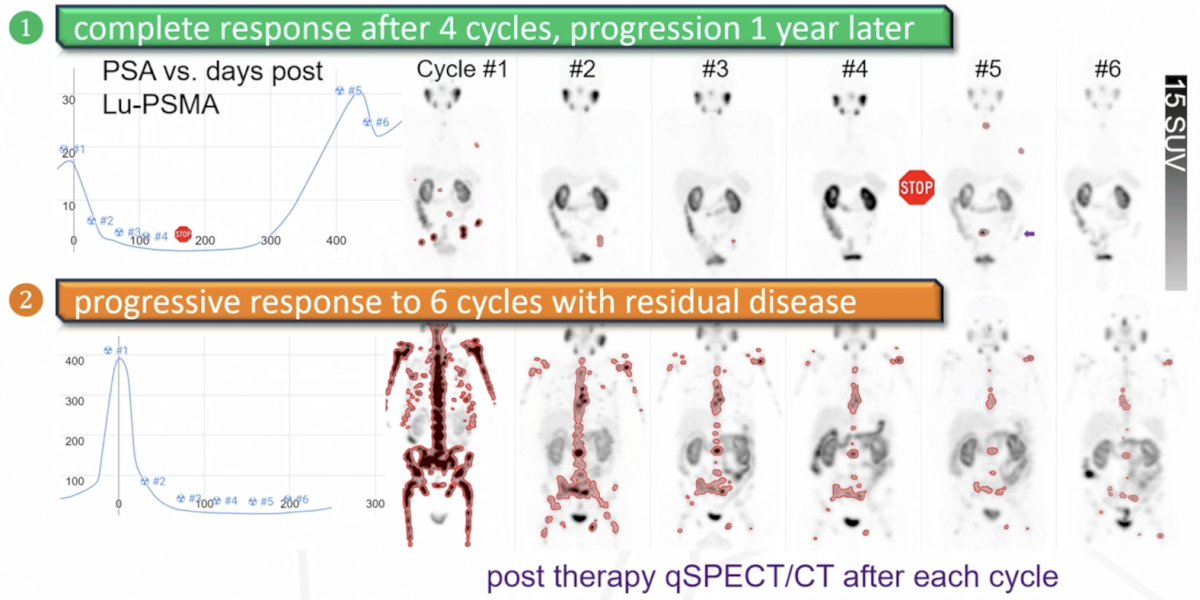
Response to 177Lu-PSMA-617 can be quite variable, with some patients having complete response after 4 cycles and progression 1 year later, or other patients having progressive response to 6 cycles with residual disease (most common):
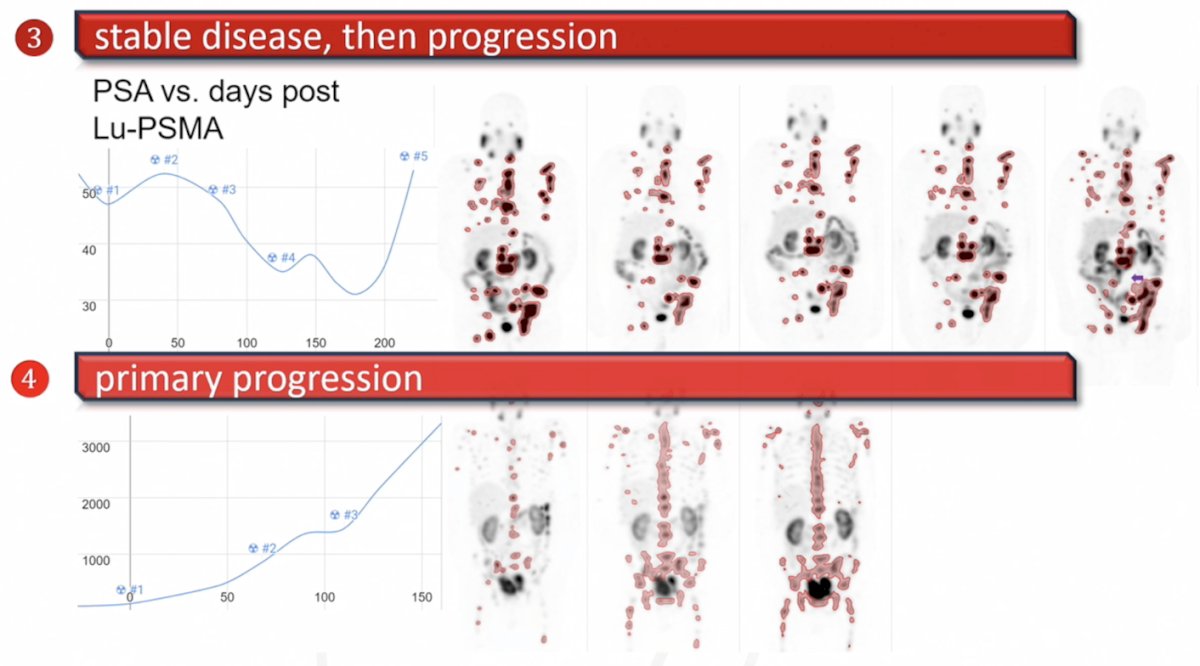
Additionally, patients may have stable disease followed by progression, and others may have no response to 177Lu-PSMA-617 and suffer from primary progression:
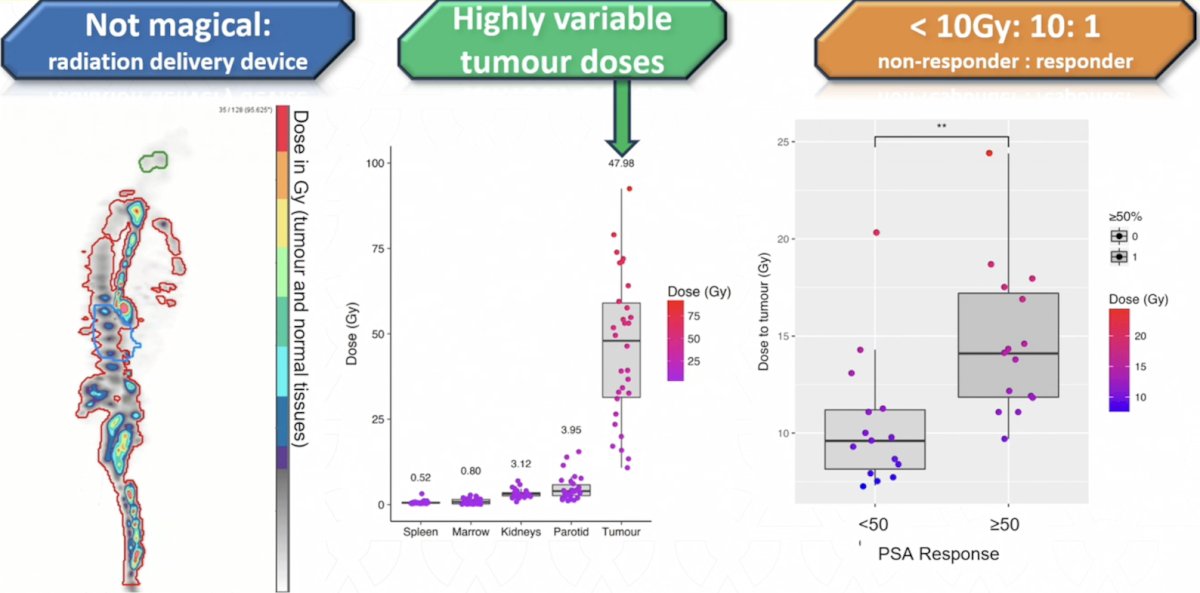
With regards to dosimetry, 177Lu-PSMA-617 is not magical in that it is a radiation delivery device, and what you see in theranostics is typically what you get. Moreover, the radiation dose to normal organs is low and normally quite predictable. But, at the tumor level, the dose to the tumor is often variable, with <10Gy being 10:1 when comparing PSA responders and non-PSA responders:
Is theranostics a drug or a type of radiotherapy? The radiotherapy model uses dosimetry to define close to critical organs and we do not exceed the known maximum tolerated limits to these critical organs. Toxicities are usually delayed, and thus, short term follow-up for toxicity is inadequate. These toxicity limitations are often extrapolated from external beam radiotherapy data. For the drug model, there is no need for dosimetry or post-treatment imaging, and the maximum tolerated dose is defined with phase 1 dose escalation studies. Acute toxicities are observable and definable; predictable, delayed cumulative toxicities may be missed.
