(UroToday.com) The 2026 PSMA & Beyond conference featured an approaches to combination therapies session and presentation by Dr. Shahneen Sandhu discussing lessons learned from radioligand combination therapies. Despite many patients having an adequate/excellent response to 177Lu-PSMA-617 in TheraP1 and VISION,2 there are still patients experiencing primary and secondary resistance:
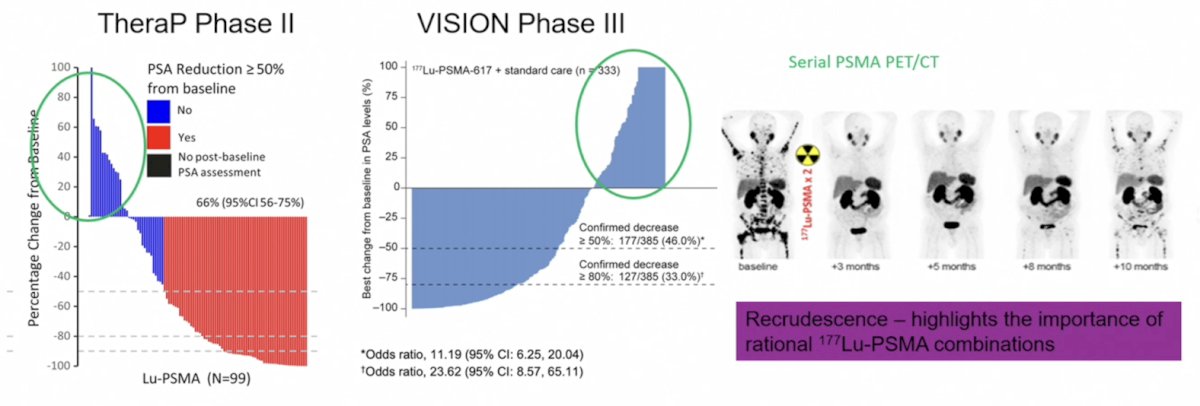
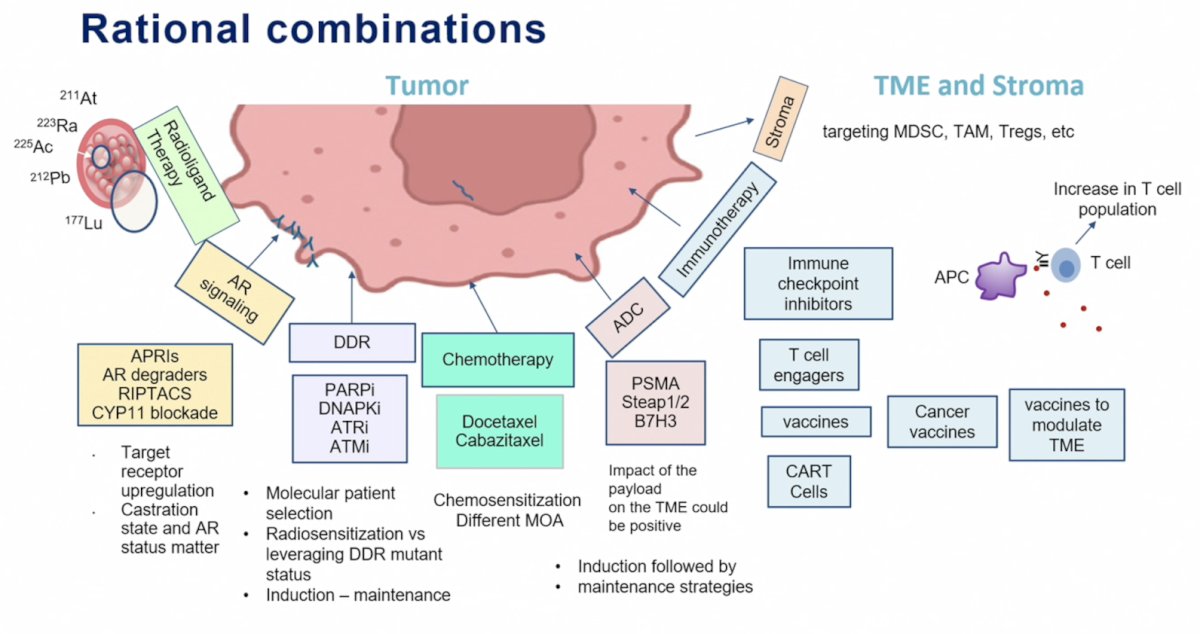
Dr. Sandhu notes that an inherent radioresistant biology and tumor volume/heterogeneous targets are part of the biology that drives primary resistance. Can we turn this around with alpha emitters and combinations of radioligand therapy? Is it possible to reduce the subset of rational combination treatments?
- Androgen receptor pathway inhibitor + radioligand therapy
- Chemotherapy + radioligand therapy
- T cell engagers + radioligand therapy
- Antibody drug conjugates + radioligand therapy
- DDR inhibitors + radioligand therapy
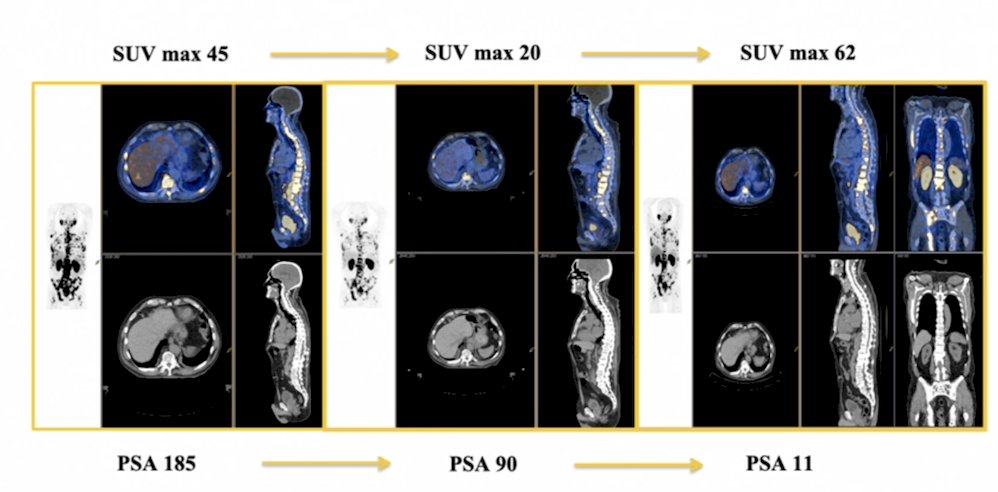
First, Dr. Sandhu discussed leveraging androgen receptor signaling. Previous studies have suggested that androgen receptor pathway inhibitors can upregulate PSMA expression, with a median 45% increase in SUVmax by day 9:
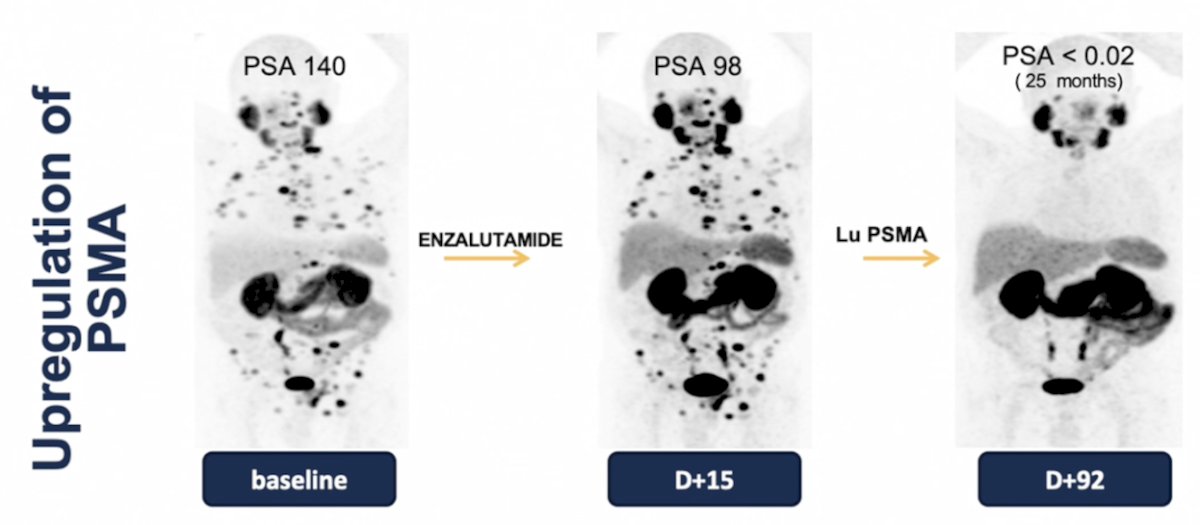
The following case example demonstrates upregulation of PSMA, with images at baseline, after enzalutamide, and after 177Lu-PSMA-617:
