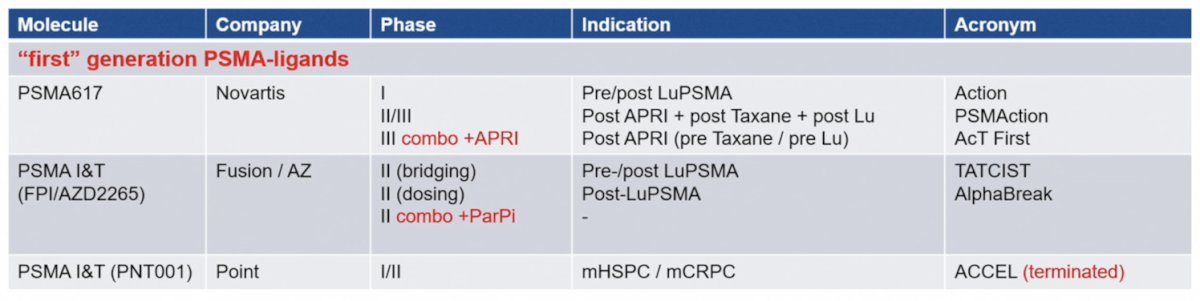
(UroToday.com) The 2026 PSMA and Beyond conference featured a new radioligands and radionuclides session and presentation by Dr. Matthias Eiber discussing Ac-PSMA. Over the last 10 years, we have seen multiple retrospective case series, including meta analyses, in more than 1,000 patients, as well as phase I-III trials initiated, but to date there has been no Ac-PSMA agent approved. The following table highlights the development status of Ac-PSMA radioligand therapy, including the PSMAction, AcT First, and AlphaBreak trials:
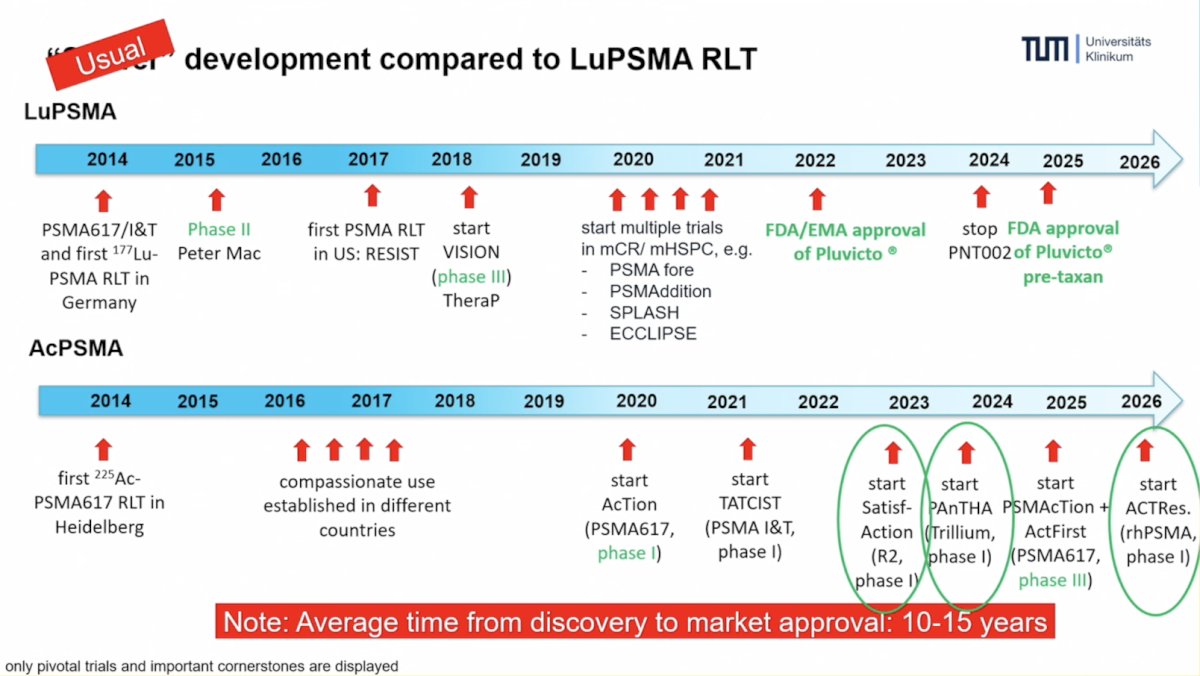
Whereas it may appear that Ac-PSMA has had a slower development trajectory compared to Lu-PSMA radioligand therapy, Dr. Eiber notes