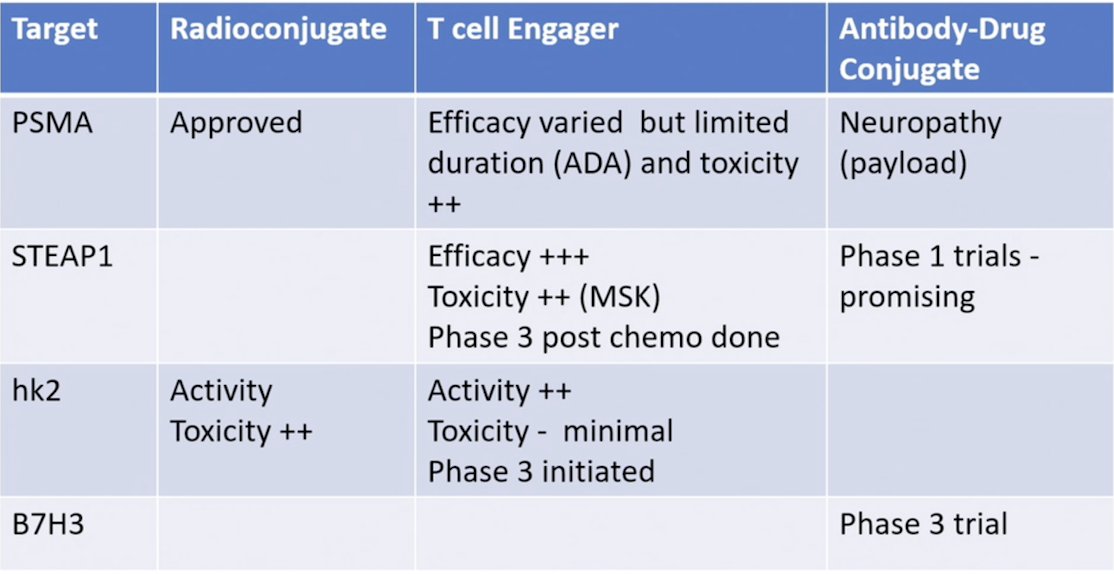
(UroToday.com) The 2026 PSMA & Beyond conference featured a targeting the cell surface session and presentation by Dr. Tanya Dorff discussing antibody drug conjugates and BiTEs and their role in prostate cancer. Dr. Dorff started her presentation by providing the following table showing cell surface targets in prostate cancer.
Early studies used PSMA targeted antibody drug conjugates (MLN2704) with an MMAE payload. In a phase 1 study of 23 mCRPC patients, there were no immunogenicity or dose-dependent pharmacokinetics, and adverse events included diarrhea, nausea, leukopenia, and elevated transaminase.1 There was one dose limiting toxicity (febrile neutropenia), and 2 patients at a high dose had a PSA50 response, with 1 objective response. In another phase 1/2 (n = 62) trial of mCRPC patients, 5 patients (8%) had a PSA decrease, however the disulfide linker lability and rapid deconjugation led to neurotoxicity.2
CD46 is expressed in both adenocarcinoma and neuroendocrine prostate cancer. FOR46 is an antibody drug conjugate to CD46 with an MMAE payload. Initial results were presented at ASCO 2022, whereby 31 patients with mCRPC post androgen receptor pathway inhibitor but chemotherapy naïve and tumor emergent neuroendocrine prostate cancer received FOR46. Among these patients, 10 (32%) had a PSA50 response, and 4/18 (22%) had an objective response rate. In terms of adverse events, grade 3-4 neutropenia occurred in 77% of patients, grade <2 infusion reactions occurred in 37% of patients, grade <2 fatigue in 31%, and grade <2 peripheral neuropathy in 24% of patients. There were 2 partial responders in this cohort.
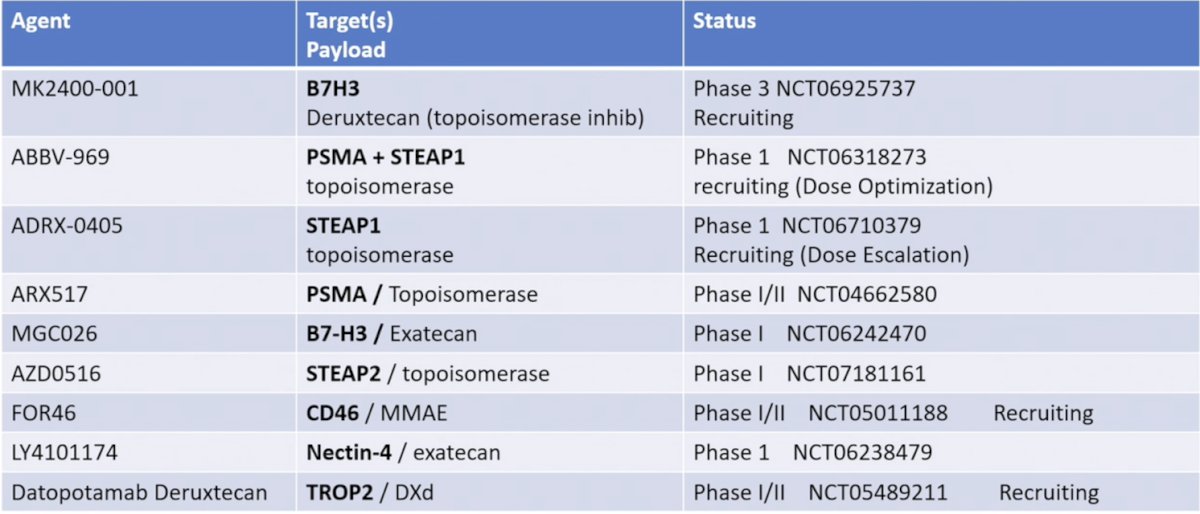
B7H3 is an immune down regulator that is identified in 93-99% of prostate cancers, and expression is associated with more advanced/aggressive disease. DB-1311/BNT324 is an antibody drug conjugate associated with a topoisomerase payload that was tested in 465 patients, including 73 with mCRPC (presented at ASCO 2025). There was an objective response rate of 42.3%, a median progression free survival not reached, and a 6 month radiographic progression free survival rate of 67.7%, with antigen escape clearly not the issue for this antibody drug conjugate. Toxicity included 42.5% grade 3+ adverse events, with an adverse event profile including diarrhea, nausea, and leukopenia. The following table highlights the current antibody drug conjugates in development for prostate cancer (not comprehensive):
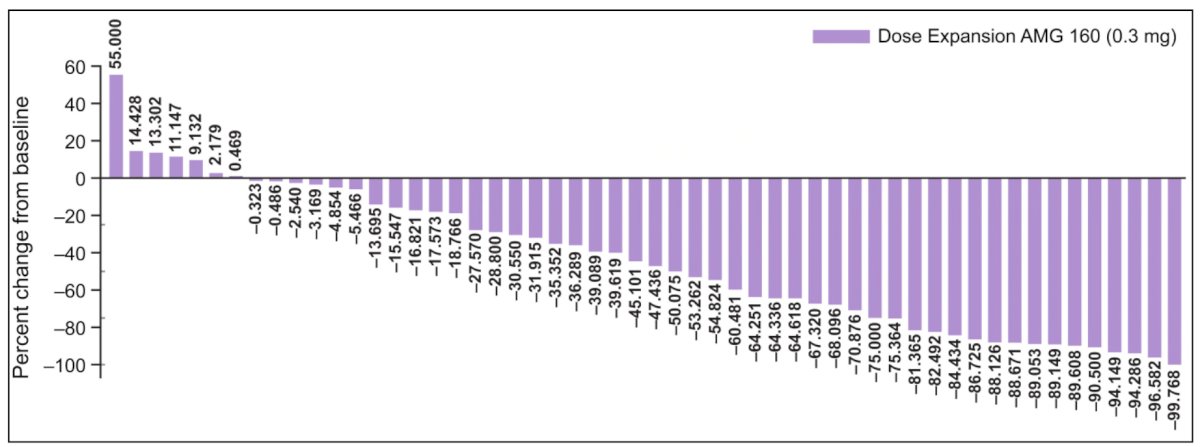
In 2024, Dr. Dorff and colleagues published results of a phase I study of acapatamab, a half-life extended, PSMA-targeting bispecific T-cell engager for mCRPC.3 In the dose expansion phase, 20.3% had grade >= 3 cytokine release syndrome and 27.1% had serious adverse events:

In dose expansion, confirmed PSA50 responses were seen in 30.4% of patients and radiographic partial responses in 7.4% (RECIST 1.1):
Dr. Dorff then discussed JNJ-63898081, a PSMA CD bispecific, which has been previously tested in a phase 1 study.4 All 39 patients experienced ≥1 treatment emergent adverse event, but no treatment related deaths were reported. Cytokine release syndrome was observed at higher doses with JNJ-081 IV or subcutaneous administration, however cytokine release syndrome and infusion-related reaction were reduced with subcutaneous dosing and step-up priming at higher doses. Additionally, treatment doses >30 µg/kg subcutaneous led to transient PSA decreases.