Dr. Sandhu then discussed the PSMAddition trial, which randomized men with untreated or minimally treated mHSPC and ≥1 PSMA-positive metastatic lesion on 68Ga-PSMA-11 PET/CT to the experimental arm of 177Lu-PSMA 617 (7.4 GBq ±10% 6 cycles every 6 weeks) + ADT + androgen receptor pathway inhibitor versus the control arm of ADT + androgen receptor pathway inhibitor. Of note, crossover to the 177Lu-PSMA 617 arm was permitted upon radiographic progression:
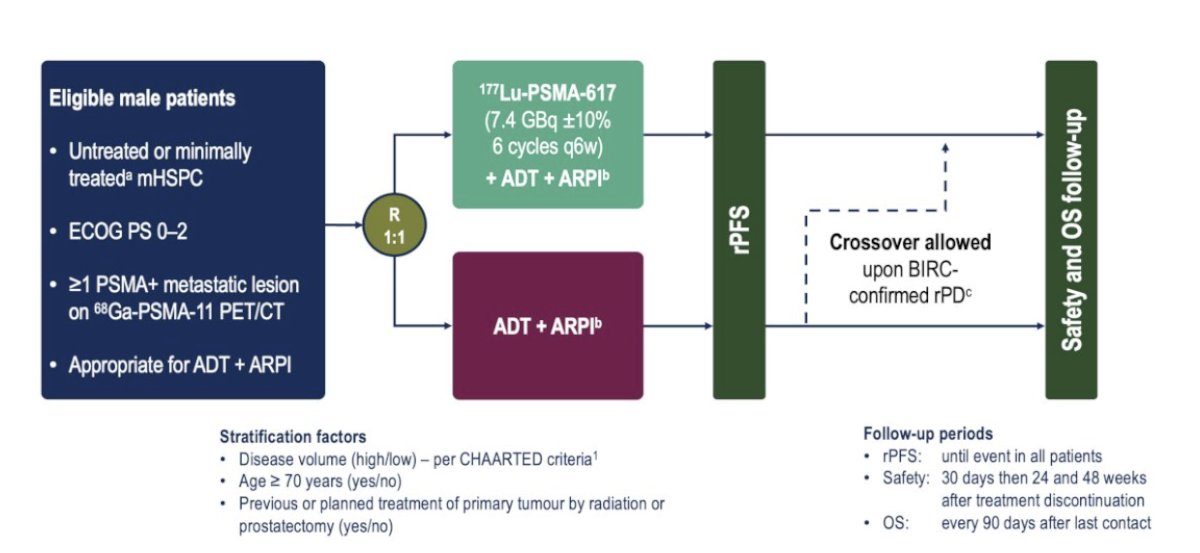
The primary study endpoint was radiographic progression free survival, assessed via blinded central review using the PCWG3/RECIST v1.1 criteria. The key secondary endpoint was overall survival, with other endpoints including:
- PSA90 response rate
- Time to castration resistance
- Progression free survival and progression free survival 2
- PSA <0.2 ng/ml at 12, 24, and 38 weeks
- Safety and tolerability
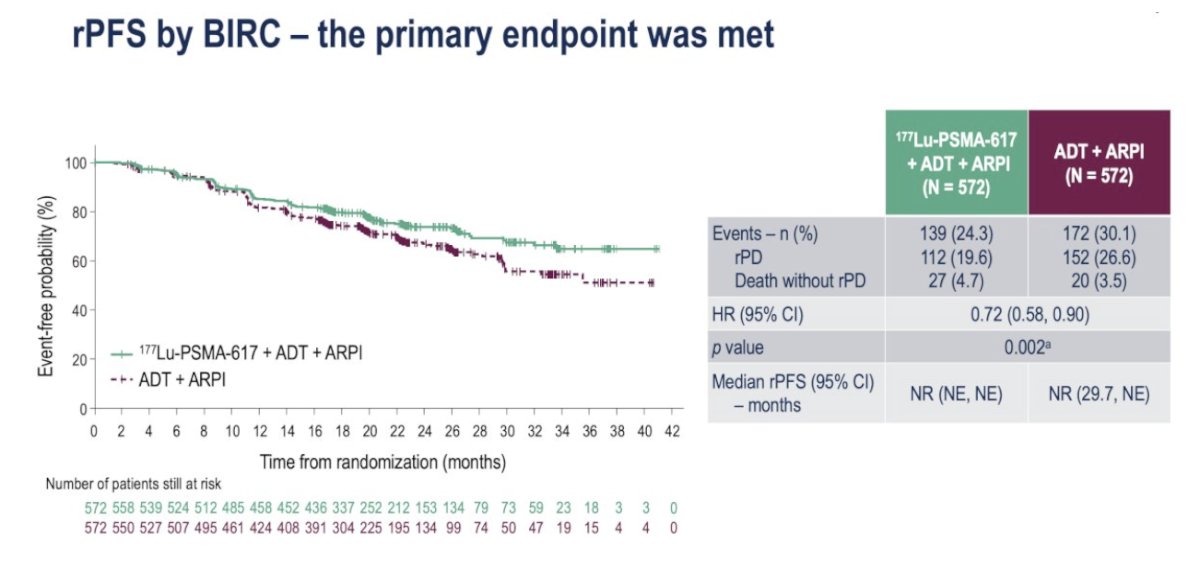
The study met its primary endpoint with radiographic progression free survival significantly prolonged with the addition of 177Lu-PSMA-617 (HR 0.72, 95% CI 0.58-0.90; p = 0.002). The median radiographic progression free survival has not been reached in either arm:
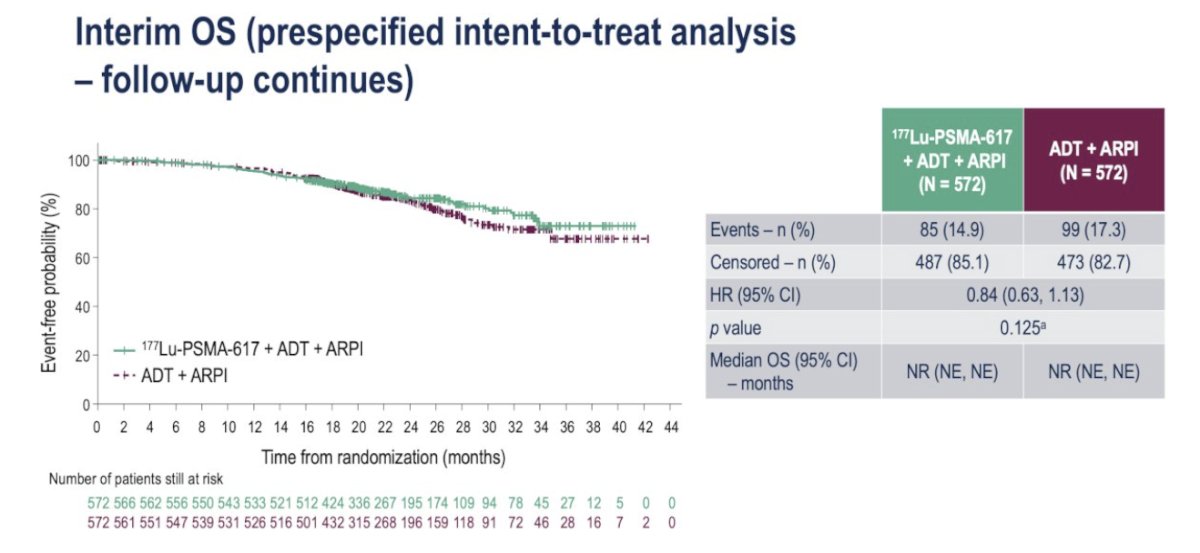
Overall survival analysis to date demonstrates a trend towards an overall survival benefit in the intervention arm (HR 0.84, 95% CI 0.64-1.13; p = 0.125):
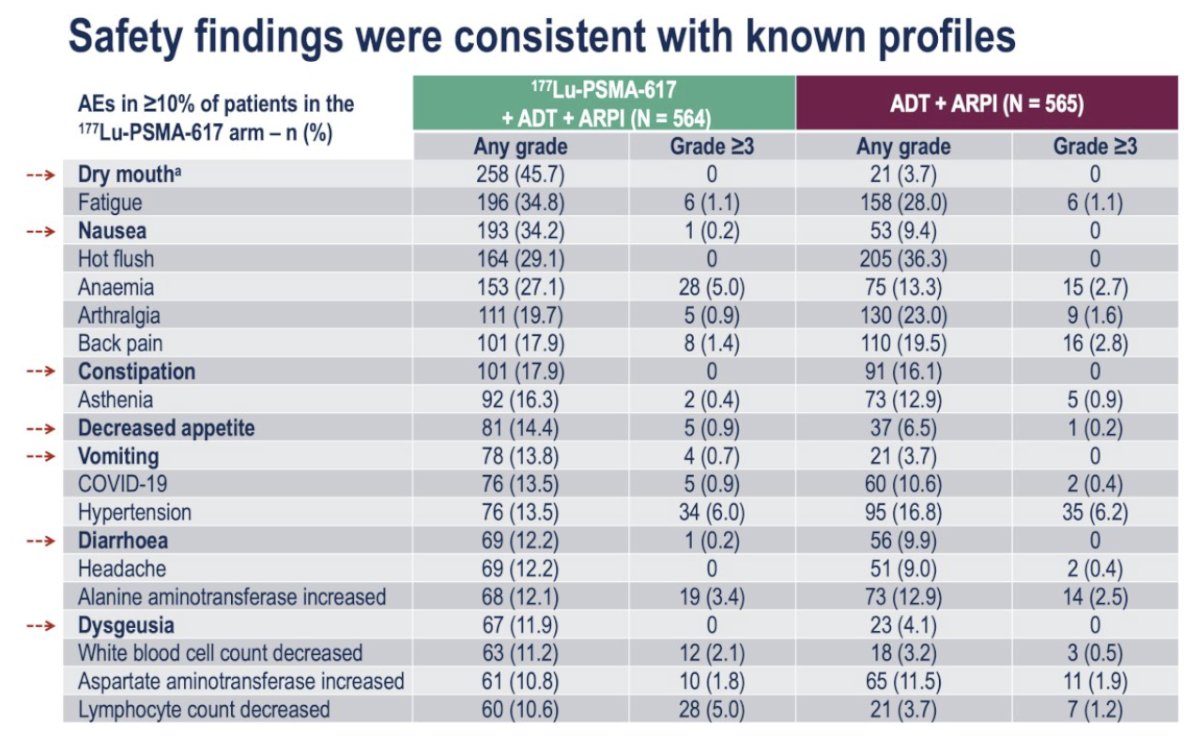
The adverse event profiles were consistent with those of 177Lu-PSMA 617 and androgen receptor pathway inhibitors. Dr. Sandhu highlighted the increased incidence of the following any-grade adverse events in the 177Lu-PSMA 617 arm:
- Dry mouth: 46% versus 4%
- Nausea: 34% versus 9%
- Constipation: 18% versus 16%
- Decreased appetite: 14% versus 6.5%
- Vomiting: 14% versus 4%
- Diarrhea: 12% versus 10%
- Dysgeusia: 12% versus 4%
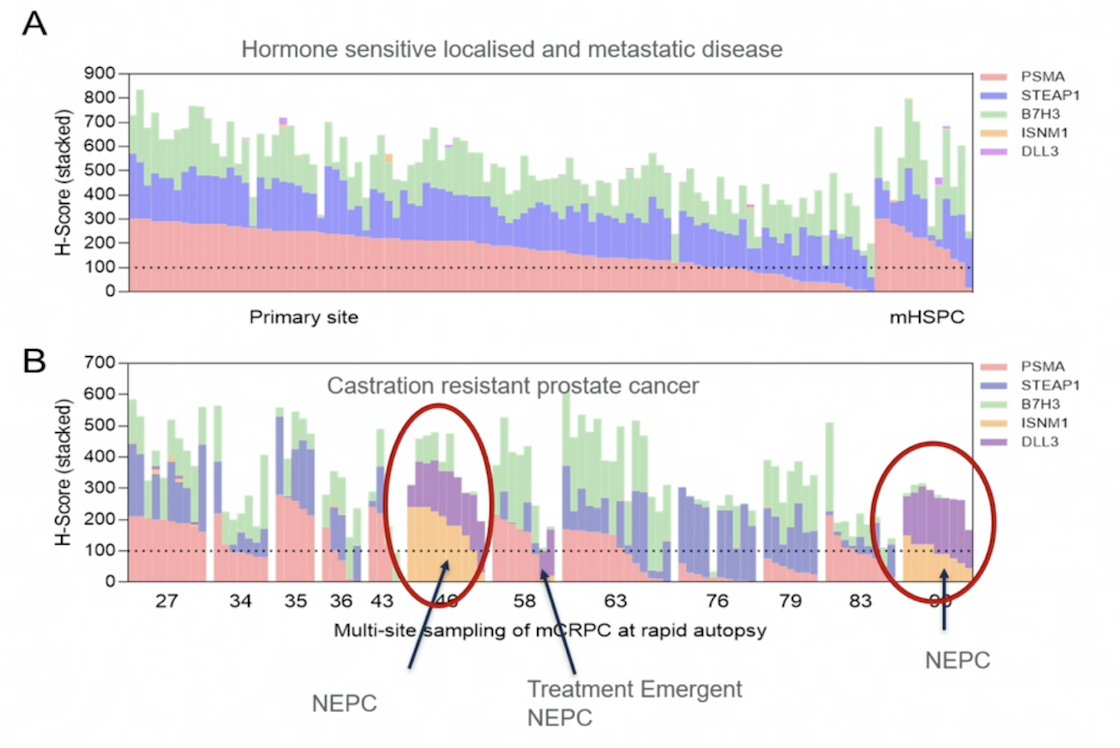
Dr. Sandhu also emphasized that leveraging tumor heterogeneity is central to improving outcomes in patients. There is a high diversity of membrane antigen positivity of specific genes (PSMA, STEAP1, B7H3), supporting the rationale for co-targeting strategies, whether in combination or sequential therapies:
Dr. Sandhu provided the following key lessons for leveraging androgen receptor signaling:
- Co-targeting the androgen receptor signaling is an effective strategy
- Beyond androgen receptor pathway inhibitors in the mCRPC space, there are new therapeutic agents likely to be: androgen receptor degraders, RIPTACs, etc
- When considering co-targeting, the following are key considerations:
- The level of expression, as there is heterogeneity across sites
- Does target expression change with the disease state (ie, mHSPC to mCRPC)? Where do we position combination therapy in the treatment paradigm?
- Target expression modulation with blockade of androgen receptor signaling (relevant for mHSPC)
- Adaptation and impact on the tumor microenvironment – currently, we are failing in this field, as it is not well understood
Second, Dr. Sandhu discussed leveraging DNA damage response. 177Lu-PSMA 617 delivers a payload of beta radiation to PSMA expression tumors, which primarily causes single stranded DNA breaks, repaired by PARP-dependent BER. Thus, blocking PARP could result in the conversion of DNA single stranded breaks to double stranded breaks. 177Lu-PSMA 617 in combination with olaparib leverages DNA damaging and potential immune modulating effects of radioligand therapy. The enhanced anti-tumor activity has been shown in combination with PARP inhibitors and radiotherapy, including 177Lu-DOTATATE.
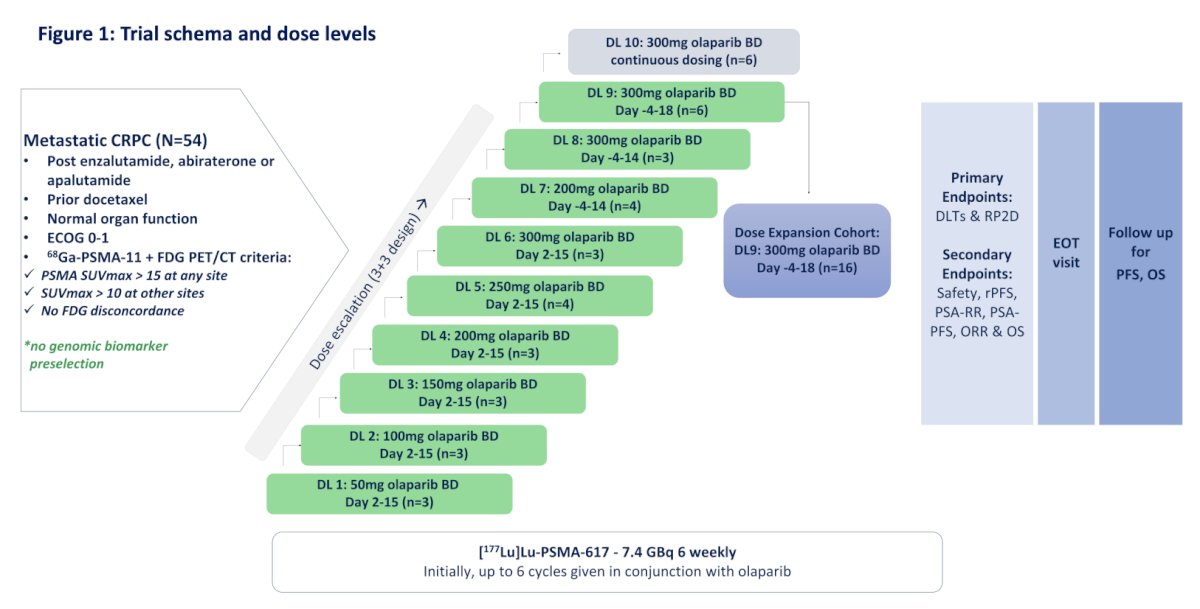
LuPARP is an investigator initiated phase 1 trial utilizing a 3+3 design for dose escalation followed by dose expansion. Between September 2019 and August 2024, 54 patients were enrolled across 2 Australian sites. Patients with mCRPC with high PSMA expression (SUVmax ≥15) without discordant FDG+ /PSMA- sites were enrolled. All patients received 177Lu-PSMA-617 7.4 GBq every 6 weeks for up to 6 cycles. Olaparib was dosed across 10 dose levels:
- Dose level 1-6: 50 mg – 300 mg BD days 2 to 15
- Dose level 7: 200 mg BD days -4 to 14
- Dose level 8: 300 mg BD days -4 to 14
- Dose level 9: 300mg BD days -4 to 18
- Dose level 10: 300 mg BD, days -4 to day 42
The primary endpoints were safety and dose limiting toxicity. Key secondary endpoints were radiological progression free survival, PSA response rate, PSA progression free survival, objective response rate, and overall survival:
Across the DL7-9 cohorts, the PSA50 response was 69% (20/29 patients), and PSA90 response was 52% (15/29):

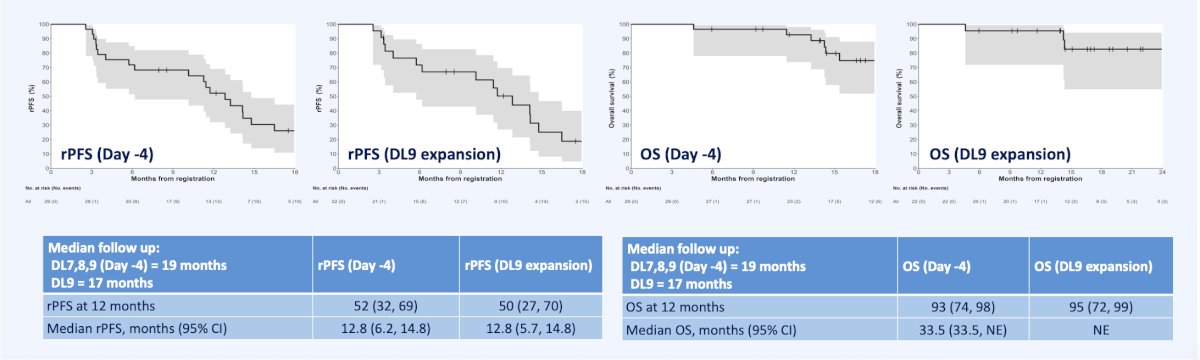
The following figure demonstrates radiographic progression free survival, and overall survival in Day – 4 and DL9 expansion:
Treatment related adverse events for DL9 expansion cohort, DL10 continuous dosing cohort, and the overall population are listed in the following table:
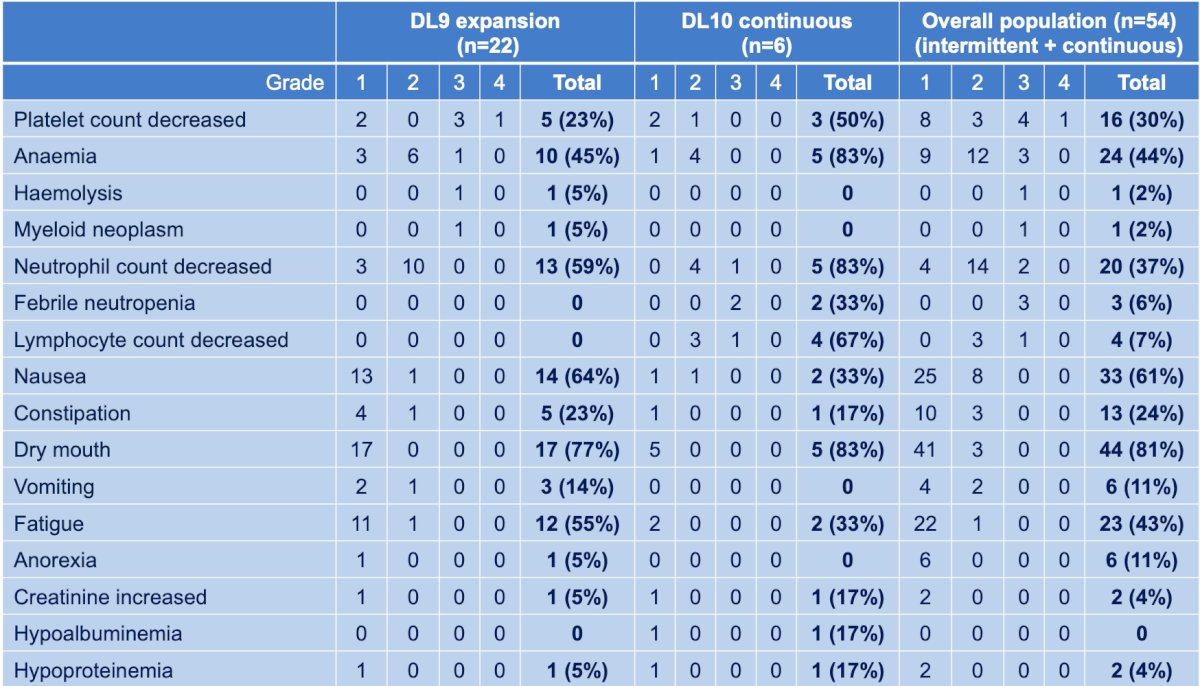
The most common treatment related adverse events of any grade included dry mouth (81%), nausea (61%), anemia (44%), fatigue (43%), neutropenia (37%), thrombocytopenia (30%). Eight patients (15%) had a grade 3 or 4 treatment related adverse events with one patient experiencing grade 4 thrombocytopenia (2%). One patient (in DL9) has a diagnosis of treatment related myelodysplastic syndrome 20 months post commencing 177Lu-PSMA-617 and olaparib.
Dr. Sandhu provided the following key lessons for leveraging DNA damage response:
- Targeting DDR to achieve radiosensitization is viable, as there is clear efficacy from the combination
- Most of the benefit is being delivered by radioligand therapy, but this may be deepened, translating into > PSA90 response, as well as progression free survival and overall survival benefits
- However, this approach does not overcome primary radioresistance
- Full blockade of DDR on Day 1 of 177Lu-PSMA-617 is important to maximally leverage DNA damage from radioligand therapy
- Continuous dosing of DDR inhibitors may not be tenable
- There is potential overlapping toxicities that need to be managed – intermittent schedule is key
- Two concepts to consider:
- For radiosensitization, non-DDR cohort - intermittent scheduling is important to maximize benefit and minimize toxicity
- For radiosensitization, HRD cohort - intermittent scheduling for inducing, followed by maintenance single agent PARP inhibitor or PARP inhibitor + androgen receptor pathway inhibitor
- We may envision triple combinations with DDR inhibitors, radioligand therapy, and immunotherapy, but scheduling will be important
Third, Dr. Sandhu discussed leveraging immunotherapy with conventional immune checkpoint inhibitors and T cell engagers. Indeed, there are several immune modulatory effects of radiation therapy, our understanding of the impact on the tumor immune microenvironment from alpha and beta radiation is limited:

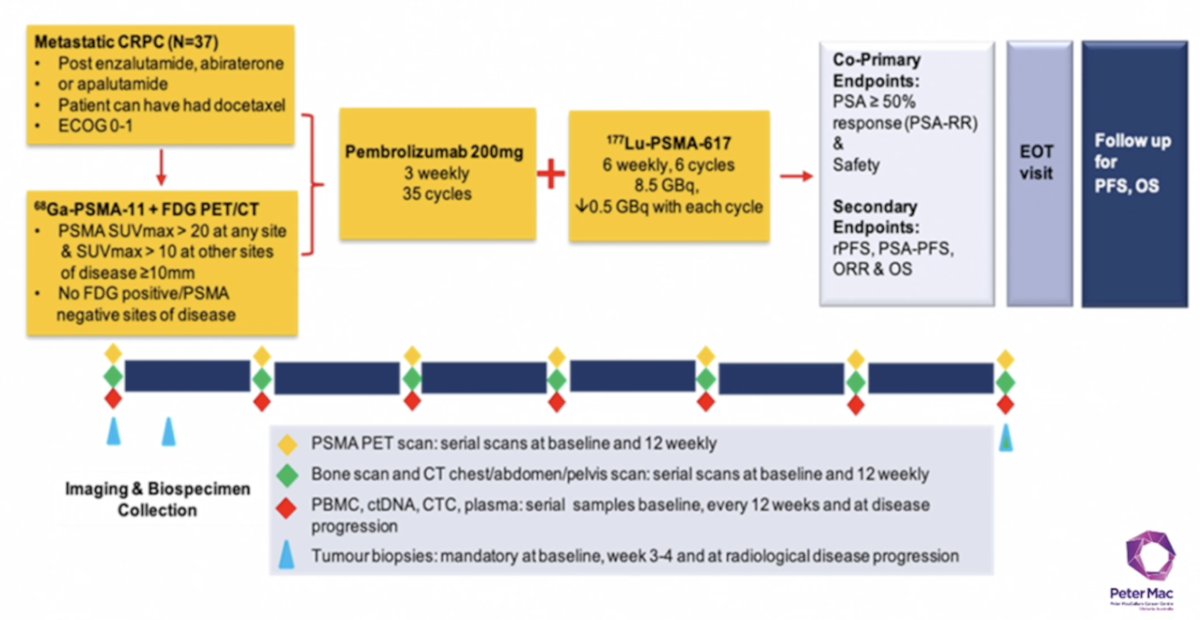
In the PRINCE phase I trial of 177Lu-PSMA-617 in combination with pembrolizumab, mCRPC patients with high PSMA expression (SUVmax ≥ 20 in an index lesion, SUVmax > 10 for all lesions ≥ 10mm), and no FDG positive/PSMA negative lesions on paired baseline PET/CT screening, received up to 6 cycles of 177Lu-PSMA-617 (starting at 8.5 GBq, reducing by 0.5 GBq with each cycle) every 6 weeks in conjunction with 200 mg of pembrolizumab every 3 weeks for up to 2 years. The study schema is as follows:
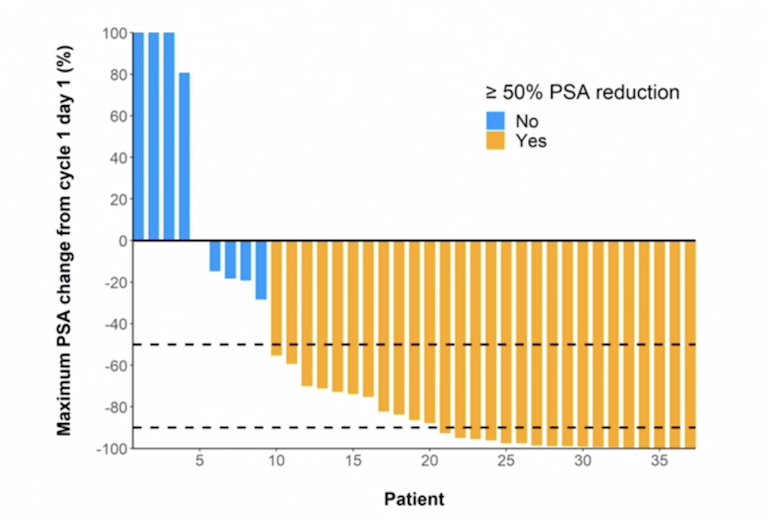
The PSA50 response was 76%, 95% CI 59-88, and the objective response rate was 70%:
The first results of the EVOLUTION trial were initially presented at ASCO 2025, assessing 177Lu-PSMA-617 with ipilimumab and nivolumab for patients with mCRPC. For this phase 2 trial, eligibility included: prior androgen receptor pathway inhibitor therapy, PSMA-positive disease, normal organ function, no contraindications to immune checkpoint inhibitors, and <= 1 line of chemotherapy. Patients were randomized (1:2) to 177Lu-PSMA-617 alone (7.4 GBq every 6 weeks, up to 6 doses) or 177Lu-PSMA-617 + induction ipilimumab (3 mg/kg every 6 weeks for 4 doses) and nivolumab (1 mg/kg every 3 weeks for 8 doses) followed by maintenance nivolumab (480 mg every 4 weeks for 18 doses) (177Lu-PSMA-617 + immune checkpoint inhibitor). The trial design of EVOLUTION is as follows:

Over a median follow-up of 18 months (IQR 16-22), PSA progression free survival at 12 months was higher in participants assigned 177Lu-PSMA-617 + immune checkpoint inhibitors than 177Lu-PSMA-617-alone (33% versus 17%; HR 0.71, 95% CI 0.43-1.19), in addition to improvement in radiographic progression free survival (47% versus 23%; HR 0.53, 95% CI 0.32-0.90):
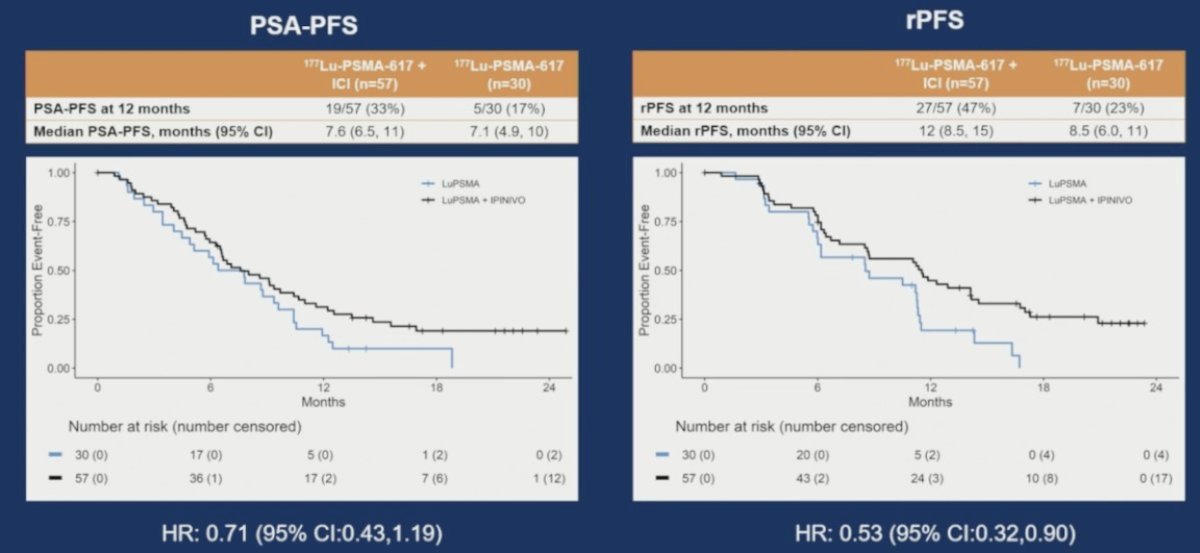
177Lu-PSMA-617 + immune checkpoint inhibitors also resulted in numerically better PSA responses, and an improvement in objective response rate (71% versus 50%) compared to 177Lu-PSMA-617 alone.
Exciting prospects in combination with radioligand therapy include T cell engagers, specifically VIR-5500 targeting PSMA and xaluritamig targeting STEAP1. Dr. Sandhu provided the following key lessons for leveraging immunotherapy with conventional immune checkpoint inhibitors and T cell engagers:
- Most of the benefit when combined with immune checkpoint inhibitors is delivered by radioligand therapy
- Immunotherapy toxicity is as anticipated, but there is no obvious overlapping toxicity with radioligand therapy (ie. renal, xerostomia)
- Alphas versus beta remains an unresolved question
- There are issues around timing of both agents that needs to be considered
- There appears to be a combination effect: improved radiographic progression free survival and overall survival landmarks, however, likely in a subset of patients
- We need to better understand predictors and weigh the risks and benefits
- Co-target tumor microenvironment is leading to a new generation of cytokines, chemokines (ie. IL12, CCR8, etc)
- Future efforts should include targeting radioligand therapy with T cell engagers, which may be highly effective. However, there are some unknowns regarding the impact of radioligand therapy on the tumor microenvironment and longer retention of T cells, but this is being actively explored
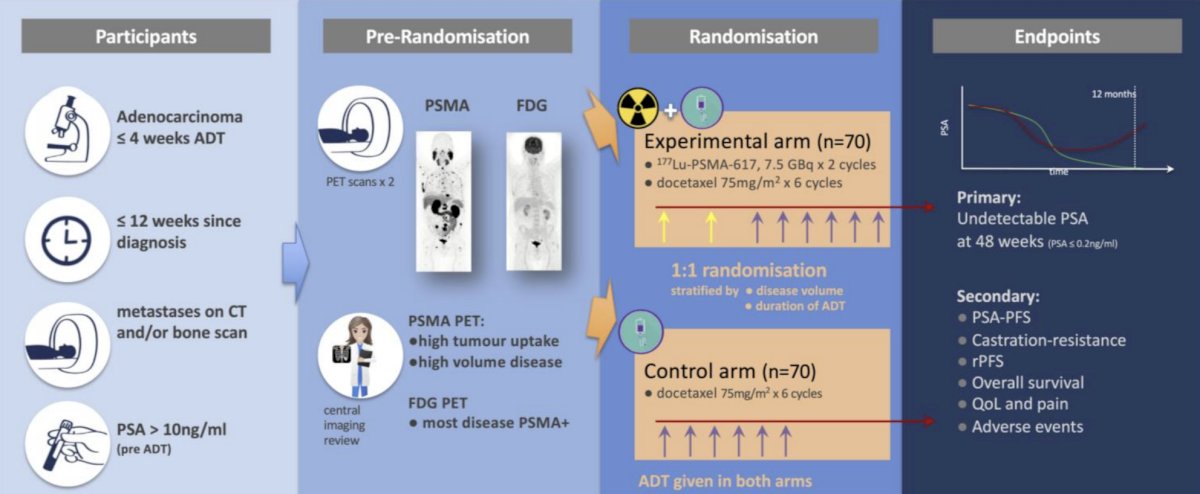
Finally, Dr. Sandhu briefly touched on leveraging radioligand therapy in combination with chemotherapy regimens. The UpFrontPSMA trial3 was published in 2024 and included patients with de novo high-volume mHSPC who had received ≤4 weeks of ADT and had a PSA >10 ng/ml at diagnosis. Prior to randomization patients underwent both PSMA and FDG PET scans. Eligibility was limited to those patients with evidence of high tumor uptake and high-volume disease on PET scans. Patients were also required to have the majority of their metastatic disease demonstrating PSMA positivity. Eligible patients were randomized to:
- Experimental arm: 177Lu-PSMA-617 7.5 GBq x 2 cycles + docetaxel 75 mg/m2 x 6 cycles
- Control arm: Docetaxel 75 mg/m2 x 6 cycles
Between May 2020 and April 2023, 130 patients were recruited and underwent randomization (experimental: 63, control: 67). All 63 patients in the experimental arm completed the two cycles of 177Lu-PSMA-617, and 79% of patients in the combination arm completed all 6 cycles of docetaxel, compared to 84% of patients in the control arm. However, a docetaxel dose reduction was required in 33% of patients in the combination arm, compared to 17% of patients in the docetaxel arm.
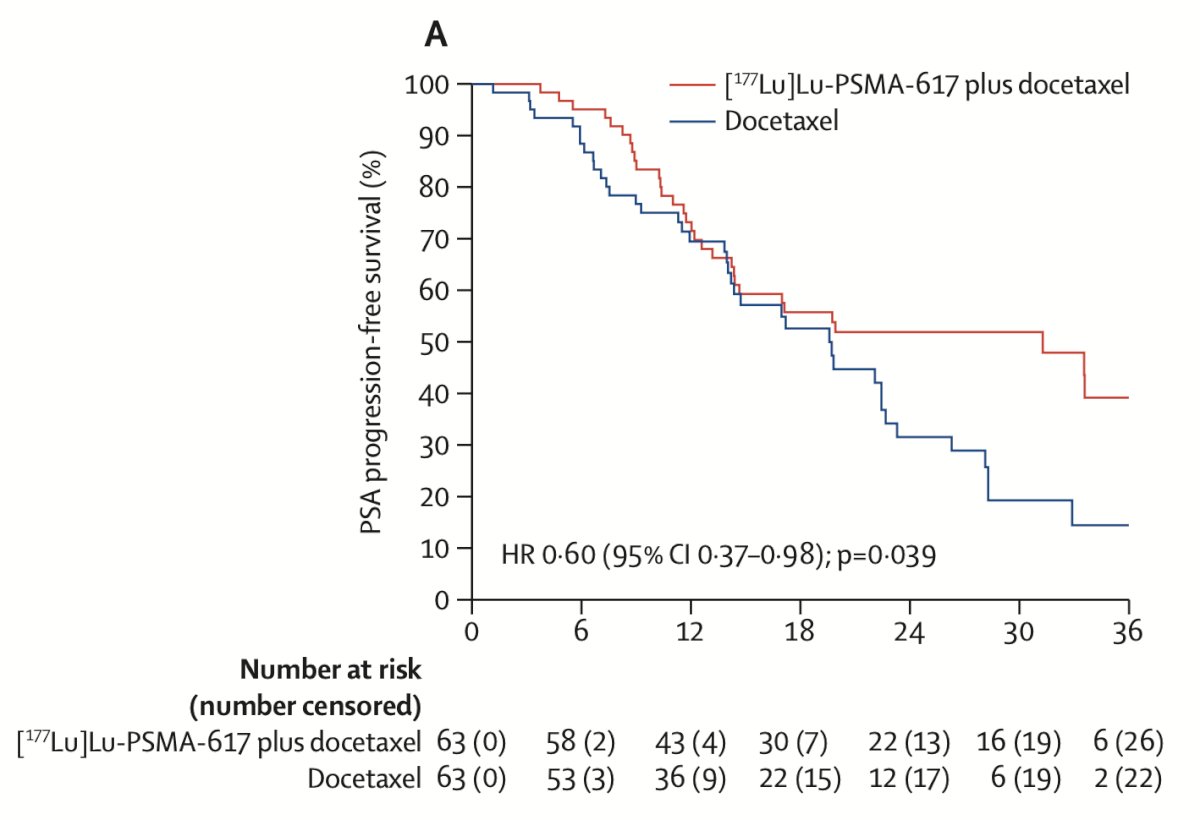
For the primary outcome, an undetectable PSA at week 48 was observed in 41% of patients in the 177Lu-PSMA-617 + docetaxel arm versus 16% of patients in the docetaxel control arm (OR 3.88, 95% CI 1.61–9.38, p = 0.002). An undetectable PSA at any point was observed in 51% and 32% of patients, respectively (OR 2.14, p = 0.042). Time-to-event analyses demonstrated that patients in the experimental arm had superior PSA progression free survival (median: 31 versus 20 months; HR 0.60, p = 0.039):
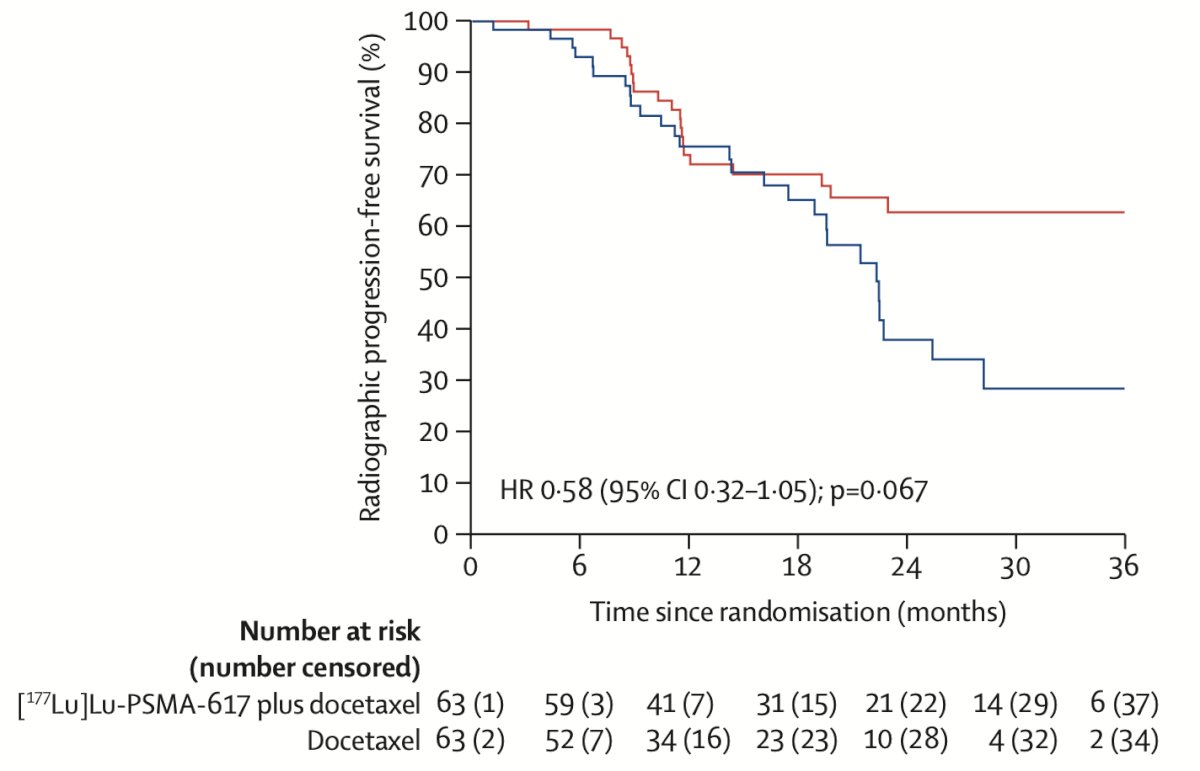
Radiographic progression free survival similarly favored 177Lu-PSMA-617 + docetaxel (HR 0.58, p = 0.067):
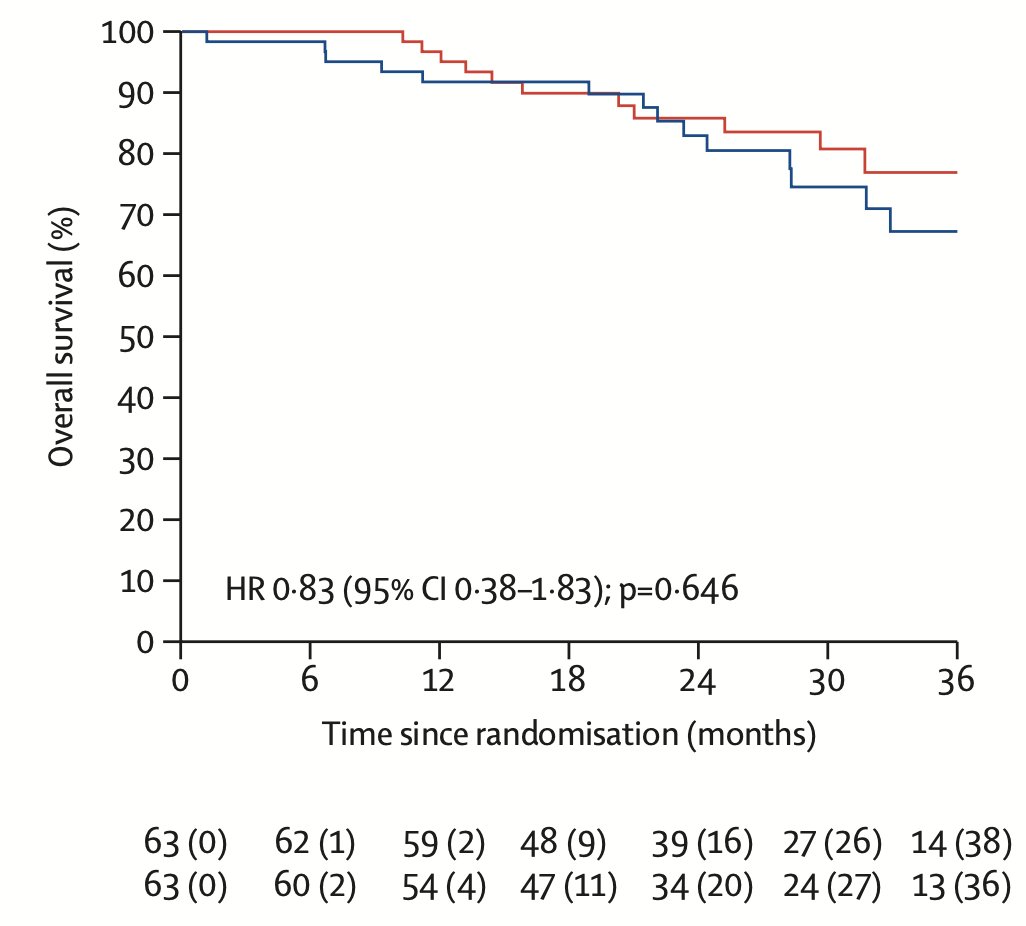
To date, there is no overall survival benefit with the addition of 177Lu-PSMA-617 to docetaxel (HR 0.83, 95% CI: 0.38–1.83, p = 0.646):
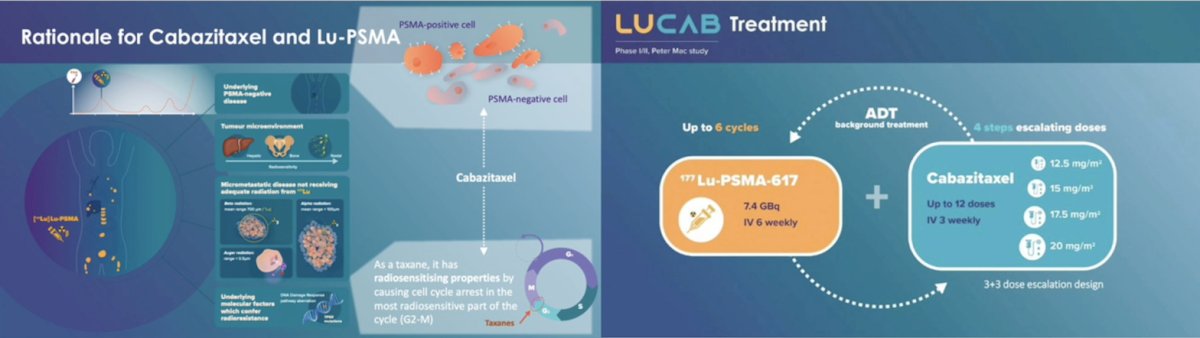
The LuCab trial will also assess the combination of 177Lu-PSMA-617 + cabazitaxel, with a primary endpoint of maximum tolerated dose and recommended phase 2 dose:
Dr. Sandhu concluded her presentation discussing lessons learned from radioligand combination therapies by highlighting key concepts to consider for rational combinations:
- Novel targets and mechanism of action combinations – durable response balanced with tolerability is the key
- Type, dose, and sequencing matters, which depend on the agents
- Positioning within the existing therapeutic paradigm
- Risk mitigation– stop early in non-responders and deep responders
- Does a new therapy impede the delivery of standard of care options?
- We need dosing schedules to mitigate toxicity
- Cumulative toxicity is important, and the need to evaluate this approach properly over the long term
- There are gaps in knowledge, such as the impact of treatment on the tumor microenvironment, that need to be interrogated in the setting of clinical trials
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 PSMA & Beyond Conference, Los Angeles, CA, Thurs, Mar 26 – Fri, Mar 27, 2026.
Related content: Lessons Learned from Radioligand Combinations "Presentation" - Shahneen Sandhu
References:
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Azad AA, Bressel M, Tan H, et al. Sequential [(177)Lu]Lu-PSMA-617 and docetaxel versus docetaxel in patients with metastatic hormone sensitive prostate cancer (UpFrontPSMA): A multicentre, open label, randomized, phase 2 study. Lancet Oncol. 2024 Oct;25(10):1267-1276.