(UroToday.com) The 2026 PSMA & Beyond conference featured a clinical trial updates session and presentation by Dr. Oliver Sartor discussing the PSMAddition trial. The PSMAddition trial randomized men with untreated or minimally treated mHSPC and ≥1 PSMA-positive metastatic lesion on 68Ga-PSMA-11 PET/CT to the experimental arm of 177Lu-PSMA 617 (7.4 GBq ±10% 6 cycles every 6 weeks) + ADT + androgen receptor pathway inhibitor versus the control arm of ADT + androgen receptor pathway inhibitor. Of note, crossover to the 177Lu-PSMA 617 arm was permitted upon radiographic progression:
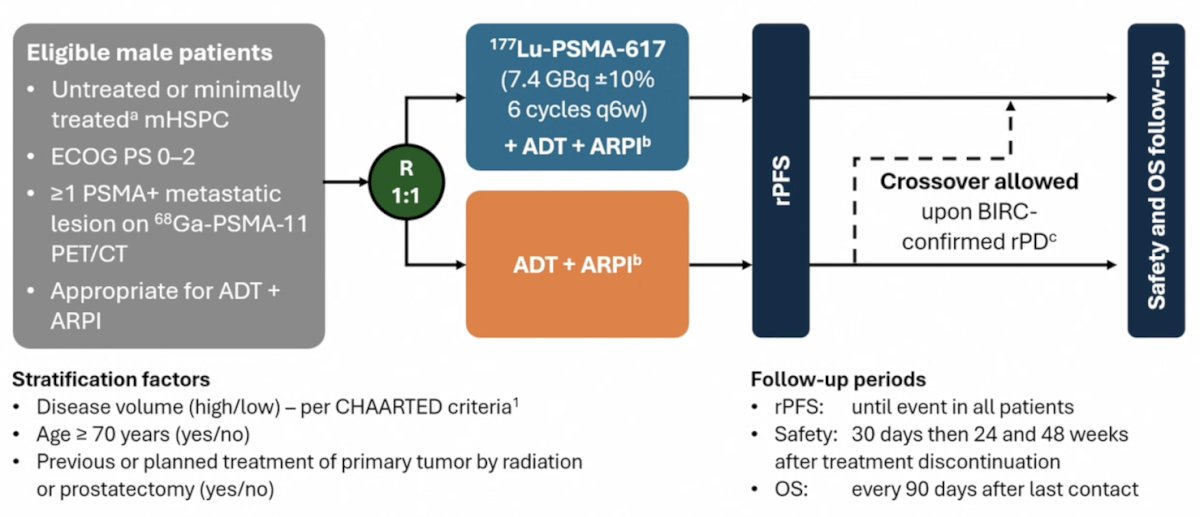
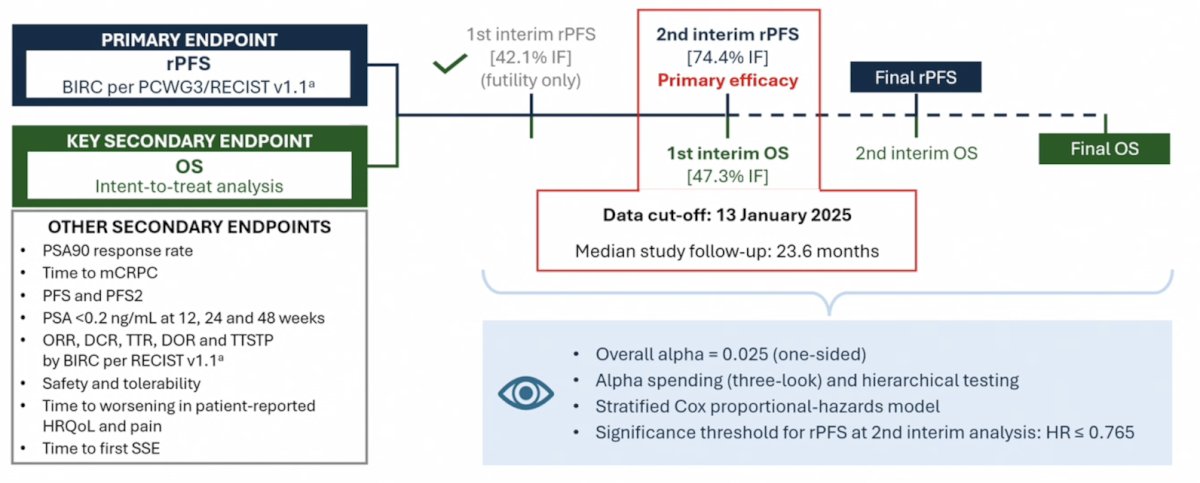
The primary study endpoint was radiographic progression free survival, assessed via blinded central review using the PCWG3/RECIST v1.1 criteria. The key secondary endpoint was overall survival, with other endpoints including:
- PSA90 response rate
- Time to castration resistance
- Progression free survival and progression free survival 2
- PSA <0.2 ng/ml at 12, 24, and 38 weeks
- Safety and tolerability
The study cut-off date for this analysis was January 13, 2025, and the median study follow-up was 23.6 months. The data presented represents the second interim analysis of radiographic progression free survival (data maturity: 74.4%) and the first interim analysis of overall survival (data maturity: 47.3%).