that the average time from discovery to market approval is 10-15 years, and therefore he considers the Ac-PSMA development as a usual/normal pace:
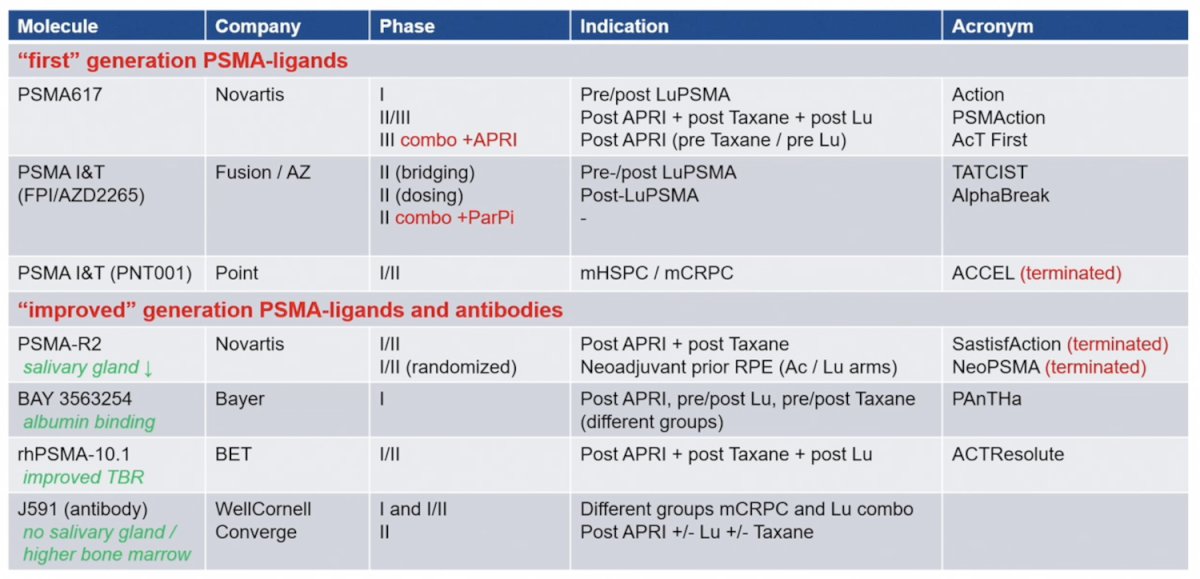
An improved generation of PSMA-ligands and antibodies includes BAY 3563254 (PAnTHa trial) and rhPSMA-10.2 (ACTResolute trial), as highlighted in the following table:
In 2024, 225Ac-PSMA-617 was assessed in the retrospective multicenter WARMTH Act study1, specifically 488 patients at 7 centers (South Africa, Germany, India, Australia). 225Ac-PSMA-617 was associated with a median overall survival of 15.5 months and median progression free survival of 7.9 months. Any PSA decline was noted in 73% of patients and PSA50 response was noted in 57% of patients:

Toxicity across this study and the collective literature of 225Ac-PSMA-617 is driven largely by xerostomia, with an any grade adverse event rate of ~80-85%, albeit with rarely reporting of grade 3+ xerostomia. The hematologic toxicity profile is reasonable, with rates of grade 3-4 adverse events <15%. The following is a case example of xerostomia after 177Lu-PSMA and 225Ac-PSMA-617 radioligand therapy:

Unfortunately, for salivary gland toxicity, there are limited strategies to mitigate side effects. The salivary glands are a highly vascularized organ, with limited regenerative potential, especially serous excretion, which is vulnerable to radiation (mainly the parotid gland). Additionally, PSMA’s high affinity for glutamate may drive high accumulations of ligands (versus antibodies). Can dosimetry inform and guide development? The following table highlights difference agents, their mean kidney dose, mean salivary dose, and mean reported tumor dose:

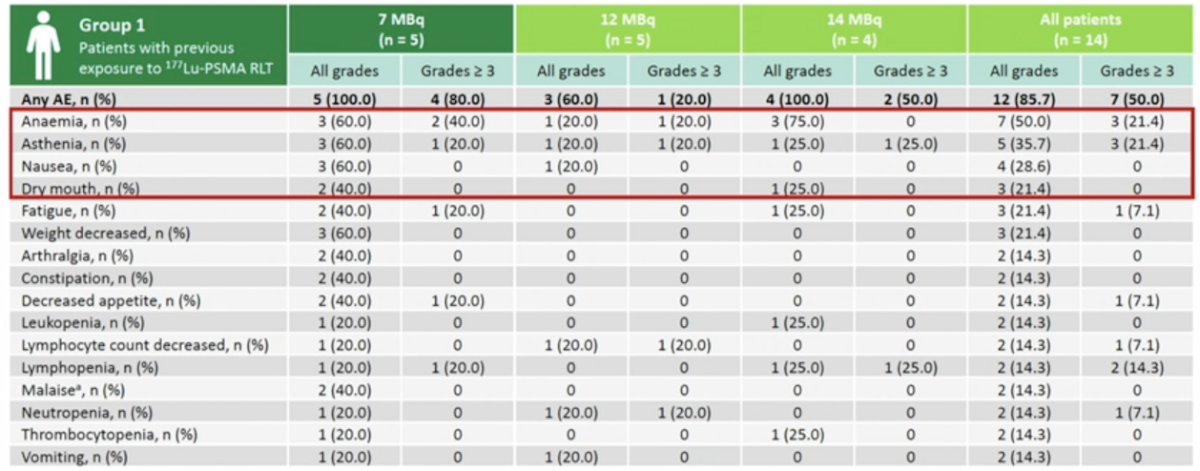
Newer agents, such as 225Ac-PSMA-R2, appear to have lower salivary gland uptake. Preliminary data from the phase I/II SatisfAction open label, multi-center study of 225Ac-PSMA-R2 in men with mCRPC with or without prior 177Lu-labelled PSMA-targeted radioligand therapy, showed no grade 3+ xerostomia adverse events, and reasonable all grade xerostomia events:
However, as of December 2025, development of 225Ac-PSMA-R2 has been stopped given the aforementioned xerostomia rates in SatisfAction, and high rates of xerostomia in the WARMTH Act study.
With regards to 225Ac-rhPSMA-10.1, this agent has been assessed in a phase I trial, with notable high tumor uptake and a long effective half-life of 91 hours. This trial also had low salivary gland exposure (0.130 Gy/GBq versus 0.63 Gy/GBq in the VISION substudy). 225Ac-rhPSMA-10.1 is also being explored in the ACTResolute phase I trial at University College London in heavily pre-treated mCRPC post 177-Lu-PSMA patients. The first patient is expected to enter the study in April 2026.
There are also several combination trials assessing several therapeutics with 225Ac-PSMA:

The initial optimism for potentially overcoming beta resistance and the notable anti-tumor effect of 225Ac-PSMA has been tempered by xerostomia substantially impairing quality of life. Dr. Eiber hopes that we can find a plateau of productivity for 225Ac-PSMA:

Dr. Eiber concluded his presentation discussing Ac-PSMA with the following take-home points:
- 225Ac-PSMA is the “real world” of drug development
- Despite challenges, there are many active players in the field:
- Novartis: life cycle strategy post-Pluvicto
- Fusion/AstraZeneca: PSMA-I&T platform
- Phase III trials may lead to approvals, with the impact on quality of life to be determined
- Early clinical entry with new ligands and other antibodies are being investigated (ie. Bayer)
- Adapted strategies should include (i) ligand engineering to optimize gland uptake, and (ii) finding the ideal combinations to reduce the 225Ac-PSMA dose
- Success will probably not be determined by the most potent drug, but by the optimal therapeutic window
Presented by: Matthias Eiber, MD, PhD, Technische Universität München, Munich, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 PSMA & Beyond Conference, Los Angeles, CA, Thurs, Mar 26 – Fri, Mar 27, 2026.
Related content: Ac-PSMA: The Truth Should be Told! "Presentation" - Matthias Eiber
References: