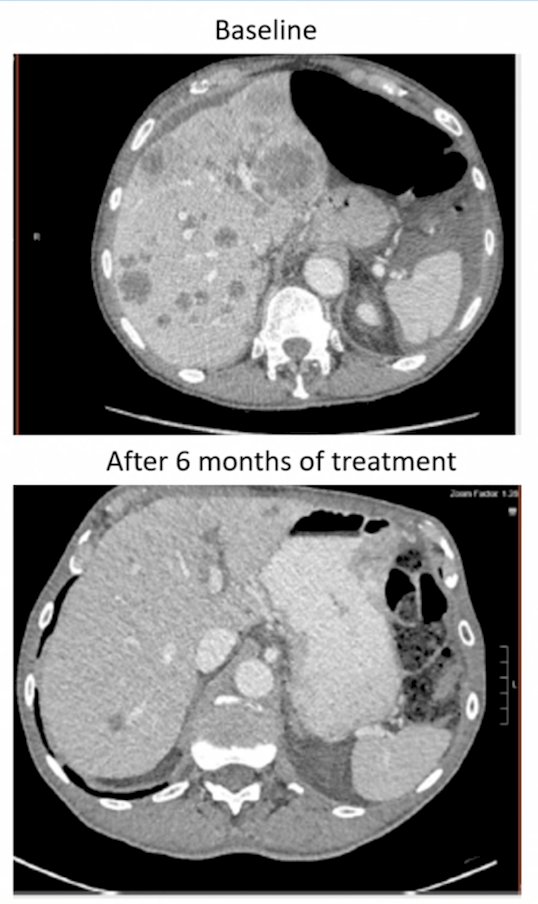
(UroToday.com) The 2026 PSMA & Beyond conference featured a targeting the cell surface session and presentation by Dr. Rahul Aggarwal discussing DLL3 and whether target expression determines the method of targeting. Dr. Aggarwal started his presentation by highlighting a case of a 61 year old male who presented with de novo metastatic disease to the bone and lymph node. A biopsy showed Gleason 4+4 adenocarcinoma of the prostate, with NGS testing showing TMPRSS2-ERG, PTEN deletion, MSS, and low tumor mutational burden. The patient was started on ADT + abiraterone + prednisone, and his PSA went from 40 ng/mL to 0.6 ng/mL at 6 months. A surveillance CT of the abdomen and pelvis at that time showed the following:
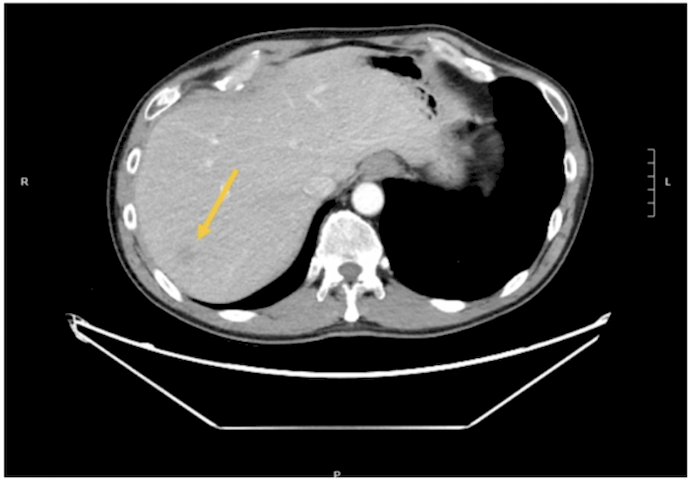
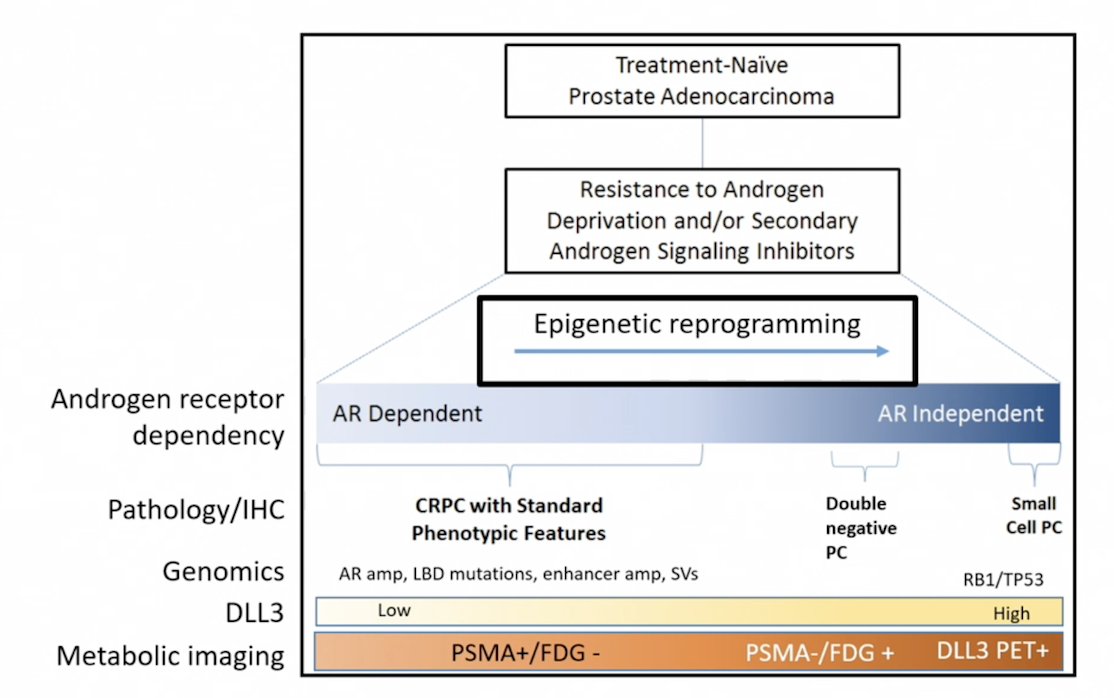
A liver biopsy demonstrated high grade carcinoma with neuroendocrine differentiation with 70% Ki67, NKX 3.1/AR negative, + INSM1, + synaptophysin, and MMR intact. Next generation sequencing showed: RB1 deletion, TP53 point mutation, PD-L1 0%, and DLL3 80% tumor positivity by immunohistochemistry. The patient then received carboplatin + etoposide x 6 cycles, with a partial response lasting for 3 months, at which time he had multifocal progression. Dr. Aggarwal highlighted that lineage plasticity leads to a spectrum of androgen receptor independent prostate cancer:
De novo small cell neuroendocrine prostate cancer is rare (< 1% of new prostate cancer diagnoses) and can be pure or mixed with adenocarcinoma. Treatment emergent neuroendocrine prostate cancer is more common, and incidence and prevalence estimates vary by study. In an evaluation of 202 patients with accessible mCRPC lesions for tumor biopsy and centralized pathology review, 75% had prior androgen receptor pathway inhibition, with pure or mixed small cell histology observed in 17% of all patients.1
DLL3 is an atypical Notch pathway ligand that is overexpressed on the cell surface of small cell lung cancer and other tumor types of neuroendocrine origin. Approximately 60%-80% of neuroendocrine prostate cancer samples are positive for DLL3 expression. There are several ways to target DLL3 in neuroendocrine prostate cancer:
Antibody drug conjugates:
- Typically requires high surface receptor density (> 10,000 copies/cell)
- Receptor mediated endocytosis
- Payloads with varying degrees of bystander effect
- Internalization is not required
- Immunologic synapse
- May be effective even in lower expression/heterogeneous antigens (ie. DLL3)
- cross fire effect and enhanced binding/tumor internalization properties may lead to efficacy with lower density/heterogeneous targets such as DLL3
With regards to antibody drug conjugates, rovalpituzumab tesirine has cathepsin mediated cleavage, with a PBD payload causing DNA damage. There is significant toxicity, including pleural/pericardial effusions, pneumonitis, and transaminitis. Of note, development was halted after a phase 3 small cell lung cancer trial was stopped early for futility.
There is a need for emerging strategies to expand the therapeutic index of drug conjugates targeting DLL3. Payloads with a higher bystander effect and improved predictable toxicity profile include ZL-1310 and FZ-AD005 in early phase clinical trial development. Improving constructs have linker hydrophilicity, dual cleavage, optimizing drug-antibody ratio, site specific conjugation, higher binding affinity, and more efficient internalization. For bi-specific drug conjugates, 1+1 may be greater than 2 for receptor-mediated endocytosis, with improved specificity. Moreover, small molecules and small peptide conjugates may lead to shorter systemic circulation.
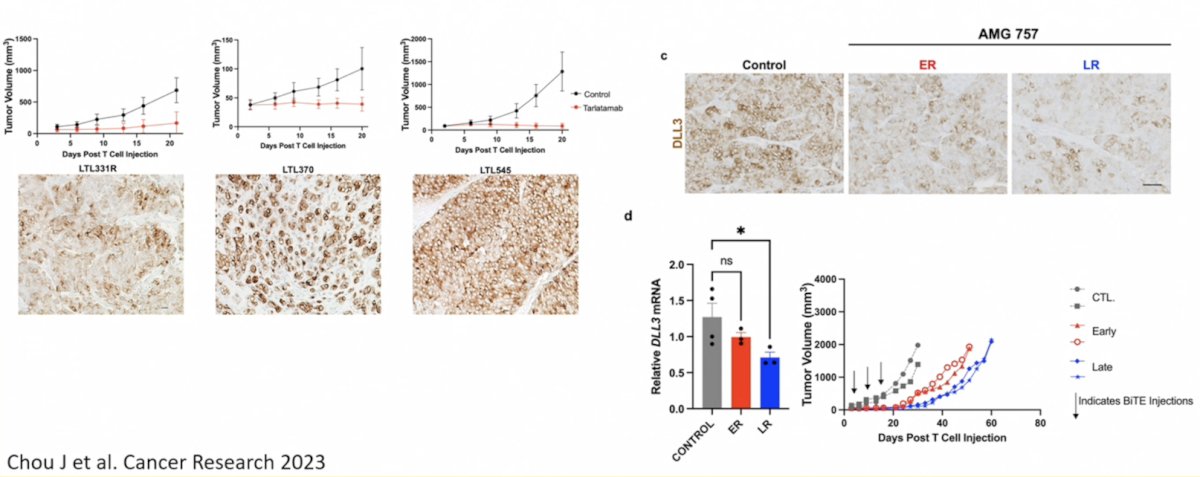
With regards to T-cell engagers, DLL3 expression may drive benefit with T cell engagers, and loss of expression is associated with disease relapse:
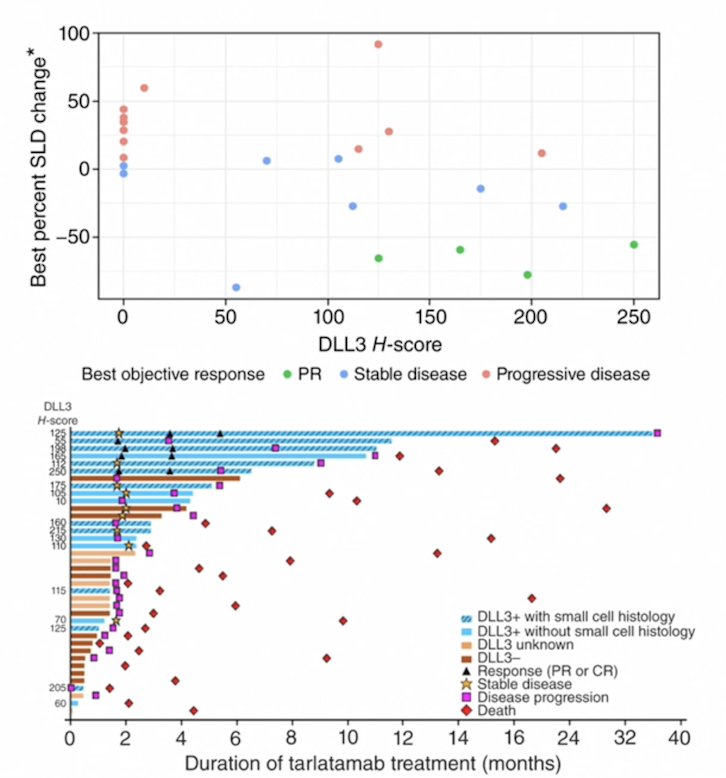
Tarlatamab has been assessed in a phase 1b study in neuroendocrine prostate cancer/molecularly-defined advanced variant prostate cancer led by Dr. Aggarwal and colleagues.2 Of note, change in tumor size from baseline correlated with baseline DLL3 H-score, and objective response rate was 22% in DLL3 positive tumors. Durable responses were observed in a subset of DLL3 positive tumors with small cell histology:
Going back to the clinical case, the patient had DLL3 testing by immunohistochemistry of a liver biopsy, demonstrating strong positive expression (tumor positivity of 80%):
The patient was subsequently enrolled in a tarlatamab phase 2 trial, during which he had grade 1 cytokine release syndrome during cycle 1, and no tocilizumab was required. The patient had a durable response lasting 14 months, but subsequently had disease progression, and he transitioned to second line chemotherapy.
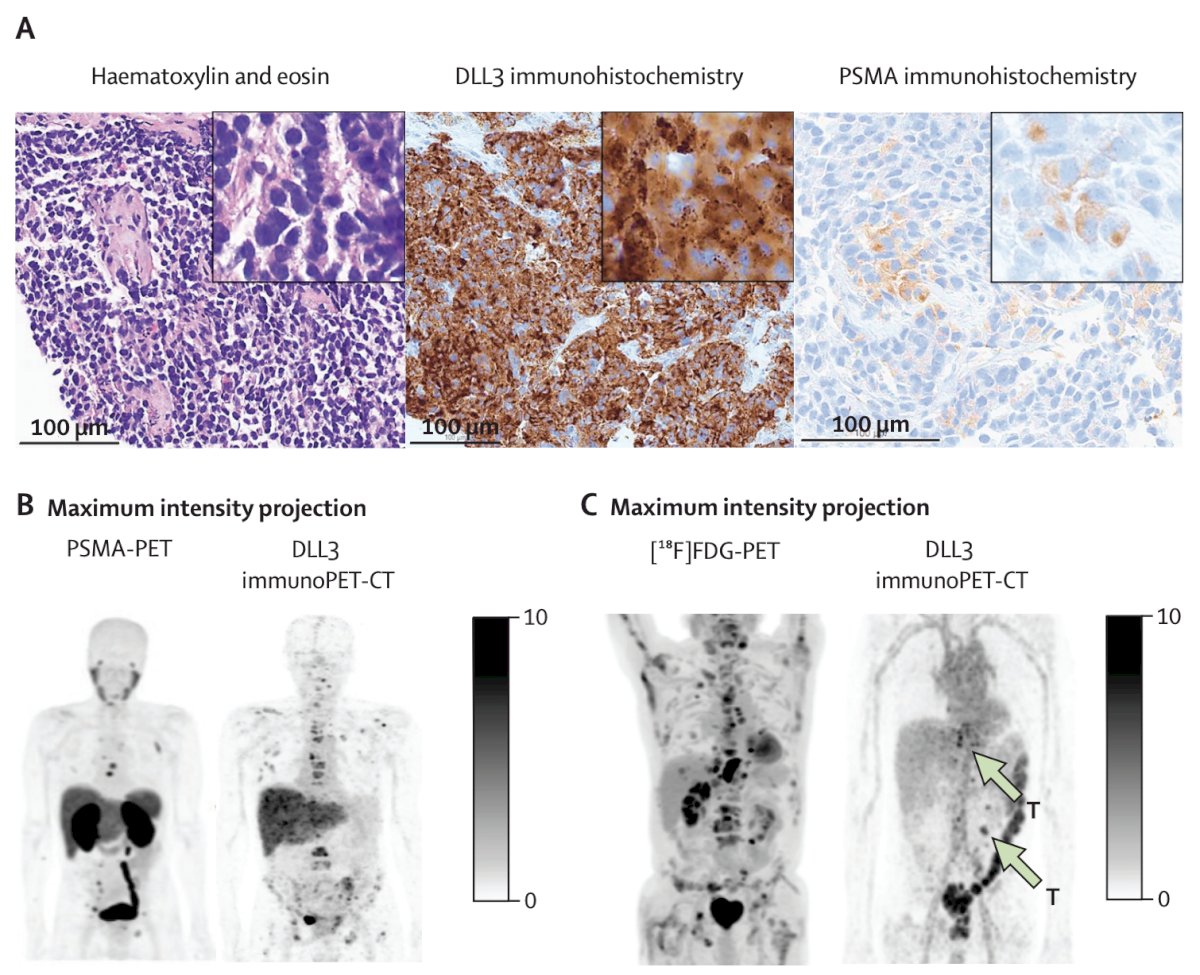
Finally, with regards to DLL3-targeted imaging and radioligand therapy, Tendler and colleagues3 assessed the safety and feasibility of the DLL3-targeted imaging tracer 89Zr-DFO-SC16.56 in patients with neuroendocrine derived cancer. In a patient with transformed neuroendocrine prostate cancer initially diagnosed with prostate adenocarcinoma via biopsy, the patient had rapid progression of liver metastases, which were PSMA-PET tracer non avid, with corresponding low PSMAP protein expression on immunohistochemistry of the liver metastases sampled on repeat biopsy. Furthermore, the liver biopsy sample showed high grade neuroendocrine carcinoma, with high DLL3 protein expression. Additionally, the DLL3 immunoPET-CT showed that most metastases were DLL3-avid:
Emerging therapeutics for DLL3-targeted radioligand therapy include next generation 177Lu-based radioligand therapy, with a fully human Fab-arm exchange-deficient IgG4 backbone. A second therapeutic Pb-212 radio-DARPins, has a short systemic half-life, high binding affinity, and thermal stability. Finally, 225Ac-ETN0239 is a macrocyclic peptide with a phase I trial ongoing.
Dr. Aggarwal concluded his presentation discussing DLL3 and whether target expression determines the method of targeting by highlighting future direction with DLL3-targeting in neuroendocrine prostate cancer:
- Combination therapies targeting different cell surface antigens
- Combining with other cell surface antigens expressed in neuroendocrine prostate cancer (SEZ6, CEACAM5, GPC3, and others)
- Combining payloads (ie. radioligand therapy + T cell engager)
- Mechanisms of DLL3 cell surface expression and enhancing expression to achieve more robust responses
- Optimizing patient selection and moving beyond neuroendocrine diagnostic classification to focus on target expression: ie. the phase 2 TIDAL trial of DLL3 positive metastatic prostate cancer (MSKCC/UCSF)
Presented by: Rahul Aggarwal, MD, UCSF, San Francisco, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 PSMA & Beyond Conference, Los Angeles, CA, Thurs, Mar 26 – Fri, Mar 27, 2026.
Related content: DLL3: Does Target Expression Determine the Method of Targeting? "Presentation" - Rahul Aggarwal
References:
- Aggarwal R, Huang J, Alumkal JJ, et al. Clinical and genomic characterization of treatment-emergent small-cell neuroendocrine prostate cancer: A multi-institutional prospective study. J Clin Oncol. 2018;36(24):2492-2503.
- Aggarwal R, Rottey S, Bernard-Tessier A, et al. Safety and efficacy of tarlatamab in patients with neuroendocrine prostate cancer: Results form the phase 1b DeLLpro-300 study. Clin Cancer Res. 2025 Sep 15;31(18):3854-3863.
- Tendler S, Dunphy MP, Agee M, et al. Imaging with [89Zr]Zr-DFO-SC16.56 anti-DLL3 antibody in patients with high-grade neuroendocrine tumours of the lung and prostate: A phase 1/2, first-in-human trial. Lancet Oncol. 2024 Aug;25(8):1015-1024.