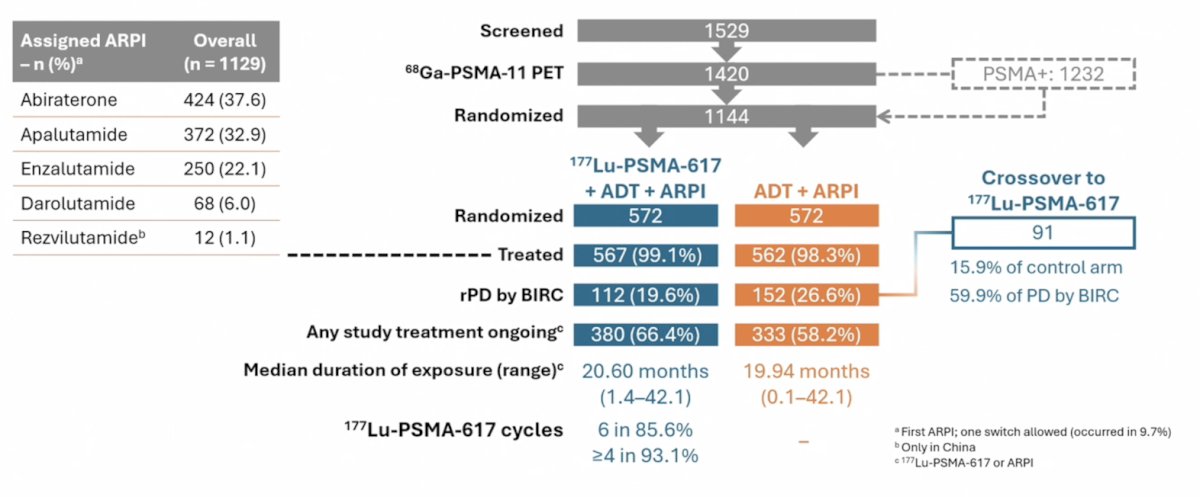
The study flow chart is summarized below. Overall, 1,144 patients were randomized 1:1 to the 177Lu-PSMA 617 + ADT + androgen receptor pathway inhibitor and ADT + androgen receptor pathway inhibitor arms, respectively (n = 572 for each arm). The assigned androgen receptor pathway inhibitor was most commonly abiraterone acetate (37.6%), followed by apalutamide (33%) and enzalutamide (22%). Radiographic progressive disease was observed in 19.6% and 26.6% of patients in the experimental and control arms, respectively. Crossover to the 177Lu-PSMA 617 arm was observed in 16% of patients in the control arm. In the experimental arm, 86% of patients received all 6 cycles, and 93% received ≥4 cycles:
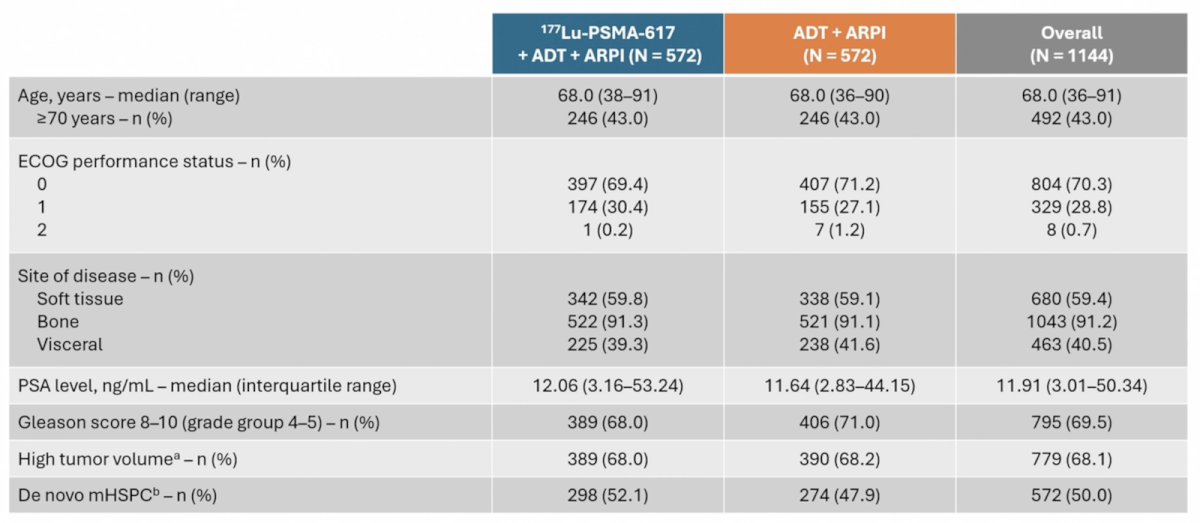
The baseline characteristics are summarized in the following table. The median patient age was 68 years, 91% of patients had bone metastases, and 41% had visceral metastases. The median PSA at study entry was 11.9 ng/ml, 68% of patients had high-volume disease, and 50% had de novo mHSPC:
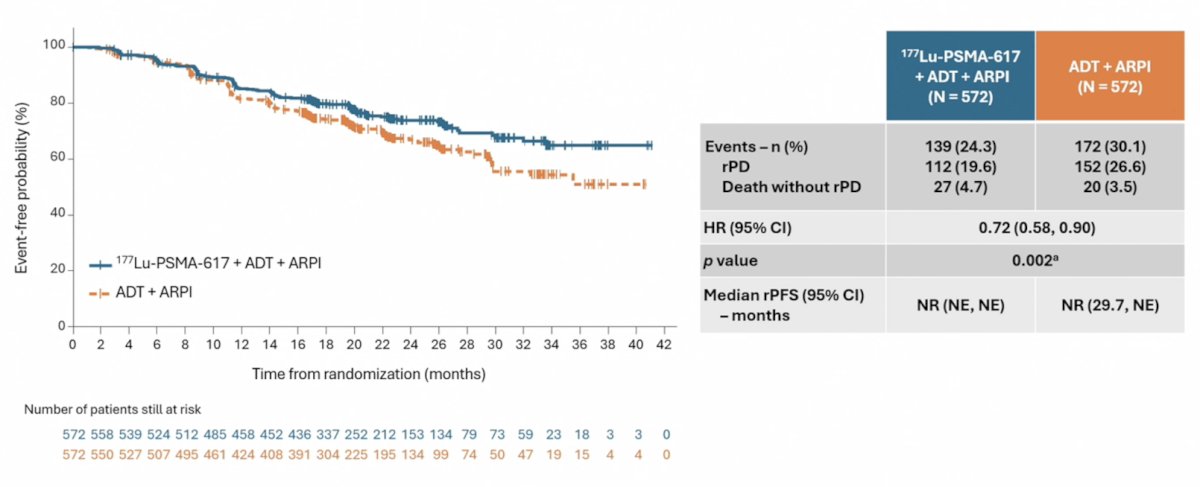
The study met its primary endpoint with radiographic progression free survival significantly prolonged with the addition of 177Lu-PSMA-617 (HR 0.72, 95% CI 0.58-0.90; p = 0.002). The median radiographic progression free survival has not been reached in either arm:
