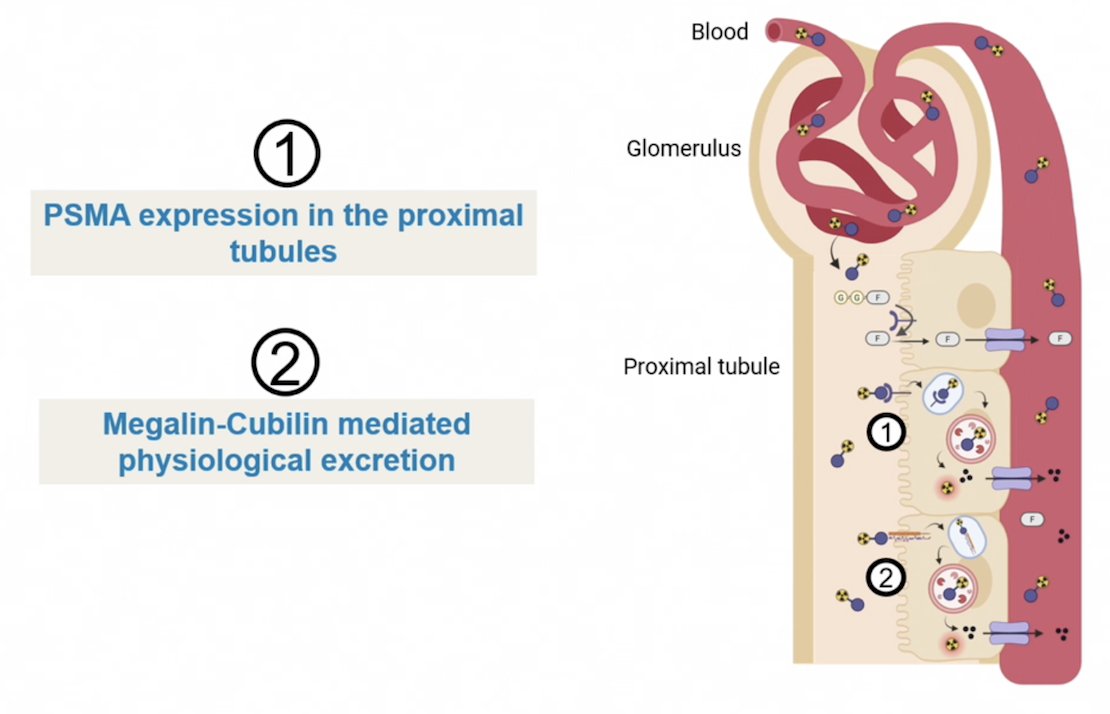
(UroToday.com) The 2026 PSMA & Beyond conference featured a session on challenges of radioligand therapy and a presentation by Dr. Inès Camille Azrour discussing renal toxicity associated with PSMA targeted therapy. PSMA functions as a transmembrane glycoprotein with both folate hydrolase and carboxypeptidase capabilities. The kidney plays an important role in the metabolism of proteins and peptides: for absorption, transport, and degradation. Of note, PSMA is expressed on the brush border of the proximal tubular cells, where it functions as a folate hydrolase to maintain folate homeostasis. In terms of radiopharmaceutical handling by the kidney, this is done by (i) PSMA expression in the proximal tubules, and (ii) by Megalin-Cubilin mediated physiological excretion:
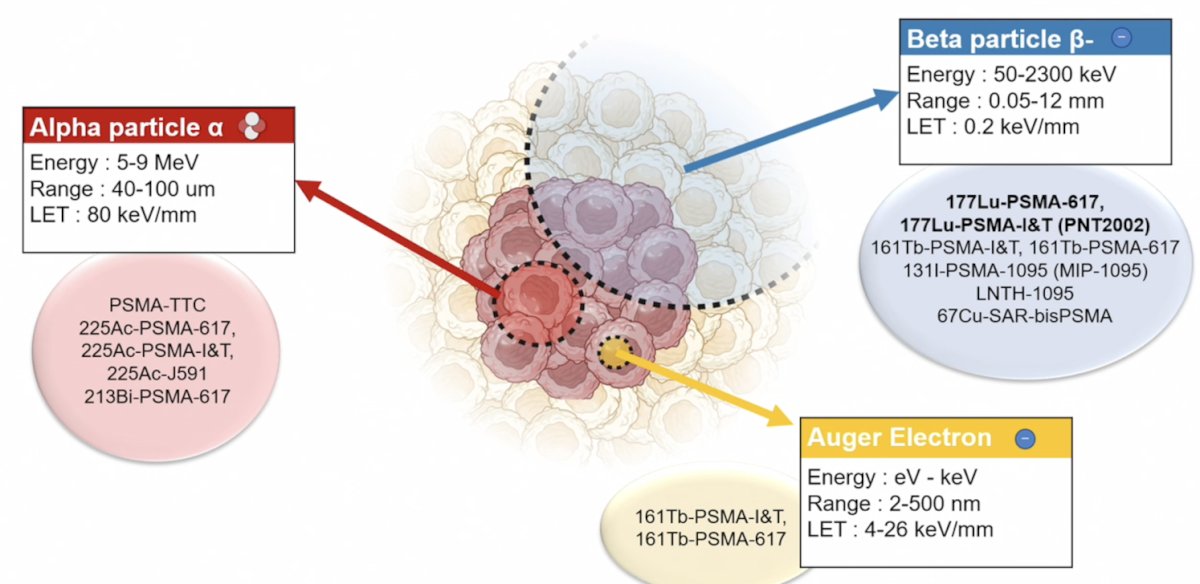
Dr. Azrour notes that radiation injury to any cell can occur by alpha particles, beta particles, and by auger electrons:
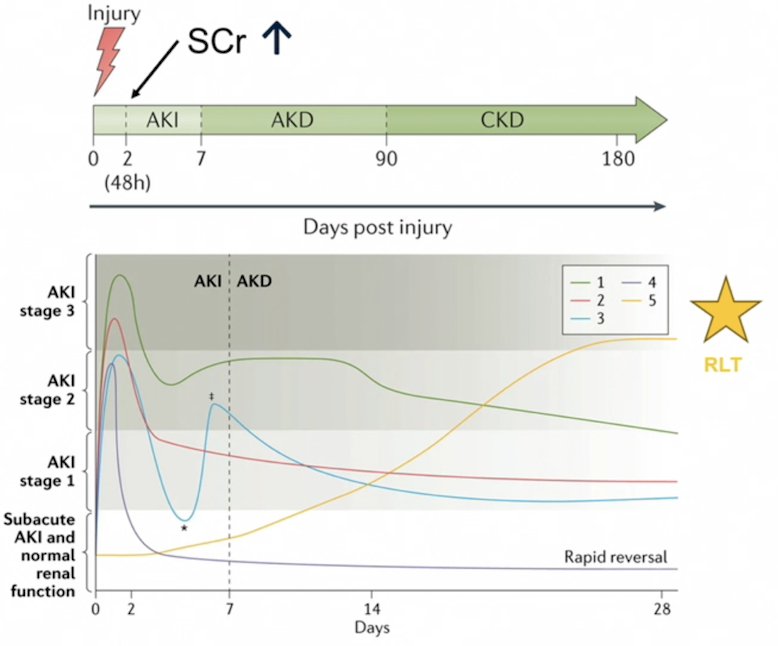
How do the kidneys respond to radiation injury? According to a Consensus report of the Acute Disease Quality Initiative 16 Workgroup,1 ~2 days after a kidney injury, the serum creatinine starts to increase during the acute kidney injury phase, followed by a 7 to 90 day period of acute kidney disease, followed by chronic kidney disease thereafter. The yellow line in the following figure highlights the estimated days post-kidney injury for radioligand therapy:
At the cellular level, after an acute kidney injury, there is cellular differentiation and proliferation that either results in adaptive repair and complete recovery, or maladaptive repair and chronic kidney disease. At the patient level,2 for the first six months there are no symptoms or clinical abnormalities, followed by signs of glomerular pathology (edema, azotemia, proteinuria, hypertension, hypertensive crisis, fatigue, anemia) for 6-18 months, followed by signs of chronic kidney disease (hypertension, albuminuria, anemia, chronic renal failure, small atrophic kidneys) after 18 months from the date of the initial kidney injury. Dr. Azrour states that because, to date, 177Lu-PSMA-617 has only been used in the mCRPC setting (with a median overall survival in VISION3 of 15.3 months), most patients have not typically lived long enough to reach the later stages of chronic kidney disease after 177Lu-PSMA-617:

Thus, it is unknown what the long term kidney toxicity of 177Lu-PSMA-617 will be if it is moved up in the prostate cancer disease space when patients are expected to live longer.
There is some, but limited, data on long term renal toxicity from the VISION trial reported in 2024 [4]. The frequency of renal toxicity was similar between the two treatment arms, and there was a trend for decreasing incidence of renal toxicity by cycle of onset in the 177Lu-PSMA-617 arm:
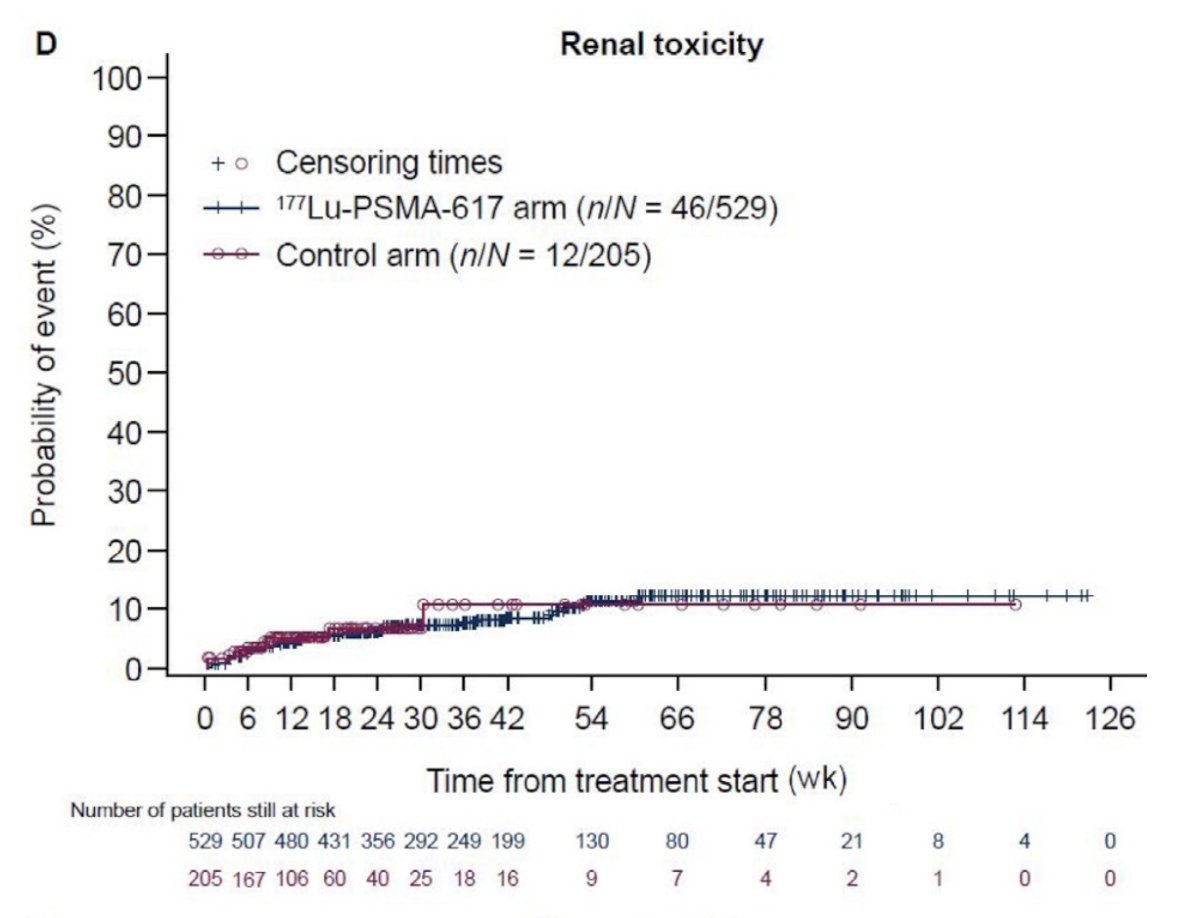
Among patients who started cycle 6, late renal toxicity (onset >6 weeks after the start of the cycle) occurred in 7/257 (2.7%) patients. Five patients had acute kidney injury (grade 3 in 4 patients), one patient had both elevated blood creatinine (grade 2) and proteinuria (grade 1), and one patient had a decrease in urine output (grade 3). Overall, treatment related late renal toxicity was reported for 3/257 patients (1.2%).
Clinically, what occurs after a kidney injury is compensatory hyperfiltration, whereby in the immediate (within 1 year) there is a rise in the eGFR, which has been observed in ~20% of patients undergoing stereotactic body radiotherapy for renal cell carcinoma. In terms of long-term nephrotoxicity, eGFR typically declines 0.15 per month, which translates to -1.8 per year.
Thrombotic microangiopathy (TMA) syndrome is a clinical-pathologic entity characterized by microvascular thrombosis, which can lead to long term kidney injury. Notably, TMA syndromes are a complication of cancer itself and can also occur as a side effect of anticancer agents. Prostate cancer is the 3rd most common cancer with cancer associated TMA syndrome, and cancer patients have a higher risk of developing acute kidney injury at baseline due to tumor burden, comorbidities, nephrotoxic drugs, and hemodynamic instabilities. To date, there have been case reports of 177Lu-PSMA-617 causing TMA syndrome.
Given that serum creatinine and eGFR are not representative of subclinical kidney injury, Dr. Azrour states that there is a need for developing new tools to evaluate early signs of structural kidney injury:
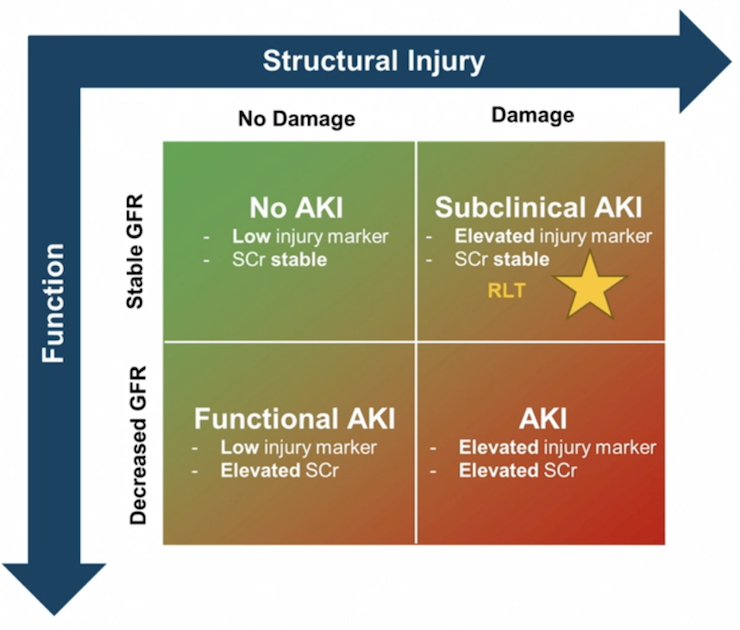
New markers of tubular injury include NGAL and KIM1, and a marker of tubular health and regeneration is EGF.
Dr. Azrour concluded her presentation discussing renal toxicity associated with PSMA targeted therapy with the following take-home points:
- We know that 177Lu-PSMA-617 can injure the kidneys through PSMA expression in the proximal tubules, and Megalin-Cubilin mediate reuptake
- There is a slight long term decline in kidney function after 177Lu-PSMA-617, even after an initial compensatory improvement
- The problem is that it remains difficult to attribute this fully to radioligand therapy because patients have high disease burden and have other risk factors for kidney injury
- The challenge and future work are to use novel tubular biomarkers and patient-specific dosimetry to detect injury earlier and safely expand the use of PSMA radioligand therapy into earlier disease stages
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 PSMA & Beyond Conference, Los Angeles, CA, Thurs, Mar 26 – Fri, Mar 27, 2026.
Related content: Renal Toxicity Associated with PSMA Targeted Therapy "Presentation" - Ines Camille Azrour
References:
- Chawla LS, Bellomo R, Bihorac A, et al. Acute kidney disease and renal recovery: Consensus report of the Acute Disease Quality Initiative 16 Workgroup. Nat Rev Nephrol. 2017 Apr;13(4):241-257.
- Klaus R, Niyazi M, Lange-Sperandio B. Radiation-induced kidney toxicity: molecular and cellular pathogenesis. Radiat Oncol. 2021 Feb 25;16(1):43.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Chi KN, Armstrong AJ, Krause BJ, et al. Safety analyses of the phase 3 VISION trial of [(177)Lu]Lu-PSMA-617 in patients with metastatic castration-resistant prostate cancer. Eur Urol. 2024 Apr;85(4):382-391.