In 2024, Kelly et al.5 reported the first in human study of xaluritamig monotherapy dose exploration for patients with mCRPC, primarily taxane pretreated patients. There were 97 patients who received ≥1 IV dose, ranging from 0.001 to 2.0 mg weekly or every 2 weeks. The maximal tolerated dose was identified as 1.5 mg IV weekly via a 3-step dose. The most common treatment-related adverse events were cytokine release syndrome (72%), fatigue (45%), and myalgia (34%). Cytokine release syndrome occurred primarily during cycle 1 and improved with premedication and step dosing.
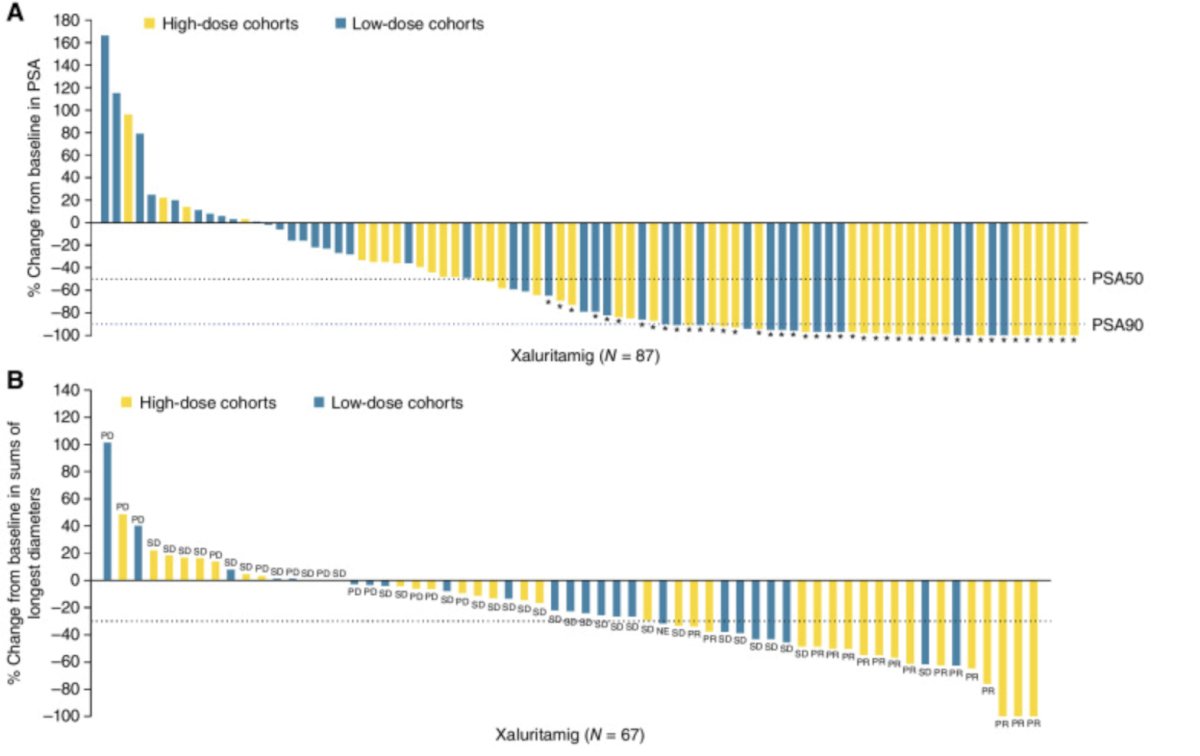
PSA and RECIST responses across cohorts were encouraging, with a 49% PSA50, 24% objective response rate, and with greater frequency at target doses ≥0.75 mg (59% PSA50, 41% objective response rate). The following represents the best PSA percentage change from baseline and the best percentage change in tumor size:
Of note, a phase 3 trial is open (NCT06691984), with a 2:1 randomization to xaluritamig versus physician choice (cabazitaxel or androgen receptor pathway inhibitor).