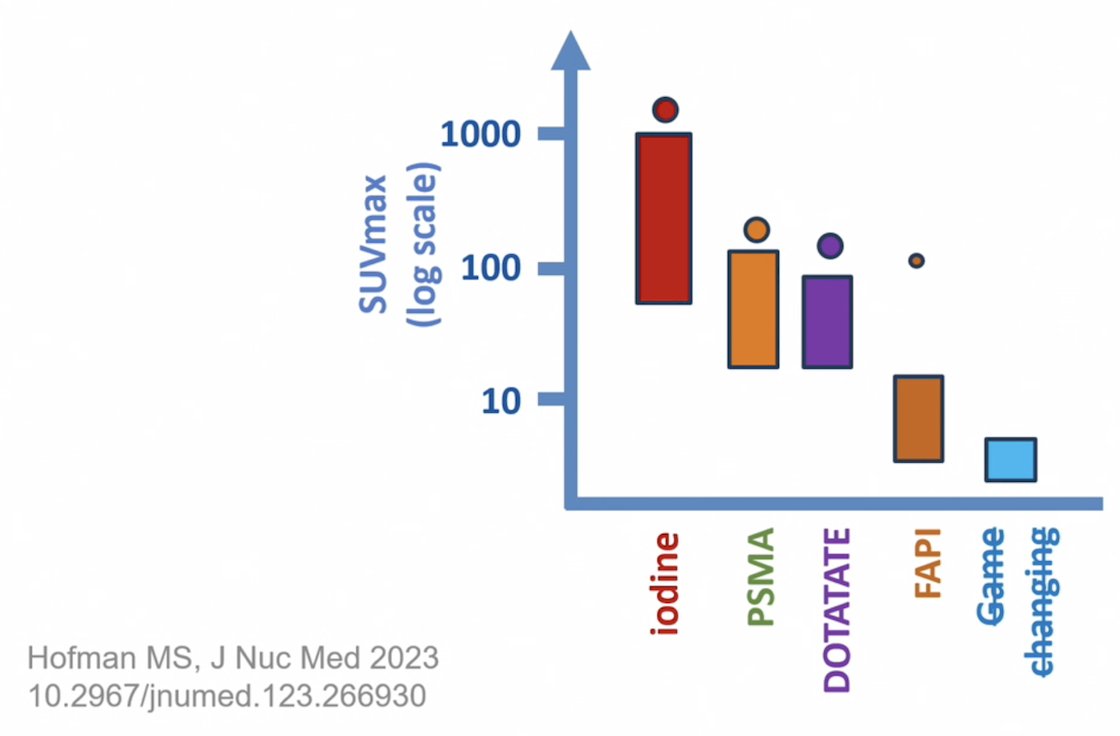
For PET imaging, Dr. Hofman discussed “Hofman’s Hierarchy of Theranostics” in that (i) we still can’t beat >80 year old iodine, although there is hope for future curative theranostics, (ii) PSMA and DOTATATE are game changers, used early, in combination, and are personalized, and (iii) compounds with low uptake will not improve outcomes and are termed theranostic zombies:
Tumor heterogeneity is a limitation of theranostics, given that PSMA PET positive lesions we can target with 177Lu-PSMA-617, whereas FDG-PET positive lesions are the most aggressive sites of disease, and we cannot target these areas. Thus, in precision medicine, patient selection is key. What PSMA and FDG imaging does enable is targeted rather than random biopsies:

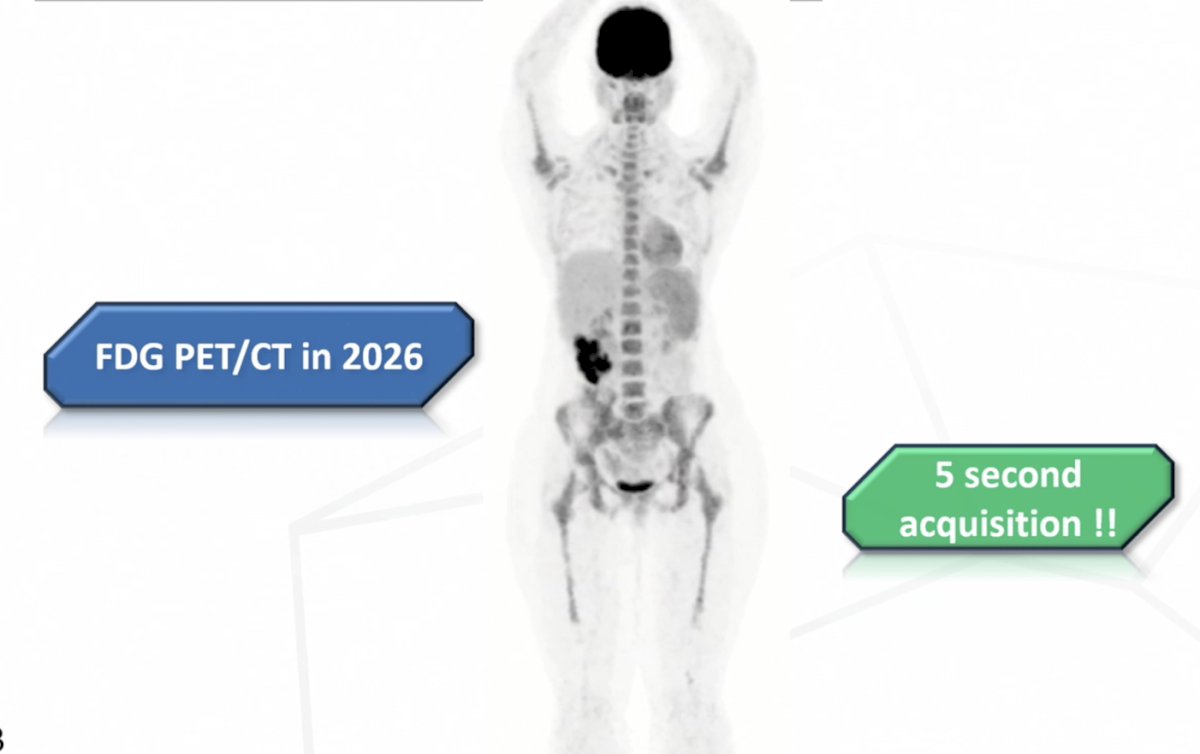
