(UroToday.com) The 2026 PSMA & Beyond conference featured a clinical development session and presentation by Dr. Michael Morris discussing how PCWG4 impacts future trials. Dr. Morris started his presentation by emphasizing that PCWG4 changes the framework of the disease from an endocrinologic basis to a mechanistic one, which includes no use of the term castration.1 A key milestone is use of prior androgen receptor directed therapy (ADT alone or androgen receptor pathway inhibitor alone or doublet or triplet with another drug class, or novel androgen receptor targeted agent, etc):

Disease states are further defined by additional classifiers, with the following key factors within disease states:
- Genotype (germline, somatic)
- Phenotype: pathology, immunohistochemistry (AR, neuroendocrine prostate cancer, double negative)
- Imaging modality used to define metastasis (PET, CT, MRI, bone scan)
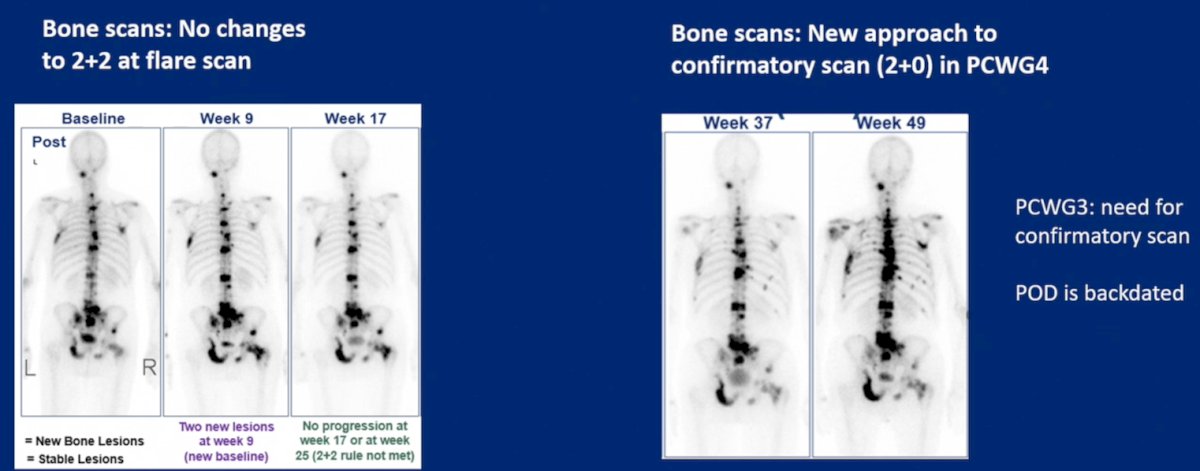
In PCWG3, radiographic progression free survival was qualified as an interim composite endpoint:
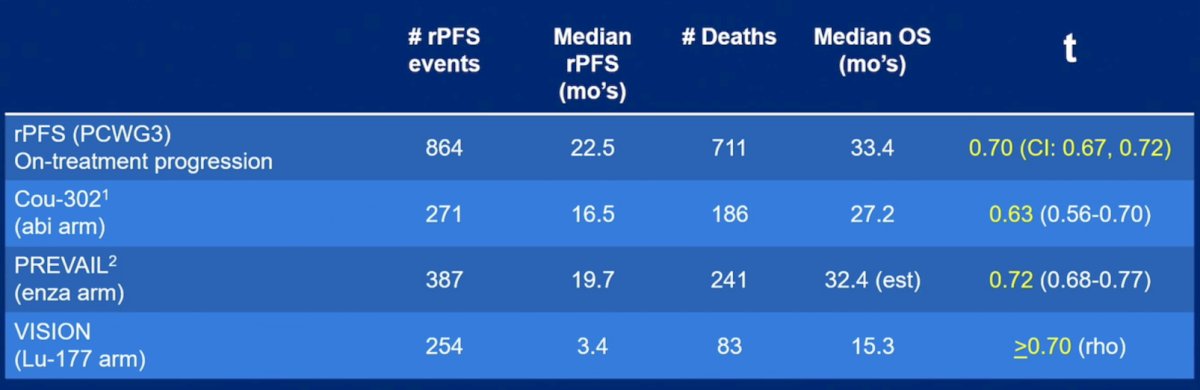
Dr. Morris emphasized that previous studies have shown an association between radiographic progression free survival and overall survival, including in COU-302 [2], PREVAIL [3], and VISION [4]:
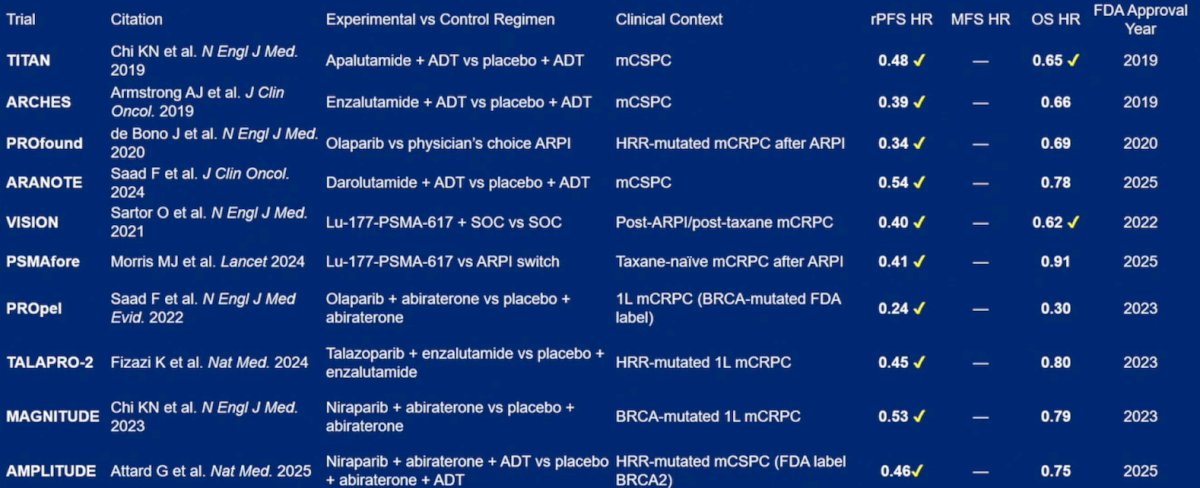
How did PCWG2/3 influence drug development in prostate cancer? The following table shows approved studies and whether there was a radiographic progression free survival and overall survival benefit reported:
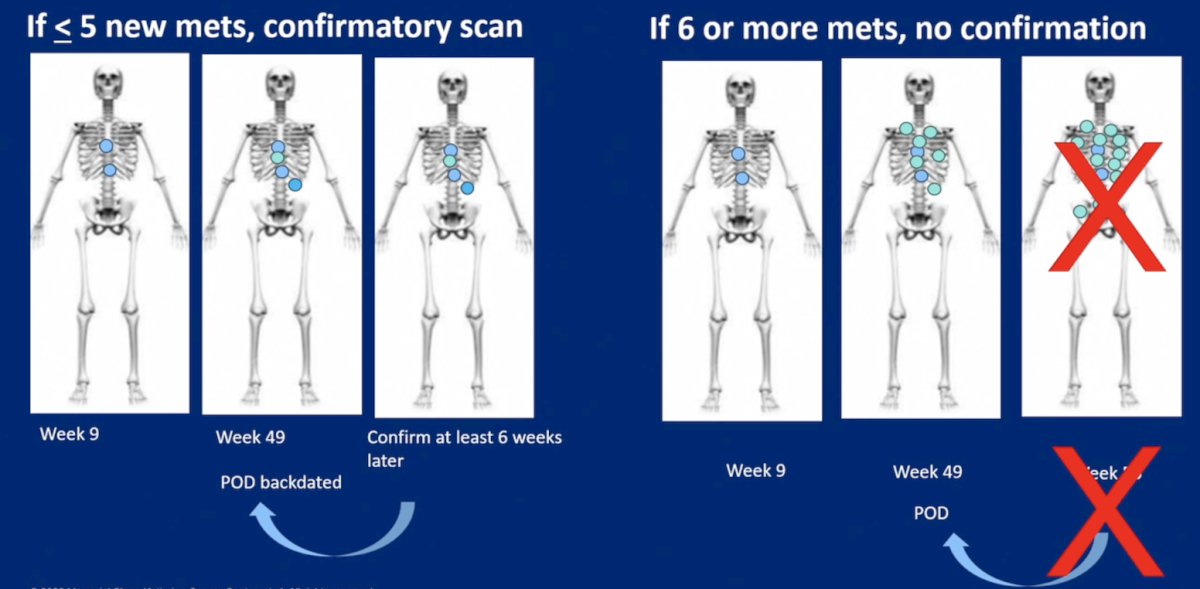
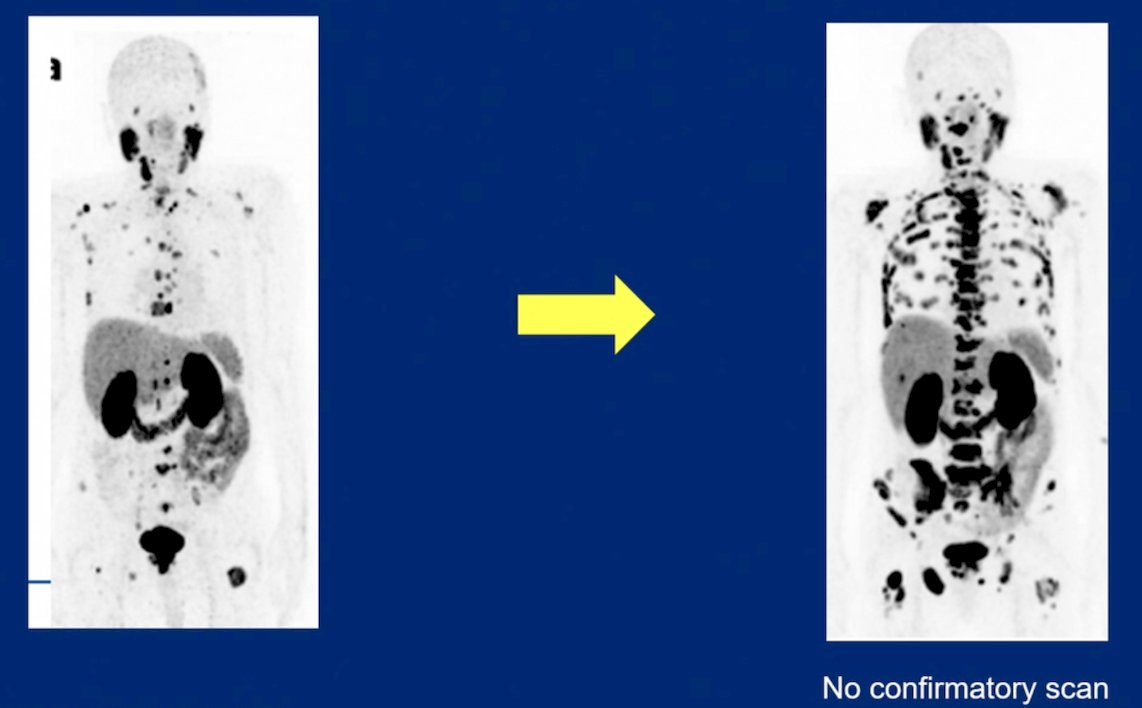
Dr. Morris then discussed the PCWG4 Rule of 5 for defining radiographic progression free survival in the post-flare period. If there are <=5 new metastases, a confirmatory scan is performed, and if there are 6 or more new metastases, no confirmatory scan is performed:
Several PSMA PET guiding principles include:
- Endpoints should be simple
- Endpoints should be feasible to determine on an international basis
- Non-proprietary software should be used to avoid planned obsolescence
- Requires clinical validation
- Progression is a regulatory and radiographic endpoint, and does not imply end of treatment benefit
Importantly, PCWG4 incorporates PSMA PET. Other schemas, such as RECIP and PPP, for response and progression are acknowledged, and serve as an opportunity to build and/or validate these further. Currently, changes in volume or SUVs are investigational, complete response is defined as a resolution below the blood pool, and progression is based on new lesions, taking into account intensity, pattern of spread, and anatomic correlates. Because PCWG4 now incorporates PSMA PET, each modality should be independently reported, and this includes: (i) PSA and serum biomarkers (PCWG3), (ii) bone scintigraphy (radiographic progression free survival per PCWG4), (iii) anatomical imaging (modified RECIST), and (iv) molecular imaging (radiographic progression free survival per PCWG4). Dr. Morris stated again that these should not be grouped together.
With regards to bones, lymph nodes, and pulmonary metastases, these should be treated as a single category, and the Rule of 5 applies:
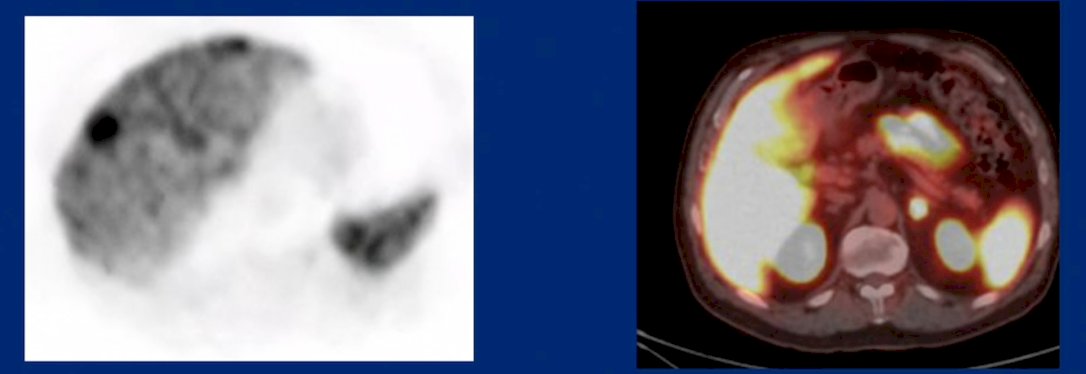
For non-pulmonary visceral metastases, any single lesion on PET constitutes radiographic progression:
For metastasis free survival, PCWG3 deferred to regulatory authorities, and any new lesion had variable requirements for confirmatory studies. PCWG4 will not change any of these definitions. If metastasis is found by PSMA PET alone and not evident by any other imaging modality, this clinical situation should be approached cautiously, especially if earlier in the disease state, given the uncertainty of the clinical relevance.
Dr. Morris concluded his presentation discussing how PCWG4 impacts future trials with the following take-home points:
- There is new nomenclature
- PCWG4 offers a safer definition of radiographic progression free survival without changing the stated time of radiographic progression free survival
- PCWG4 incorporates PSMA PET imaging
- Metastasis free survival should be treated cautiously if only the PSMA PET is positive
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 PSMA & Beyond Conference, Los Angeles, CA, Thurs, Mar 26 – Fri, Mar 27, 2026.
Related content: How PCWG4 Impacts Future Trials "Presentation" - Michael Morris
References:
- Armstrong AJ, Morris MJ, Abida W, et al. Trial design and objectives for patients with prostate cancer: Recommendations from the Prostate Cancer Working Group 4. J Clin Oncol. 2026 Feb 26 [Epub ahead of print].
- Ryan CJ, Smith MR, de Bono JS, et al. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med. 2013;368(2):138-148.
- Beer TM, Armstrong AJ, Rathkopf DE, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med 2014;371(5):424-433.
- Morris MJ, de Bono J, Nagarajah J, et al. Correlation analyses of radiographic progression-free survival with clinical and health-related quality of life outcomes in metastatic castration-resistant prostate cancer: Analysis of the phase 3 VISION trial. Cancer. 2024 Oct 15;130(20):3426-3435.