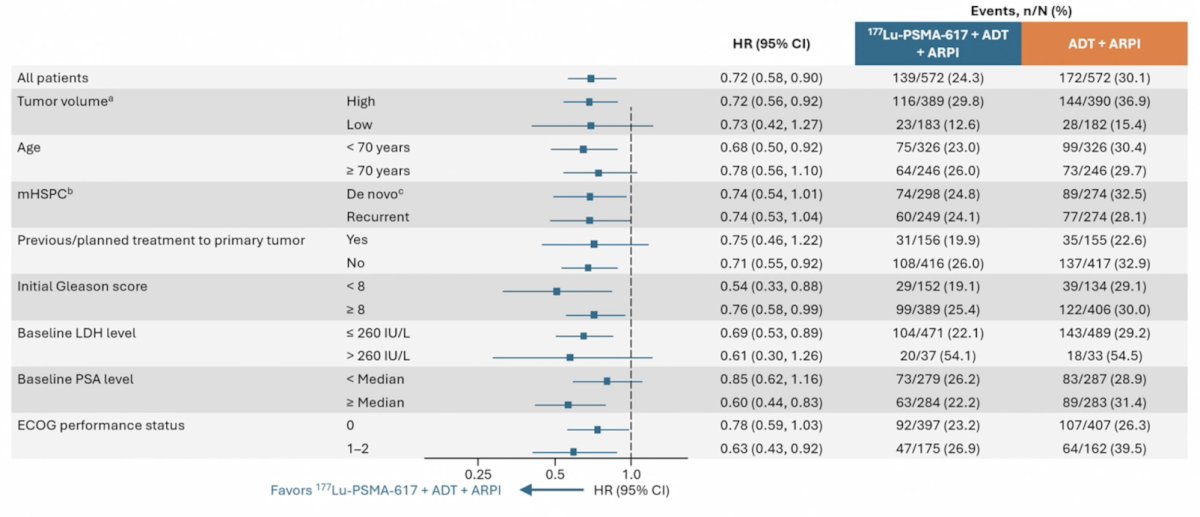
The radiographic progression free survival benefit in favor of 177Lu-PSMA-617 addition was consistent across all evaluable subgroups:
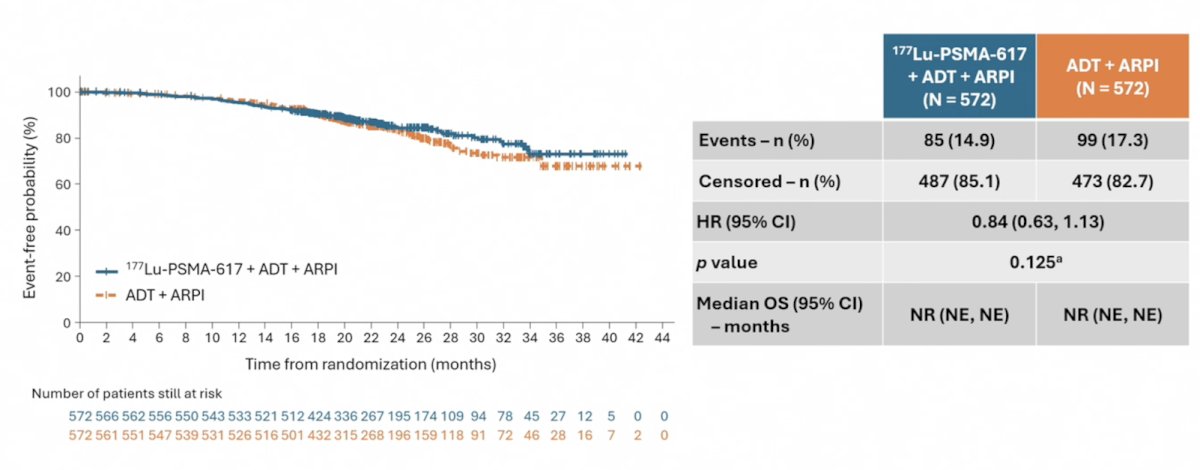
Overall survival analysis to date demonstrates a trend towards an overall survival benefit in the intervention arm (HR 0.84, 95% CI 0.64-1.13; p = 0.125):
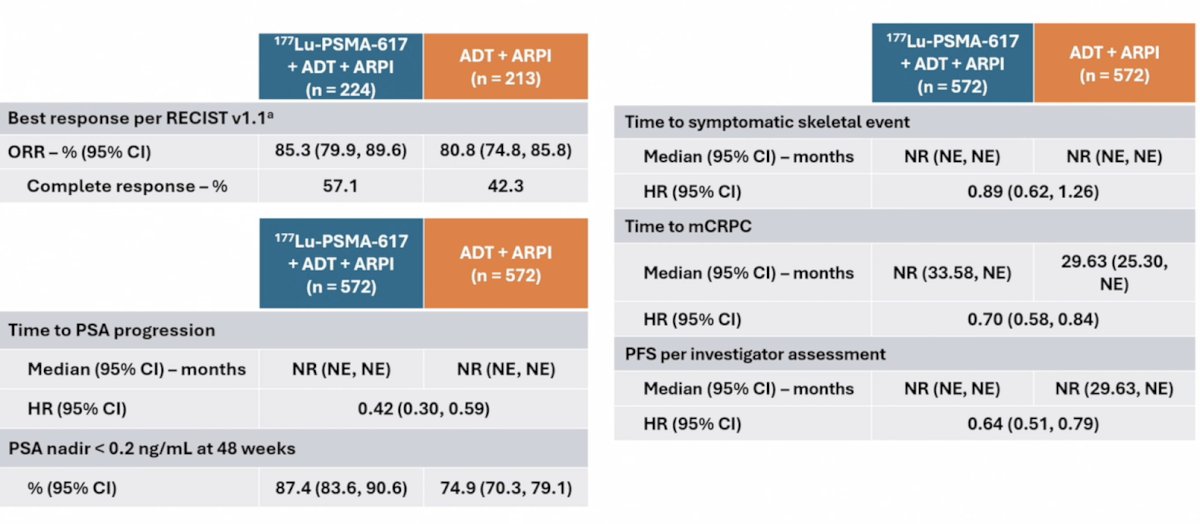
Other key secondary endpoints similarly favored the intervention arm:
- Objective response rate: 85% versus 81%
- Complete response: 57% versus 42%
- Time to PSA progression: HR 0.42, 95% CI 0.30-0.59
- PSA nadir <0.2 ng/ml at 48 weeks: 87% versus 75%
- Time to symptomatic skeletal event: HR 0.89, 95% CI 0.62-1.26