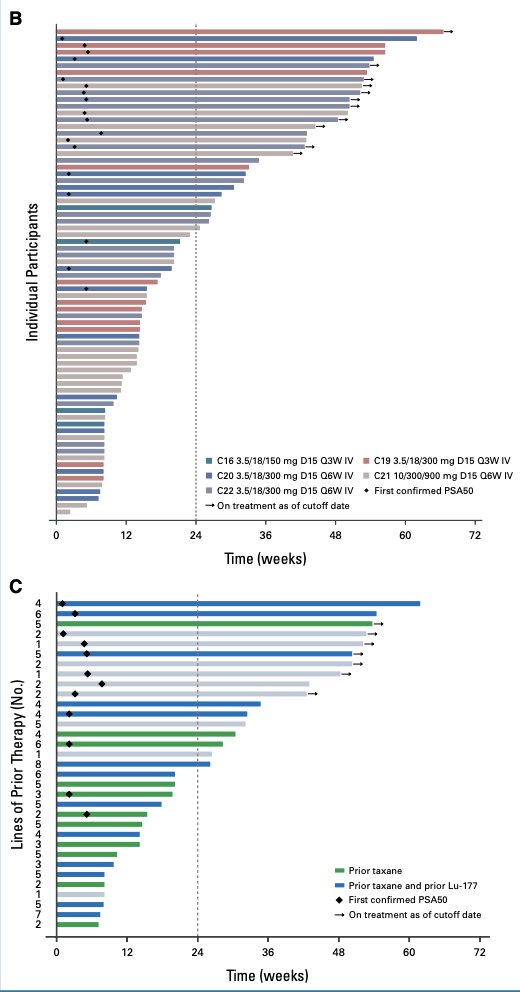
Pasritamig is an hk2 bispecific T cell engager that has been tested in a phase I trial.6 Among 174 patients receiving pasritamig with a median of 4 prior lines of therapy, treatment related adverse events occurred in 82.8% participants, with 9.8% experiencing grade ≥3 treatment related adverse events. In the recommended phase 2 dose safety population (n = 45), infusion-related reactions (24.4%), fatigue (15.6%), cytokine release syndrome (8.9%, all grade 1), and lipase increase (8.9%) were the most frequent treatment related adverse events (all were grade 1 or 2). In the recommended phase 2 dose efficacy population (n = 33), the median radiographic progression free survival was 7.85 (95% CI, 2.89 to not estimable) months, and 14 of 33 (42.4%) participants achieved a ≥50% decrease from baseline in PSA:
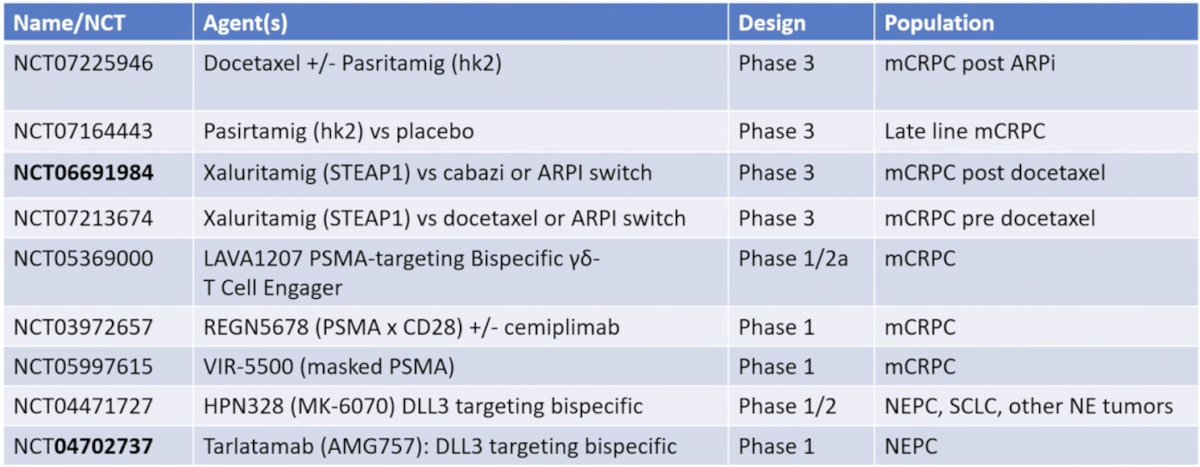
The following table highlights select ongoing trials with bispecific T cell engagers for prostate cancer:
Dr. Dorff notes that for T cell engagers, there is definite evidence of response, and in phase 3 trials, they may beat taxane chemotherapy. PSMA is not the best target, as STEAP1 and hk2 seem to be better, and new constructs may overcome limitations. T cell engagers have a high rate of cytokine release syndrome, making outpatient administration challenging.
Dr. Dorff concluded her presentation discussing antibody drug conjugates and BiTEs and their role in prostate cancer by highlighting that antibody drug conjugates and T cell engagers are active approaches:
- Target:
- Construct:
- Antibody, linker, and chemistry matter
- The ratio of cytotoxic payload or CD3:antigen may be important
- Modality: cytotoxic versus immunotherapy
- It is unclear if one offers superior durability
- CAR T is still the leading candidate for durable response
