(UroToday.com) The 2026 PSMA & Beyond conference featured a clinical development session and presentation by Dr. Alicia Morgans discussing the incorporation of PSMA PETs in registrational trials. To do this, Dr. Morgans used the example of the ARASTEP phase 3 clinical trial for biochemical recurrent prostate cancer. Overall, 20-50% of patients with localized prostate cancer treated with curative intent develop biochemical recurrence. PSMA PET/CT has been integrated as a standard method of identifying metastatic lesions in patients with biochemical recurrence, and treatment of visualized lesions on PSMA PET with metastasis directed therapy is associated with prolonged time to progression. Adding darolutamide to ADT has previously been associated with improved cancer control outcomes versus ADT in non metastatic castration resistant prostate cancer (nmCRPC) in the ARAMIS trial1 and metastatic hormone sensitive prostate cancer (mHSPC) in the ARANOTE trial.2 The hypothesis for ARASTEP is that darolutamide + ADT will prolong time to progression versus ADT alone for patients with PSMA PET positive oligorecurrent prostate cancer.
The trial design for ARASTEP is highlighted in the following schema:
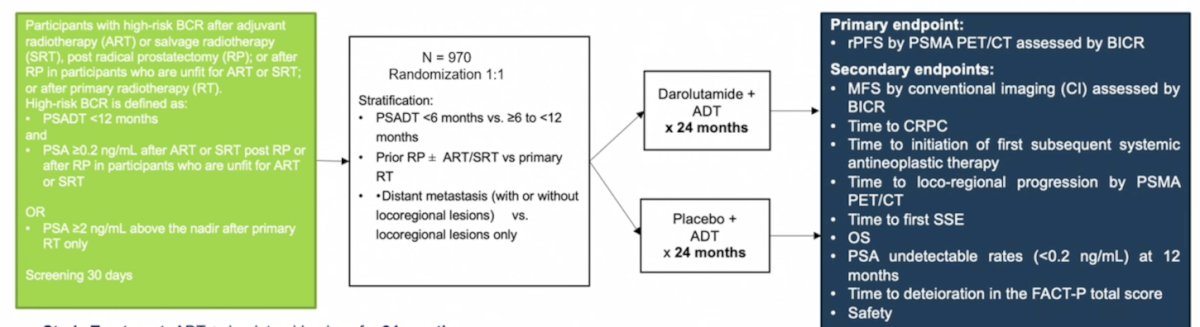
Two special considerations for ARASTEP are that all patients have maximally treated pelvic disease and that metastasis directed therapy (surgery or radiation) should be performed for all PSMA PET identified lesions.
The primary endpoint for ARASTEP is radiographic progression free survival by PSMA PET/CT assessed by blinded independent central review, defined as the time from randomization to first documentation of at least one new distant metastatic lesion by PSMA PET/CT assessed by blinded independent central review or death due to any cause, whichever occurs first. PET/CT scans will be performed at baseline and during the study every 24 weeks until at least one new distant metastatic lesion on PSMA PET/CT is observed or until primary completion, whichever is first. A distant metastatic lesion is one occurring in the bone, viscera or in lymph nodes above the common iliac artery bifurcation/ distal to external iliac artery. A key secondary endpoint is metastasis free survival by conventional imaging assessed by blinded independent central review, defined as the time from randomization to first documentation of at least one new distant metastatic lesion by conventional imaging, assessed by blinded independent central review or death due to any cause, whichever occurs first. Conventional imaging (CT or MRI scans and bone scans) for metastasis free survival will be performed by blinded independent central review and by the site investigators and will utilize RECIST 1.1 tumor response criteria. Conventional imaging will be performed at baseline and during the study every 24 weeks until radiological progression by conventional imaging is confirmed. Additional endpoints include:
- Time to CRPC: PSA and radiographic progression
- Time to initiation of first subsequent therapy: inclusive of metastasis directed therapy and/or systemic therapy
- Time to loco-regional progression by PSMA PET: Pelvic recurrence (excluded from extra-pelvic metastasis directed therapy)
- Overall survival
- Safety and tolerability assessments (patient report outcomes - deterioration, time to symptomatic skeletal event, time to symptomatic progression)
The definition of PSMA PET progression will include a new M1 (extra-pelvic) lesion on PSMA PET. If participants experience progression by conventional imaging, PSMA PET imaging continues every 6 months until at least one new lesion is identified on PSMA PET. If treatment is delivered per local standards, the reason for treatment (PSA progression, local progression, toxicity) must be documented. There is a strong recommendation to avoid treatment based on PSA progression alone without PSMA PET progression.
