(UroToday.com) The 2026 PSMA & Beyond conference featured a PSMA PET session and presentation by Dr. Lisa Bodei discussing SPECT versus PET and optimizing response biomarkers. There are several reasons why response biomarkers are now of critical relevance:
- There has been an expansion of PSMA theranostics
- An inadequacy of current response criteria (RECIST – bone disease, PCWG3)
- A need for early response assessment
- Important as predictors for stratifying patients
- Limitations of PSA
- PSMA molecular imaging is emerging as the primary biomarker
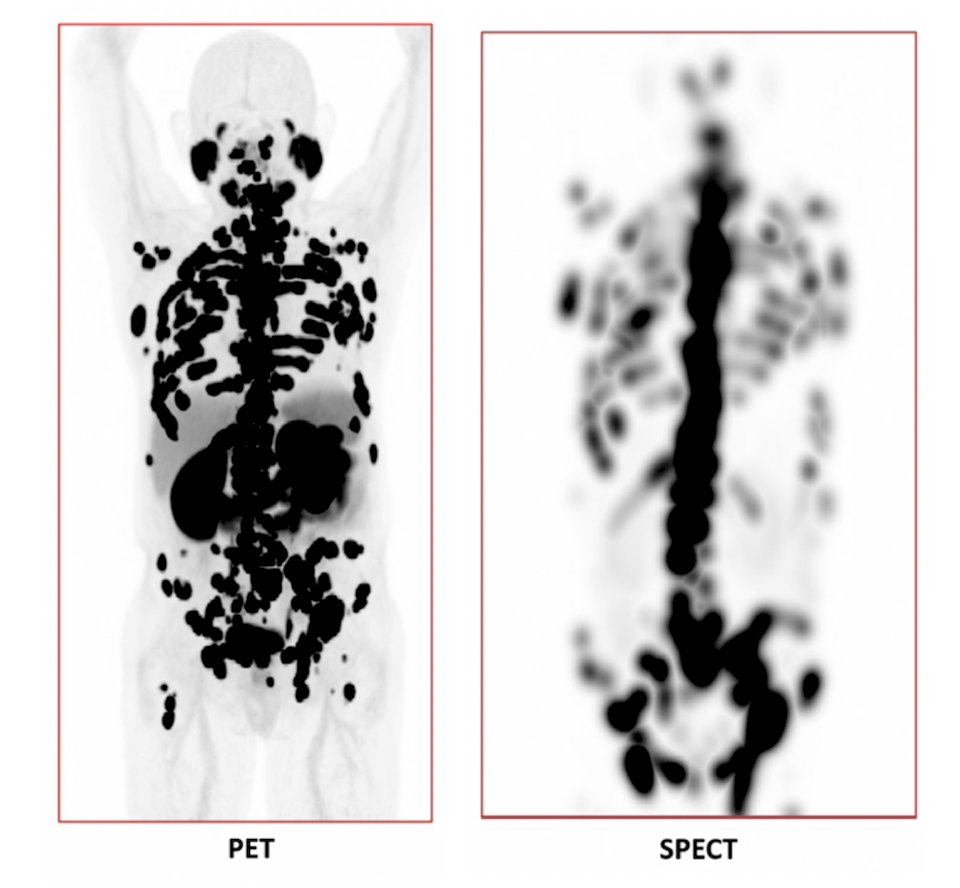
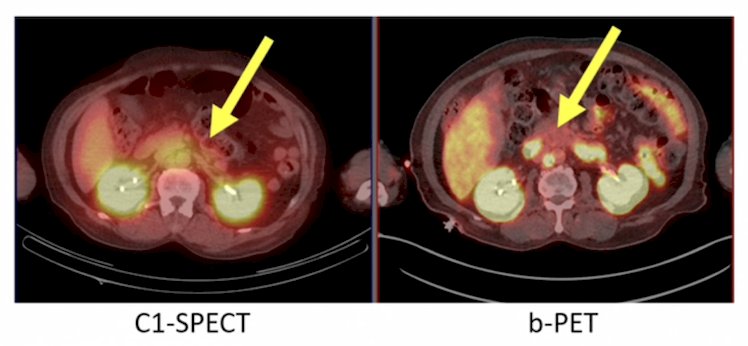
Dr. Bodei notes that there are differences between PET versus SPECT. PET has high sensitivity and is a biological signal, whereas SPECT is therapy linked and used in dosimetry. SPECT also informs therapy delivery, and both modalities inform disease biology:
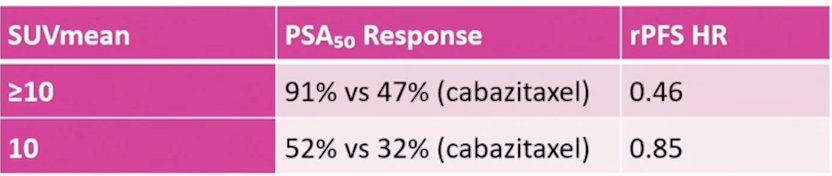
What we are currently measuring is SUV (SUVmax, SUVmean), tumor volume, total lesions PSMA, and absorbed dose to assess if these metrics correlate with overall survival, progression free survival, and PSA response. Dr. Bodei emphasized that this represents a shift to whole-body metrics. Several studies have assessed the predictive threshold of baseline PSMA PET SUVmean. In the TheraP trial,1 an SUVmean >= 10 was considered the gold standard cutoff and correlated with PSA50 response and radiographic progression free survival:
In the VISION trial,2 patients with the highest SUVmean quartile (>= 10.2) had a radiographic progression free survival of 14.1 months and overall survival of 21.4 months, compared to the lowest SUVmean quartile (6.0) with a radiographic progression free survival of 5.8 months and overall survival of 14.5 months. In a U.S. Expanded Access program (n = 88),3 baseline total tumor SUVmean had an AUC of 0.81 for PSA50 response, and was an independent predictor of PSA progression free survival (HR 0.58) and overall survival (HR 0.54).
Studies have also looked at PET volume as a baseline predictive threshold. In the TheraP trial,1 FDG-PET MTV >= 200mL was associated with PSA response (38% < 200 mL versus 56%), radiographic progression free survival (HR 1.79; p = 0.0008), and was the only independent overall survival predictor across all treatments. Other PSMA PET volume metrics include:4
- Total lesion PSMA: the tumor volume x SUVmean is a predictor of overall survival (HR 1.04)
- Total lesion quotient: TV / SUVmean has the highest C index for overall survival (0.658)
- High volume + low PSMA expression are associated with the worst prognosis
Dr. Bodei provided the following key messages for PET versus SPECT:
- SPECT is acquired during therapy workflow (no extra tracer per visit)
- A cycle 2 SPECT + PSA has a Cohen kappa = 0.93 for agreement with PET-based RECIP 1.0
- Similar overall survival prediction between the two modalities (C-index 0.63 versus 0.58, p = 0.055)
- PET is superior to SPECT for progression free survival prediction (C-index 0.66 versus 0.57, p < 0.001)
Thus, Dr. Bodei emphasized that 177Lu-PSMA SPECT/CT offers a practical, cost effective alternative with a comparable overall survival prognostication.
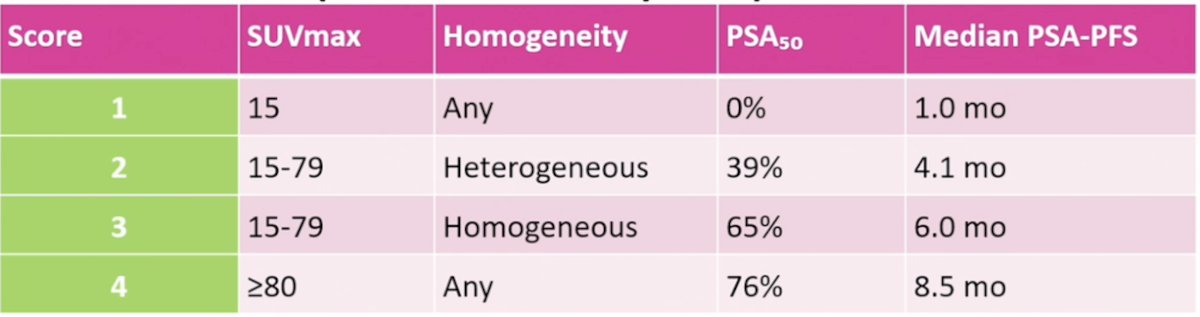
On treatment response thresholds have been proposed for PSMA PET, including the change in total lesion PSMA: -30% versus +30%.5 This cutpoint has been associated with an optimal discrimination for partial response, stable disease, and progressive disease, with significant overall survival separation across all categories. Additionally, the cutpoint was superior to PSA change or new metastases alone. The visual HIT score (no software required) was also recently published,6 assessing the prognostic value of cycle 1 SPECT SUVmean, noting the following PSA50 responses and PSA progression free survival outcomes:
On treatment response threshold for SPECT after cycle 2 of 177Lu-PSMA SPECT/CT is summarized by the following points:
- Any increase in SPECT total tumor volume predicts shorter progression free survival:
- PSA progression free survival: 3.7 versus 6.7 months (HR 2.5; p = 0.0008)
- LuPIN trial: HR 4.1 (p = 0.006)
- RECIP 1.0 applied to SPECT (>= 20% total tumor volume increase + new lesion):
- Reduced PSA progression free survival: HR 3.6 (p = 0.001)
- Reduced overall survival: HR 3.1 (p = 0.001)
- C-index for PSA progression free survival: 0.80; overall survival: 0.78
- New bone lesions (first to last cycle):
- Strongest overall survival predictor: HR 2.85 (p = 0.01)
- Overall survival stratification: 19.7, 14.4, and 6.9 months
Additionally, a cycle 1 SPECT SUVmean independently predicts PSA50 response (OR 17.1) and PSA progression free survival (HR 0.17).
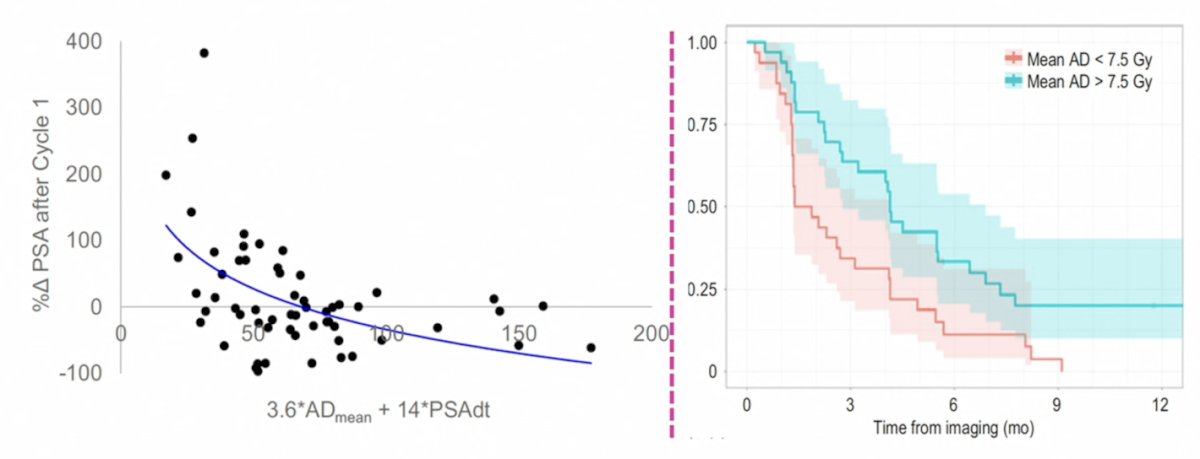
With regards to dose-response relationships, Dr. Bodei highlighted a study by Grkovski et al.7 that showed baseline PET and SPECT lesion SUVmax were strongly correlated (Pearson r, 0.74; n = 1,364 lesions). Patients receiving a higher mean absorbed dose (>7.5 Gy) had a significantly better PSA response (median 70% versus -5%; p < 0.001) and longer biochemical progression free survival (median 4.1 months versus 1.6 months; p = 0.005) compared with patients whose mean absorbed dose was less than 7.5 Gy, respectively:
When considering when to use SPECT versus PET before and during radioligand therapy, Dr. Bodei suggests that SPECT is acceptable/preferred in (i) high volume disease and PSA > 5 ng/mL (no staging difference versus PET), and (ii) during 177Lu-PSMA therapy (acquired as part of the work flow). PET is strongly preferred in (i) small lymph nodes (4 mm) when SPECT resolution is limited, and (ii) 177Lu-PSMA-617 eligibility determination (NCCN or trial validated):
Dr. Bodei concluded her presentation discussing SPECT versus PET and optimizing response biomarkers with the following take-home points:
- Baseline patient selection is critical:
- PSMA PET SUVmean ≥10 is the most robust prospectively validated threshold for Lu-PSMA candidacy (higher PSA response, longer radiographic progression free survival, and overall survival)
- FDG-PET MTV ≥200 mL or high PSMA volume identifies poor prognosis regardless of treatment
- Whole-body PET metrics (total lesion-PSMA, total lesion quotient) outperform lesion-based or PSA-only assessment:
- RECIP 1.0 (PET) at 12 weeks: gold standard (overall survival: 21.7 versus 8.3 months)
- SPECT total tumor volume change at cycle 2: practical alternative to predict PSA progression free survival and overall survival
- PET and SPECT are complementary, not competing, evaluation tools
- Dosimetry refines imaging-based response:
- Lesion absorbed dose and early SPECT/PET changes identify responders and non-responders beyond PSA and morphology, supporting dose–response driven treatment adaptation
- Genomic biomarkers clarify heterogeneity and resistance (emerging)
- Experience from neuroendocrine tumors and evolving data in neuroendocrine prostate cancer suggest that lineage plasticity and genomic programs modulate PSMA expression, radiosensitivity, and resistance—necessitating integrated imaging + dosimetry + genomic models
Presented by: Lisa Bodei, MD, PhD, Memorial Sloan Kettering, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 PSMA & Beyond Conference, Los Angeles, CA, Thurs, Mar 26 – Fri, Mar 27, 2026.
Related content: SPECT Versus PET: Optimizing Response Biomarkers "Presentation" - Lisa Bodei
References:
- Buteau JP, Martin AJ, Emmett L, et al. PSMA and FDG-PET as predictive and prognostic biomarkers in patients given [177Lu]Lu-PSMA-617 versus cabazitaxel for metastatic castration-resistant prostate cancer (TheraP): A biomarker analysis from a randomized, open-label, phase 2 trial. Lancet Oncol. 2022 Nov;23(11):1389-1397.
- Kuo P, Hesterman J, Rahbar K, et al. [68Ga]Ga-PSMA-11 PET baseline imaging as a prognostic tool for clinical outcomes to [177Lu]Lu-PSMA-617 in patients with mCRPC: A VISION substudy. J Clin Oncol. 2022;40(16):5002.
- Kimura K, Murthy V, Voter AF, et al. PSMA PET/CT-Derived indicators and outcomes after [177Lu]Lu-PSMA-617: A multicenter retrospective analysis from the U.S. Expanded-Access Program. J Nucl Med. 2026 Feb 12 [Epub ahead of print].
- Kiani I, Siri MA, Babaei M, et al. Quantitative PSMA PET biomarkers for predicting response to 177Lu-PSMA therapy in prostate cancer: A systematic review and meta-analysis. J Nucl Med. 2026 Feb 26 [Epub ahead of print].
- Gafita A, Rauscher I, Weber M, et al. Novel framework for treatment response evaluation using PSMA PET/CT in patients with metastatic castration-resistant prostate cancer (RECIP 1.0): An International multicenter study. J Nucl Med. 2022 Nov;63(11):1651-1658.
- Ghodsi A, Demirci RA, Gulati R, et al. Prognostic value of cycle 1 SPECT SUVmean in patients with metastatic castration-resistant prostate cancer treated with 177Lu-PSMA-617. J Nucl Med. 2026 Mar 12 [Epub ahead of print].
- Grkovski M, Krebs SS, O’Donoghue JA, et al. Lesion absorbed dose-response relationship in patients with metastatic castration-resistant prostate cancer undergoing [177Lu]Lu-PSMA-617 radiopharmaceutical therapy. J Nucl Med. 2025 Oct 1;66(10):1622-1630.