- The next frontier is how to sequence or combine with radio-conjugates
Presented by: Tanya B. Dorff, MD, City of Hope, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 PSMA & Beyond Conference, Los Angeles, CA, Thurs, Mar 26 – Fri, Mar 27, 2026.
Related content: PSMA and Other Targets in Antibody-Drug Conjugates & Bispecific T-cell Engages "Presentation" - Tanya Dorff
References:
- Galsky MD, Eisenberger M, Moore-Cooper S, et al. Phase I trial of the prostate-specific membrane antigen-directed immunoconjugate MLN2704 in patients with progressive metastatic castration-resistant prostate cancer. J Clin Oncol. 2008 May 1;26(13):2147-2154.
- Milowsky MI, Galsky MD, Morris MJ, et al. Phase 1/2 multiple ascending dose trial of the prostate-specific membrane antigen-targeted antibody drug conjugate MLN2704 in metastatic castration-resistant prostate cancer. Urol Oncol. 2016 Dec;34(12):530.e15-530.e21.
- Dorff T, Horvath LG, Autio K, et al. A phase 1 study of acapatamab, a half-life extended, PSMA-targeting bispecific T-cell engager for metastatic castration-resistant prostate cancer. Clin Cancer Res. 2024 Apr 15;30(8):1488-1500.
- Lim EA, Schweizer MT, Chi KN, et al. Phase 1 study of safety and preliminary clinical activity of JNJ-63898081, a PSMA and CD3 bispecific antibody, for metastatic castration-resistant prostate cancer. Clin Genitourin Cancer. 2023 Jun;21(3):366-375.
- Kelly WK, Danila DC, Lin CC, et al. Xaluritamig, a STEAP1 x CD3 XmAb 2+1 Immune Therapy for Metastatic Castration-Resistant Prostate Cancer: Results from Dose Exploration in a First-in-Human Study. Cancer Discov. 2024 Jan 12;14(1):76-89.
- Stein MN, Vinceneaux A, Robbrecht D, et al. Pasritamig, a first-in-class, bispecific T-cell engager targeting human kallikrein 2, in metastatic castration-resistant prostate cancer: A phase I study. J Clin Oncol. 2025 Aug;43(22):2515-2526.