There are several important considerations for ARASTEP:
- Blinded central scan review with a specific charter for PET imaging
• Locked baseline read (no retrospective change in lesion review based on subsequent imaging findings)
• Scan reviews independent of clinical information - Conventional imaging and PSMA PET imaging occur on the same schedule (every 6 months)
• PSMA PET imaging must continue even if conventional imaging demonstrates metastasis free survival - Additional endpoints (time to next therapy (systemic or metastasis directed therapy), time to CRPC (PSA or radiographic progression), loco-regional progression, and overall survival) are critical
One of the challenges for ARASTEP is that the definition of PSMA PET progression was created prior to the recently established PCWG4. The trial definition was created based on consensus statements and best evidence at the time, and thus, a change of the primary endpoint is not possible. Second, current practices for metastasis directed therapy vary by region and practice patterns, and metastasis directed therapy is common. Follow up imaging after metastasis directed therapy may be difficult to interpret. Third, there are challenges in planning for every pattern of progression and subsequent intervention in an international trial (ie. progression in a previously treated lesion, discordance between local and central interpretation of scans).
An example of a difficult to interpret scan is a “positive” rib lesion on PSMA PET/CT:
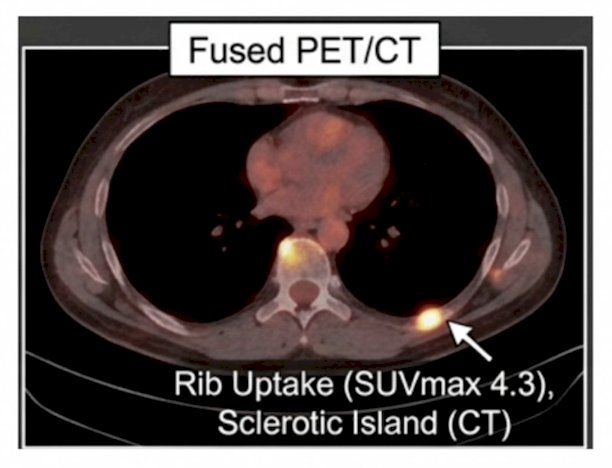
A central read without sclerotic activity on CT and with intermediate SUV uptake is deemed a false positive lesion.
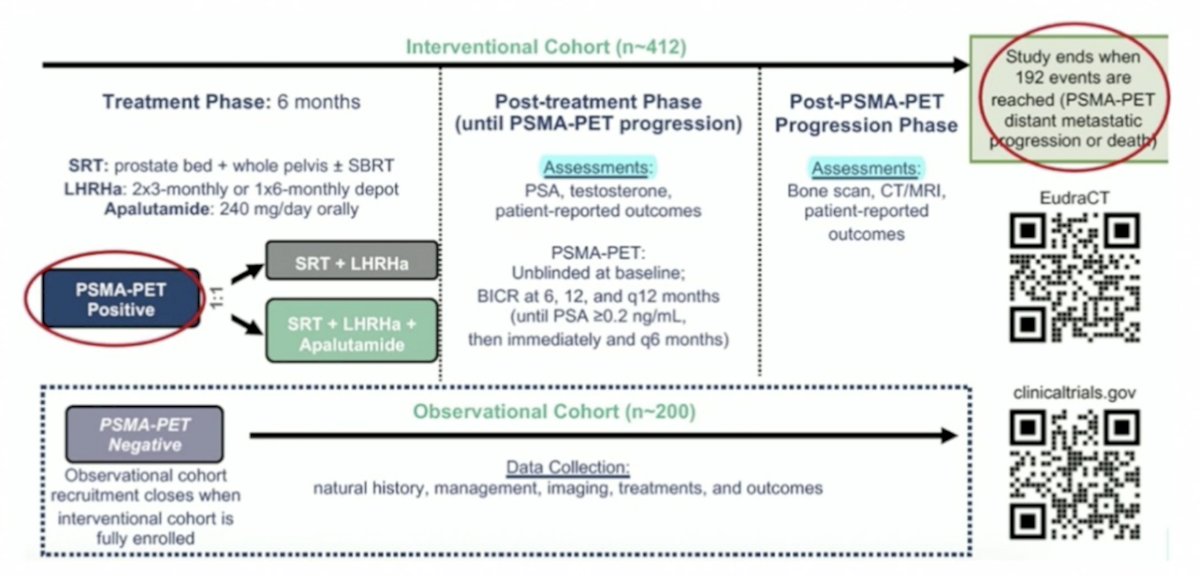
Having a PSMA PET/CT primary endpoint in a clinical trial is also being utilized in other studies, including the PRIMORDIUM trial, which includes standardized PSMA-PET imaging and enrolls PSMA-PET positive patients (≥1 locoregional lesion, interventional cohort) and PSMA-PET negative patients (no lesion, observational cohort). All patients are non metastatic by conventional imaging at screening and have high-risk biochemical recurrence (PSA doubling time ≤12 months or Gleason score ≥8) after radical prostatectomy. PSMA-PET positive patients are randomized 1:1 to either the control arm (whole pelvic salvage radiotherapy + 6 months of LHRH agonist) or the interventional arm (whole pelvic salvage radiotherapy + LHRH agonist + apalutamide 240 mg/day for 180 days). The primary endpoint is PSMA PET metastasis free survival (one new lesion):
