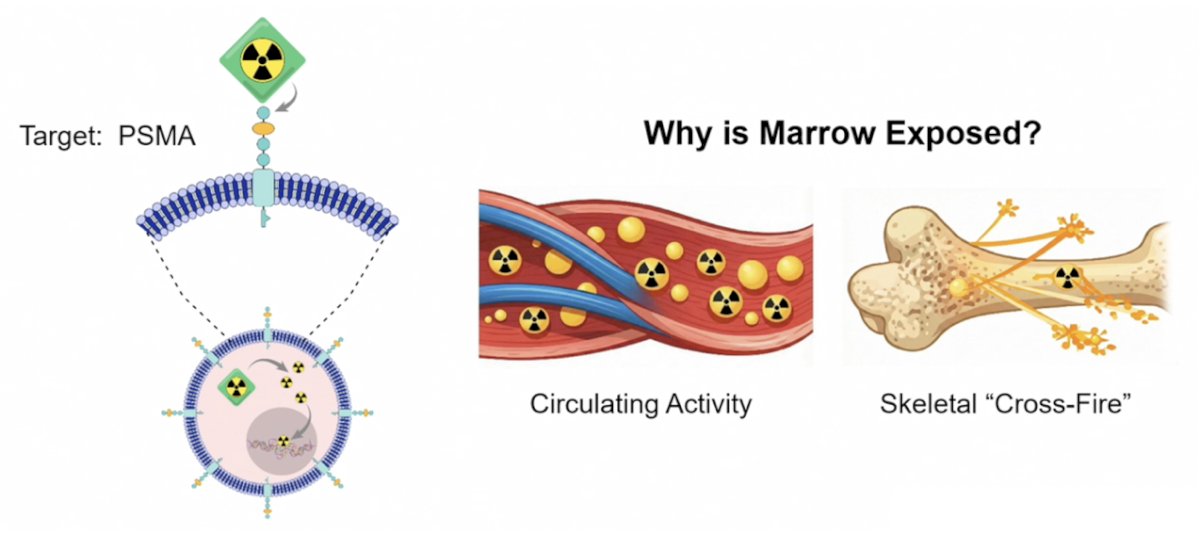
(UroToday.com) The 2026 PSMA & Beyond conference featured a challenges of radioligand therapy session and a presentation by Dr. Daniel Childs discussing long term marrow toxicity rates and risk factors. 177Lu-PSMA-617 is a life prolonging therapy that is increasingly being used in earlier disease settings. As such, understanding and anticipating hematologic consequences will optimize long term outcomes of our patients. Accumulating evidence suggests that radiopharmaceuticals can induce genotoxic stress in the hematopoietic system, resulting in prolonged cytopenias and, in some cases, therapy related myeloid neoplasms:
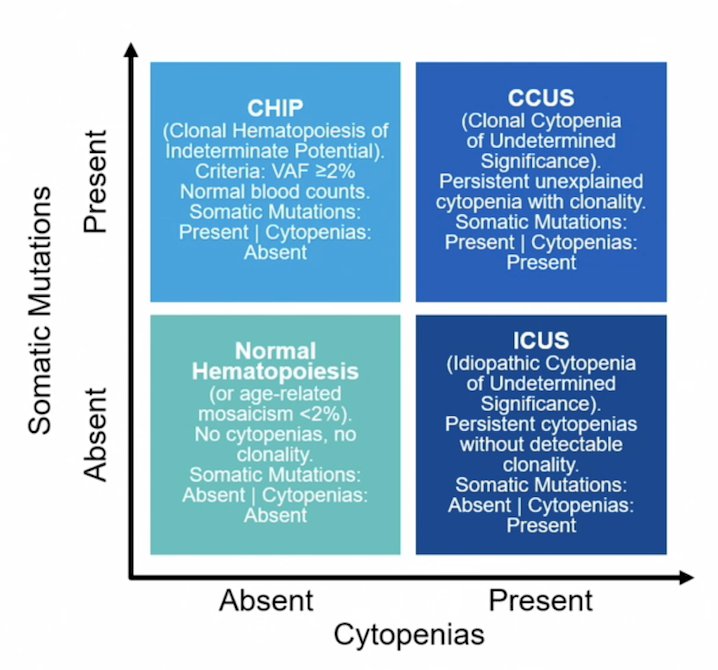
Clonal hematopoiesis refers to the expansion of hematopoietic stem and progenitor cell clones harboring acquired somatic alterations that confer a competitive advantage within the bone marrow. This is commonly seen in aging individuals and further enriched by exposure to genotoxic stressors. Clonal hematopoiesis precursor states provide the biologic substrate upon which additional genomic instability may accumulate, enabling progression to therapy related myeloid neoplasms. The following figure highlights normal hematopoiesis, clonal hematopoiesis of indeterminate potential (CHIP), clonal cytopenia of undetermined significance (CCUS), and idiopathic cytopenia of undetermined significance (ICUS) in the setting of somatic mutations (absent versus present) and cytopenias (absent versus present):
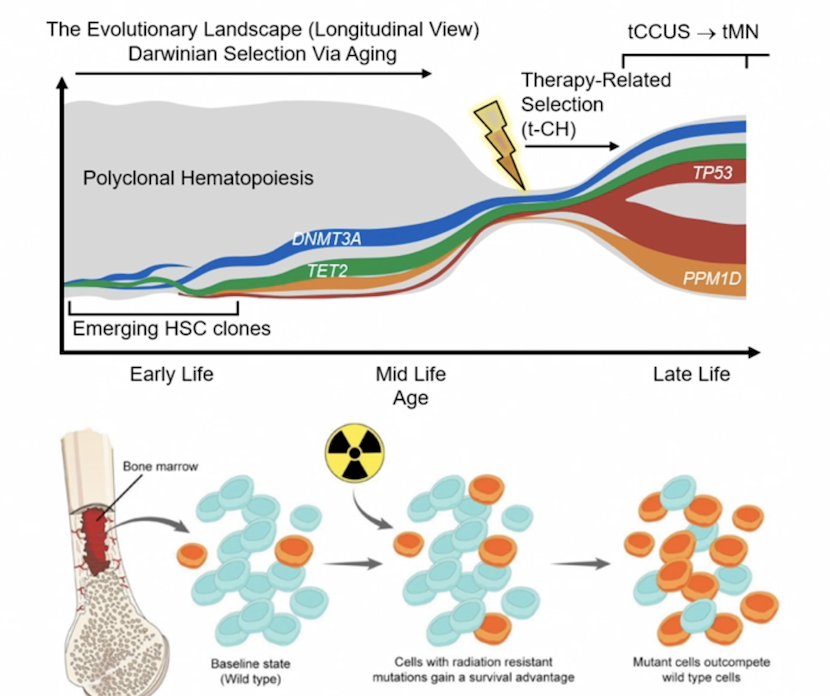
The postulated mechanism is that clonal hematopoiesis increases with age, followed by radioligand therapy exerting selective pressures in the bone marrow, followed by expansion of hematopoietic clones harboring select mutations (DDR genes), followed by radioligand therapy resistant mutations outcompeting WT cells, followed by the development of persistent cytopenias:
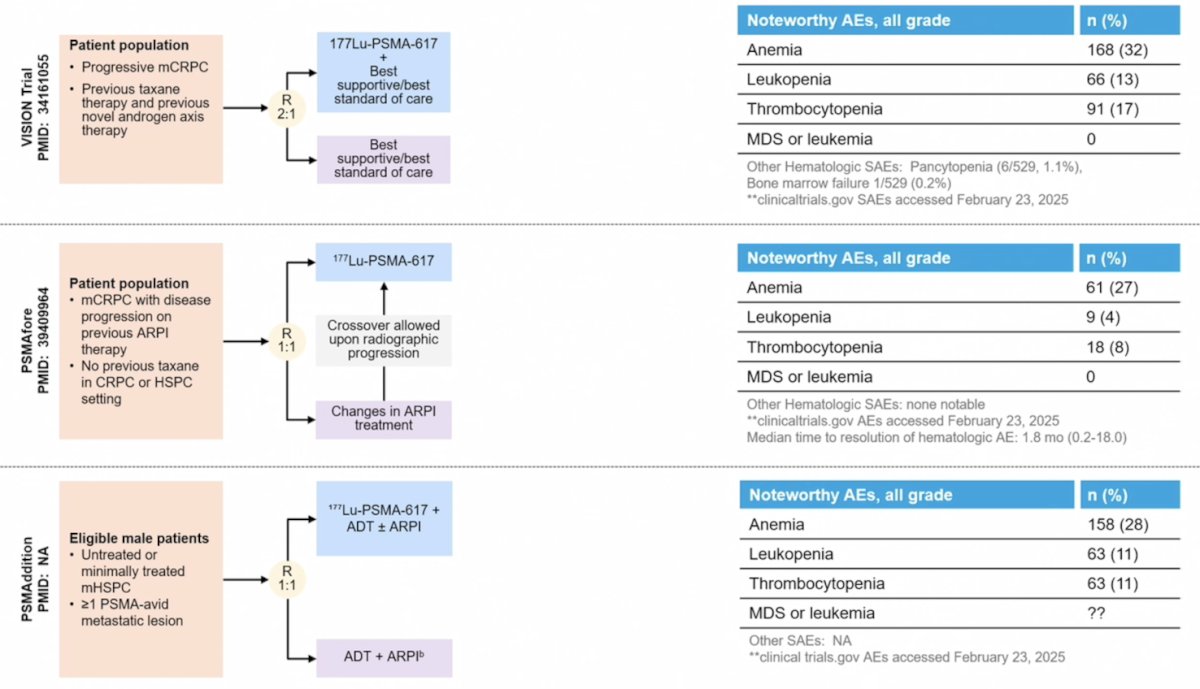
What is the evidence regarding hematologic toxicities associated with 177Lu-PSMA-617 from phase III clinical trials? The following figure highlights the noteworthy adverse events from the VISION,1 PSMAfore,2 and PSMAddition trials. Anemia is the most common hematologic adverse event, ranging from 27%-32%:
What is the evidence regarding hematologic toxicities associated with 177Lu-PSMA-617 from other data sources? Dr. Childs highlighted two large case series from the United States and Australia. In the Mayo Clinic experience,3 from January 1, 2022 to December 31, 2023, 405 patients were treated with 177Lu-PSMA-617, of which 18 patients underwent bone marrow biopsies. The diagnoses included treatment related MDS (n = 9), treatment related CCUS (n = 7), and metastatic carcinoma (n = 2). The median time from cycle 1 of 177Lu-PSMA-617 to bone marrow biopsy was 0.9 years (range: 0.4-4.7). In the Peter MacCallum Cancer Centre experience,4 between August 26, 2015, and December 31, 2022, there were 381 patients treated with 177Lu-PSMA-617, of which 5 patients (1.3%) were subsequently diagnosed with a therapy related myeloid neoplasm (including MDS, APL, and AML). The median time from cycle 1 of 177Lu-PSMA-617 to diagnosis of therapy related myeloid neoplasm was 33.6 months (range: 6.0 – 55.8 months).
Is this the true incidence of therapy related myeloid neoplasm post 177Lu-PSMA-617? There is evidence of persistent hematologic dysfunction after 177Lu-PSMA-617 therapy, even among patients who do not receive additional anti-cancer therapies, with few patients undergoing bone marrow biopsies after 177Lu-PSMA-617.
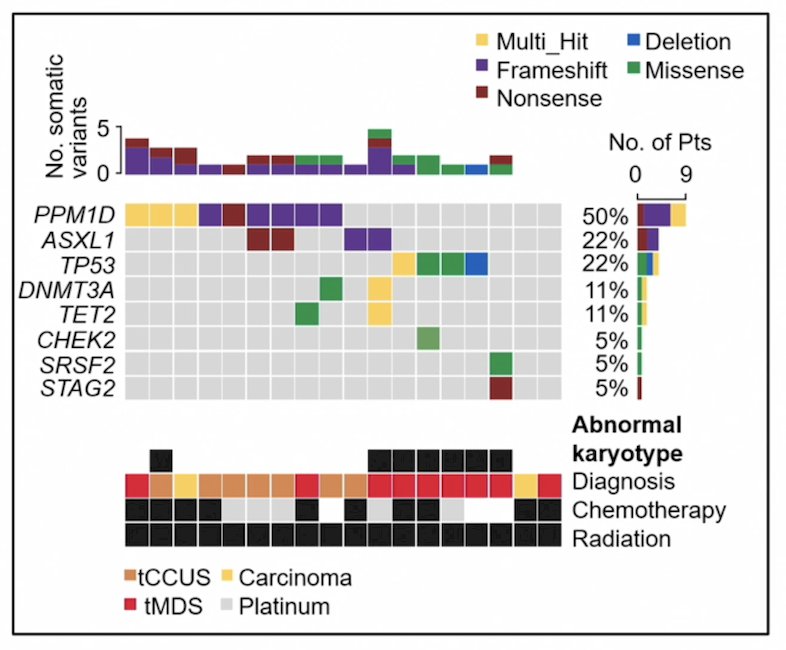
Dr. Childs notes that clonal hematopoiesis involving epigenetic regulators (ie. DNMT3A, TET2, ASXL1) typically expands slowly and remains clinically silent for years. In contrast, clonal hematopoiesis involving the DDR pathway was present in 72% of patients undergoing bone marrow biopsy in the Mayo Clinic dataset, resulting 50.0% of patients with PPM1D, 22.2% with TP53, and a median variant allele frequency of 8.5% (range: 2-82%). TP53 and PPM1D-mutant clones can dominate hematopoiesis after stress and may represent founding events in therapy related myeloid neoplasms:
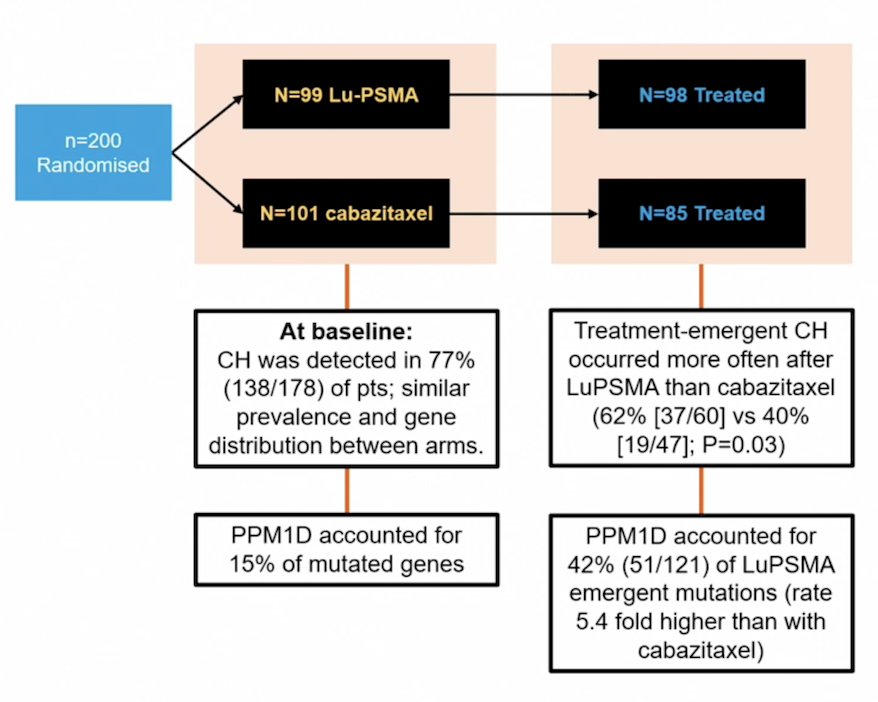
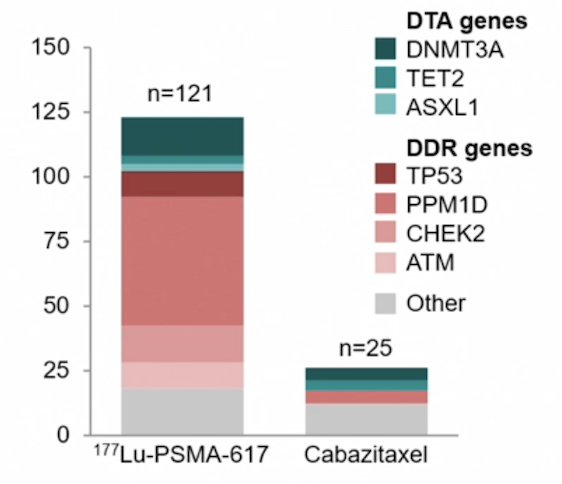