- Time to mCRPC: HR 0.70, 95% CI 0.58-0.84
- Progression free survival per investigator assessment: HR 0.64, 95% CI 0.51-0.79
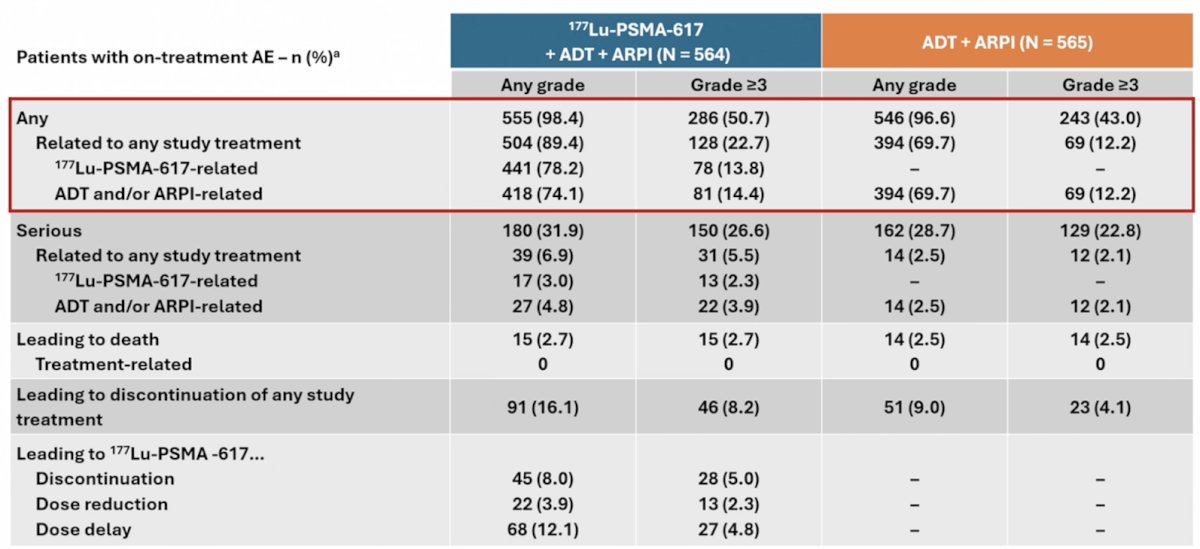
Any adverse event was observed in 98.4% and 96.6% of patients in the experimental and control arms, respectively. Grade ≥3 events were observed in 51% and 43%, respectively. Serious adverse events related to any study treatment were observed in 6.9% and 2.5% of patients, respectively (Grade ≥3: 5.5% versus 2.1%):
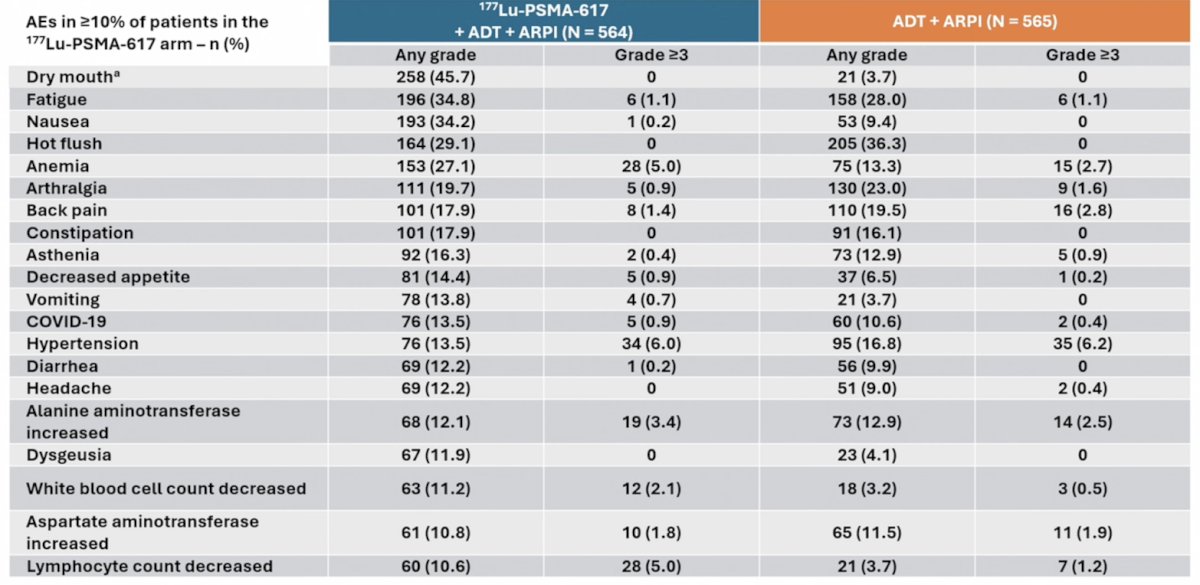
The adverse event profiles were consistent with those of 177Lu-PSMA 617 and androgen receptor pathway inhibitors. Dr. Sartor highlighted the increased incidences of the following any-grade adverse events in the 177Lu-PSMA 617 arm:
- Dry mouth: 46% versus 4%
- Nausea: 34% versus 9%
- Constipation: 18% versus 16%
- Decreased appetite: 14% versus 6.5%
- Vomiting: 14% versus 4%
- Diarrhea: 12% versus 10%
- Dysgeusia: 12% versus 4%
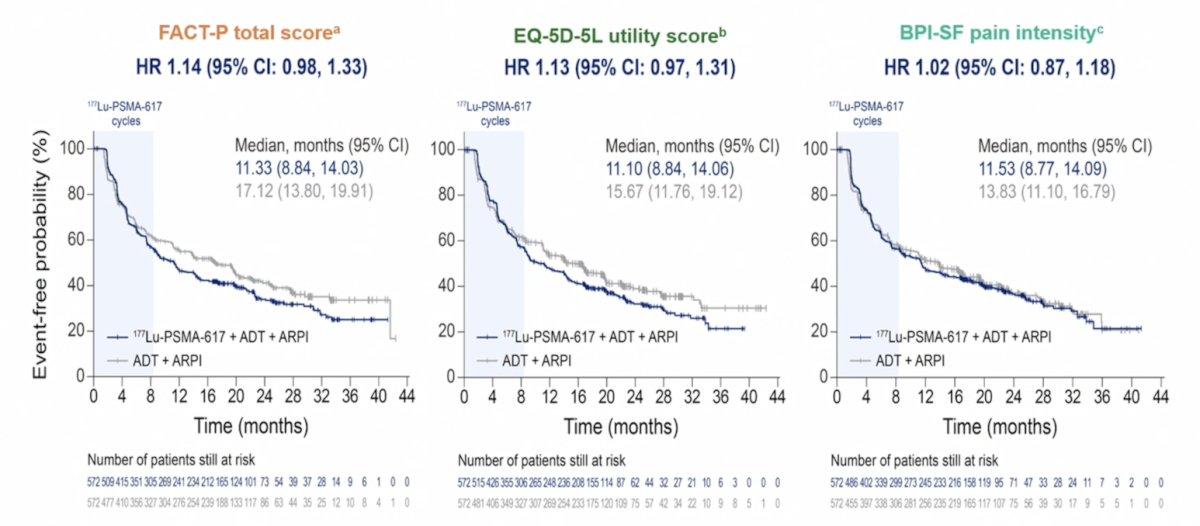
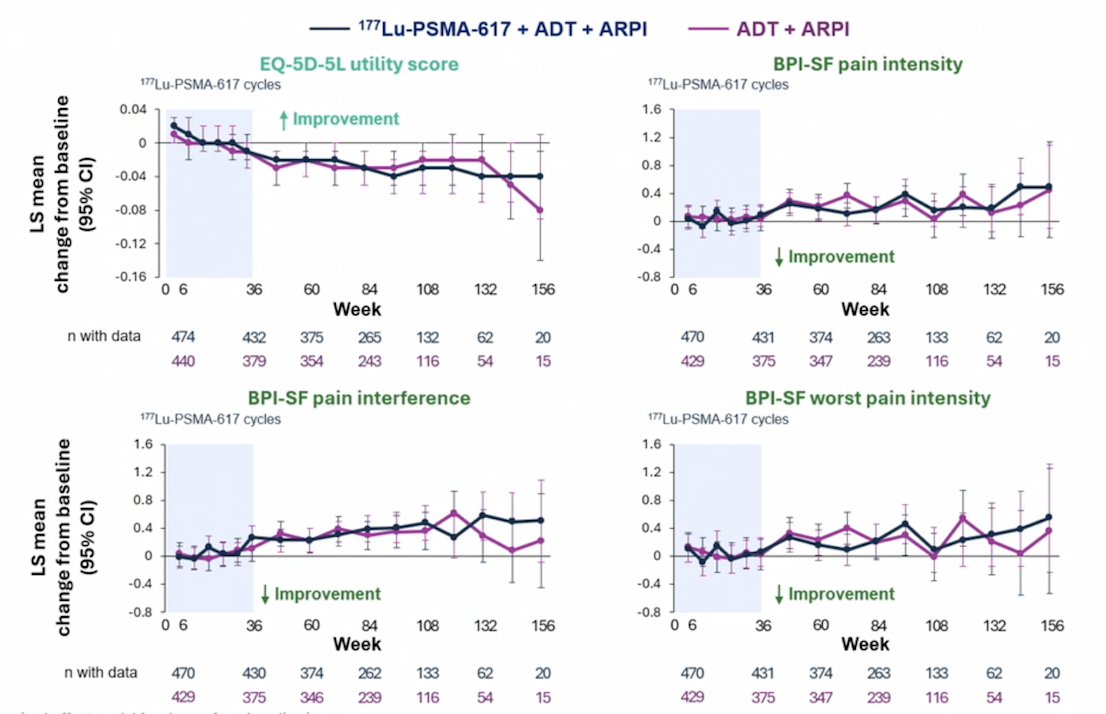
With regards to health related quality of life and pain, there were 1,144 patients randomized, with a median study treatment exposure of 20.6 months in the 177Lu-PSMA-617 arm and 19.94 months in the control arm. Hazard ratios for time to worsening in all FACT-P, EQ-5D-5L, and BPI-SF scales/subscales were >1.0 but <1.2, and all 95% CIs included 1.0 (177Lu-PSMA-617 arm versus control arm):
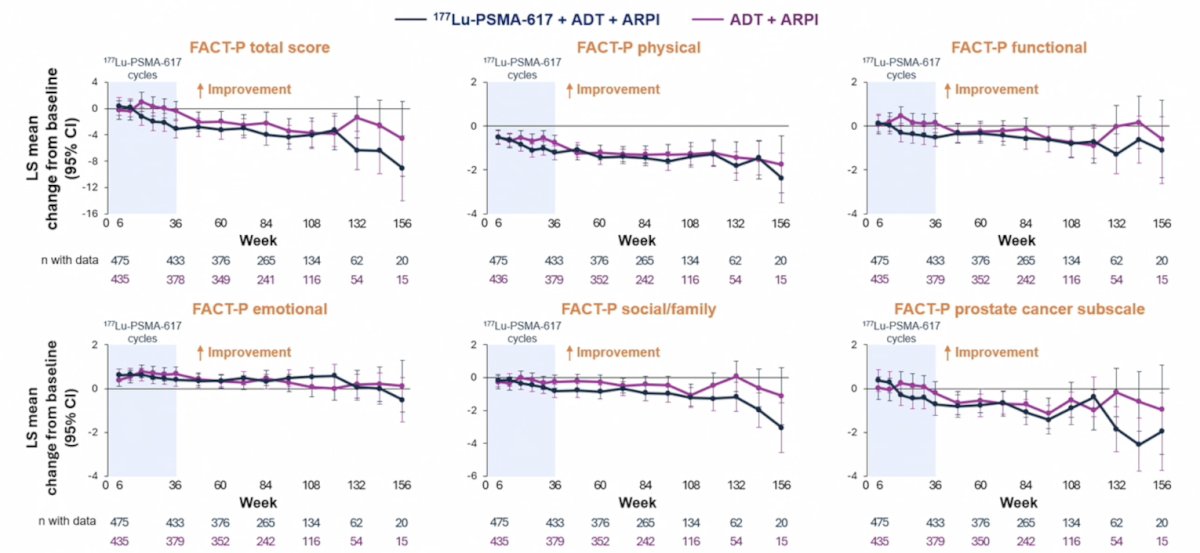
The longitudinal assessment of change from baseline for FACT-P total score and the sub-domains is highlighted in the following figure:
Finally, the longitudinal assessment of change from baseline is noted in the following figures:
Dr. Sartor concluded his presentation discussing the PSMAddition trial at the second interim analysis with the following take-home points:
- 177Lu-PSMA-617 with ADT + androgen receptor pathway inhibitor led to a statistically significant improvement in radiographic progression free survival versus ADT + androgen receptor pathway inhibitor
- There was a positive trend in overall survival, and follow-up for mature data is needed and ongoing
- PSA declines, complete responses, and time to mCRPC results favored the 177Lu-PSMA-617 combination
- Safety findings indicate no unexpected concerns from ADT + 177Lu-PSMA-617 + androgen receptor pathway inhibitor
- Adverse events were more frequent in the 177Lu-PSMA-617 combination arm, most commonly dry mouth, fatigue, and nausea
Presented by: Oliver Sartor, MD, East Jefferson General Hospital Cancer Center, New Orleans, LA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 PSMA & Beyond Conference, Los Angeles, CA, Thurs, Mar 26 – Fri, Mar 27, 2026.
Related content: PSMAddition "Presentation" - Oliver Sartor