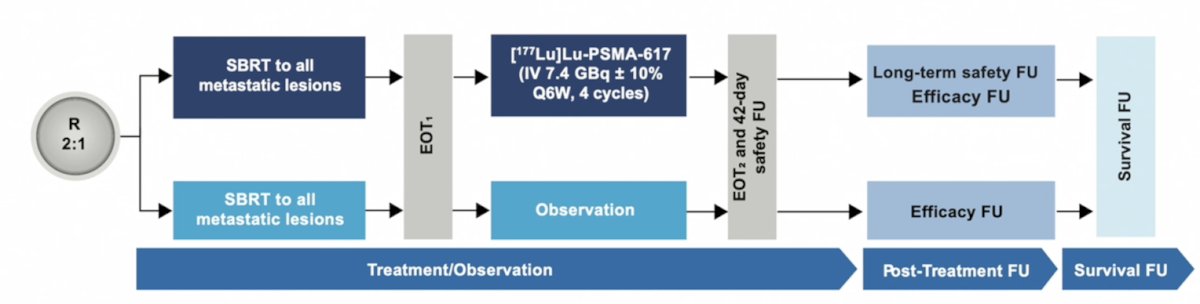
PSMA-DC is an ongoing, international, randomized phase 3 trial to evaluate the efficacy of 177Lu-PSMA-617 versus observation after stereotactic body radiation therapy in delaying castration and disease progression in patients with PSMA PET positive oligometastatic prostate cancer. Patients (n = ~450) will be randomized 2:1 to 177Lu-PSMA-617 or observation and will receive stereotactic body radiation therapy to all metastatic lesions within 14 days, completed within 3 weeks. Patients will then receive either IV 177Lu-PSMA-617 (7.4 GBq/6 weeks; 4 cycles), starting 7–21 days after stereotactic body radiation therapy, or undergo observation only. Additional stereotactic body radiation therapy for new lesions is allowed. ADT is allowed after a metastasis free survival event by conventional imaging confirmed by blinded independent review committee. The primary endpoint is conventional imaging metastasis free survival:
Dr. Morgans concluded her presentation discussing incorporation of PSMA PETs in registrational trials with the following take-home points:
- Strategies to strengthen the validity of a PSMA PET/CT metastasis free survival endpoint can reduce risk:
• Randomization and large sample size balance difficult to interpret cases between groups
• Blinded trial with central imaging review reduces bias
• Rigorous collection of additional endpoints (metastasis free survival by conventional imaging, time to first subsequent therapy (radiation and/or systemic), overall survival) provides supporting evidence of PSMA PET metastasis free survival - PSMA PET is part of the treatment algorithm. Failure to incorporate them risks loss of trial integrity, reduced ability to interpret results, and challenges when integrating results into practice
Presented by: Alicia Morgans, MD, MPH, Dana-Farber Cancer Institute, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 PSMA & Beyond Conference, Los Angeles, CA, Thurs, Mar 26 – Fri, Mar 27, 2026.
Related content: Incorporating PSMA PETs in Registrational Trials "Presentation" - Alicia Morgans
References:
- Fizazi K, Shore N, Tammela TL, et al. Darolutamide in nonmetastatic castration-resistant prostate cancer. N Engl J Med. 2019;380(13):1235-1246.
- Saad F, Vjaters E, Shore N, et al. Darolutamide in Combination with Androgen-Deprivation Therapy in Patients with Metastatic Hormone-Sensitive Prostate Cancer From the Phase III ARANOTE Trial. J Clin Oncol. 2024 Dec 20;42(36):4271-4281.