Capturing images has also significantly improved. In 1976, a whole body FDG PET would take 2 hours to acquire a poor image, whereas in 2026, an FDG PET takes less than 5 seconds to acquire excellent images:
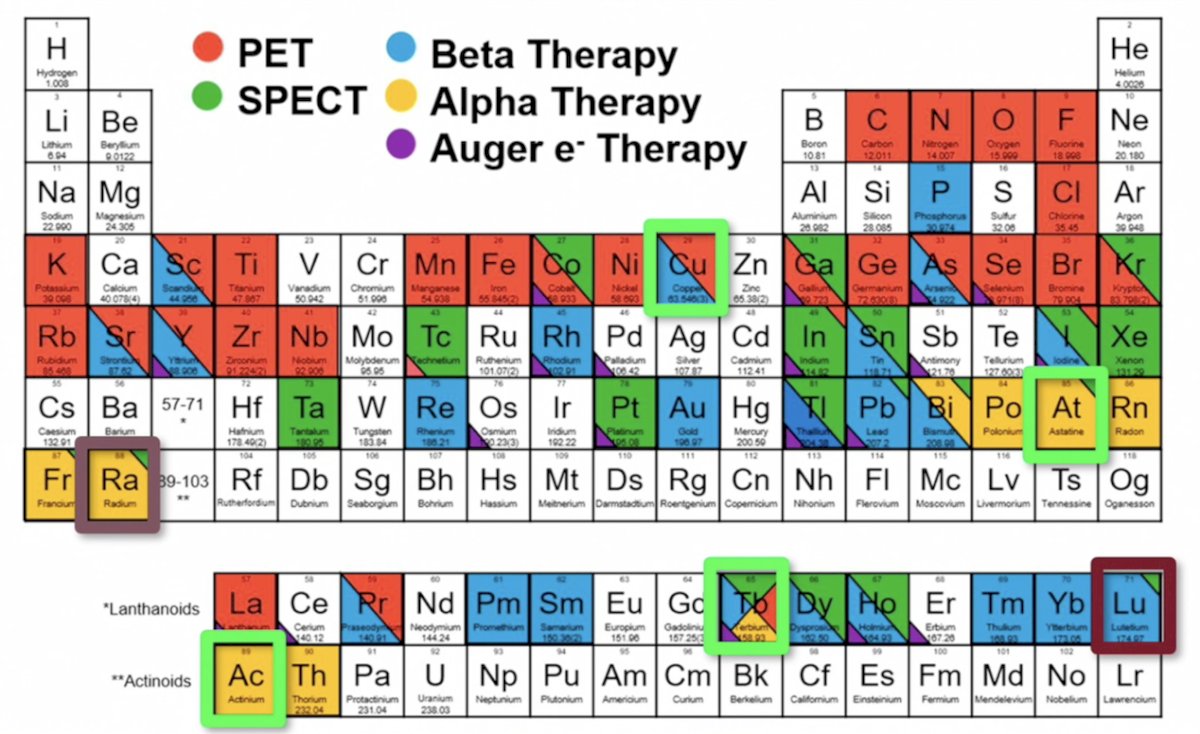
With regards to isotopes, 177Lu-PSMA-617 is a short path length beta emitter, with a mean path length of 1 mm, and an average penetration of 0.3 mm, with a median half life of 6.7 days. As a targeted drug, it is “too smart” with nearby cells not expressing the target, developing resistance. With a 1 mm path length, there is a cross fire effect, but ineffective for single cells or tumor clusters. Currently, there are many options available on the periodic table of elements for other isotope options:
In addition to monotherapy 177Lu-PSMA-617, Dr. Hofman concluded his presentation that there are many combination theranostics with PSMA, including hormone therapy, chemotherapy, immunotherapy, PARP inhibitors, radioligand therapy, surgery, and external beam radiotherapy:

Presented by: Michael Hofman, MBBS, Peter MacCallum Cancer Centre, Melbourne, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 PSMA & Beyond Conference, Los Angeles, CA, Thurs, Mar 26 – Fri, Mar 27, 2026.
Related content: The Expanding Theranostic Dream: From Hype to Hard Truths "Presentation" - Michael Hofman
References:
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.
- Soon YY, Marschner IC, Schou M, et al. Lu-177 PSMA vs Comparator Treatments and Survival in Metastatic Castration-Resistant Prostate Cancer. JAMA Netw Open. 2024 Sep 3;7(9):e2433863.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.