In a post-hoc analysis of the TheraP trial,5 baseline clonal hematopoiesis was detected in 77% of patients, with similar prevalence and gene distribution between arms. Treatment emergent clonal hematopoiesis occurred more often after 177Lu-PSMA-617 than cabazitaxel (62% versus 40%; p = 0.03). The DNA damage response gene PPM1D accounted for 42% of 177Lu-PSMA-617 emergent mutations, with odds ratios of 3.2 for any treatment emergent clonal hematopoiesis and 5.4 for PPM1D, relative to cabazitaxel:
Clonal hematopoiesis clones expanded more frequently and to a greater magnitude with 177Lu-PSMA-617 (70.9% versus 29.5%; p <0.001):
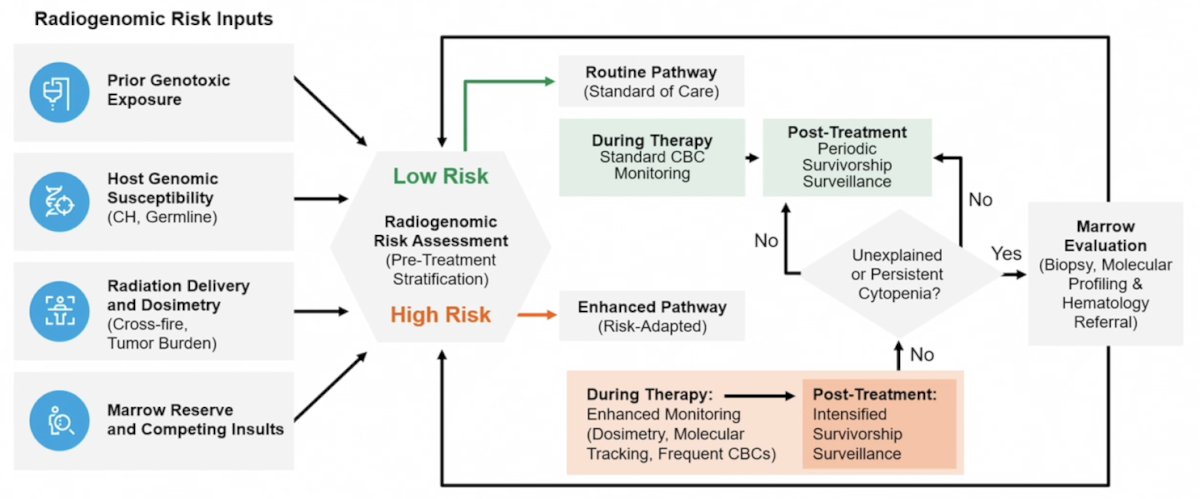
According to Dr. Childs, what is needed is a transition from post-hoc toxicity studies to prospective cohorts. Longitudinal blood collection before radioligand therapy, during therapy, and throughout extended follow-up would define baseline clonal hematopoiesis, track therapy-driven clonal evolution, and identify progression to clonal cytopenias or therapy related myeloid neoplasms. The central question is: can the risk of therapy related myeloid neoplasm following radioligand therapy be mitigated through risk stratification, treatment sequencing, schedule modification, or combination strategies?
Dr. Childs proposes the following radiogenomic risk-adapted framework for radioligand therapy:
Dr. Childs concluded his presentation discussing long term marrow toxicity rates and risk factors with the following take-home points:
- Clinical trials data are unable to provide good estimates of therapy related myeloid neoplasm post 177Lu-PSMA-617
- Persistent hematologic dysfunction and therapy related myeloid neoplasm have been identified in large and rigorous real-world datasets
- This is likely an underestimate of the prevalence of CCUS and therapy related myeloid neoplasm, owing to incomplete evaluation of persistent hematologic dysfunction
- Emerging data suggest that therapy related myeloid neoplasm observed after β-emitting radioligand therapy may occur with shorter latency intervals, measured in months to a few years
- Clonal hematopoiesis does not carry uniform biologic risk
Presented by: Daniel Childs, MD, Mayo Clinic, Rochester, MN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 PSMA & Beyond Conference, Los Angeles, CA, Thurs, Mar 26 – Fri, Mar 27, 2026.
Related content: Monitoring the Marrow: Hematologic Toxicity in the Treatment of Advanced Prostate Cancer "Presentation" - Daniel Childs
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.
- Kusne Y, Mosalem OM, Quillen J, et al. Hematologic dysfunction and myeloid neoplasm risk in patients treated with lutetium-177 prostate-specific antigen membrane therapy. Haematologica. 2025 Sep 1;110(9):2187-2192.
- Eifer M, Sutherland DEK, Goncalves I, et al. Therapy-related myeloid neoplasms after [177Lu]Lu-PSMA therapy in patients with metastatic castration-resistant prostate cancer: A case series. J Nucl Med. 2025 Apr 1;66(4):579-584.
- Munzur AD, Herberts C, Kwan EM, et al. Clonal hematopoiesis after 177Lu-PSMA-617 radioligand therapy in prostate cancer. Clin Cancer Res. 2026 Feb 6 [Epub ahead of print].